Alveolar bone height according to the anatomical relationship between the maxillary molar and sinus
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, Yonsei University College of Dentistry, Seoul, Korea. sshan@yuhs.ac
- 2Department of Periodontics, Research Institute for Periodontal Regeneration, Yonsei University College of Dentistry, Seoul, Korea.
- KMID: 2470829
- DOI: http://doi.org/10.5051/jpis.2020.50.1.38
Abstract
- PURPOSE
The aim of this study was to investigate the available alveolar bone height between the maxillary molars and the sinus floor according to their anatomical relationship using cone-beam computed tomographic (CBCT) images.
METHODS
A total of 752 maxillary first (M1) and second molars (M2) on CBCT scans of 188 patients were selected. First, each maxillary molar was categorized as type 1, 2, 3, or 4 according to the relationship of the molar root with the maxillary sinus floor. The frequency distribution of each type was analyzed. Second, the shortest vertical distance (VD) of each molar was measured from the furcation midpoints of the roots to the lowest point of the sinus floor by 2 observers. Intraclass correlation coefficients and the t-test were calculated for the VD measurements.
RESULTS
For M1, type 3 was the most frequent, followed by type 2. For M2, type 3 was the most common, followed by type 1. The VD measurements of type 1 were 9.51±3.68 mm and 8.07±2.73 mm for M1 and M2, and those of type 3 were 3.70±1.52 mm and 4.03±1.53 mm for M1 and M2, respectively. The VD measurements of M2 were significantly higher in female patients than in male patients.
CONCLUSIONS
Type 3 was the most frequent anatomical relationship in the maxillary molars, and showed the lowest alveolar bone height. This information will help clinicians to prevent complications related to the maxillary sinus during maxillary molar treatment and to predict the available bone height for immediate implant planning.
MeSH Terms
Figure
-
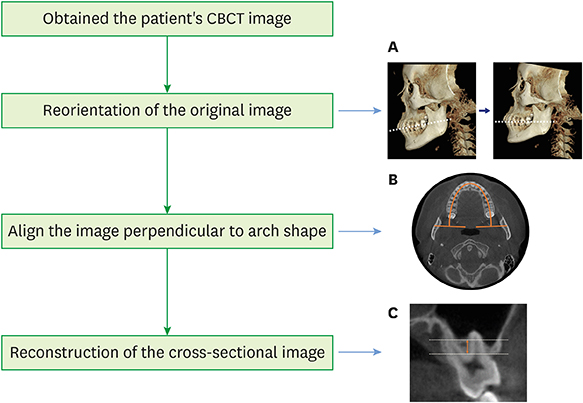
Figure 1 Overall flowchart of image reconstruction for reproducible measurements of the available alveolar bone height. (A) The occlusal plane of the original data was reoriented to be parallel to the base plane. (B) The CBCT image was aligned to be perpendicular to the arch shape at the cervical level of the maxillary molars. (C) Reconstruction of the cross-sectional image. CBCT: cone-beam computed tomography.
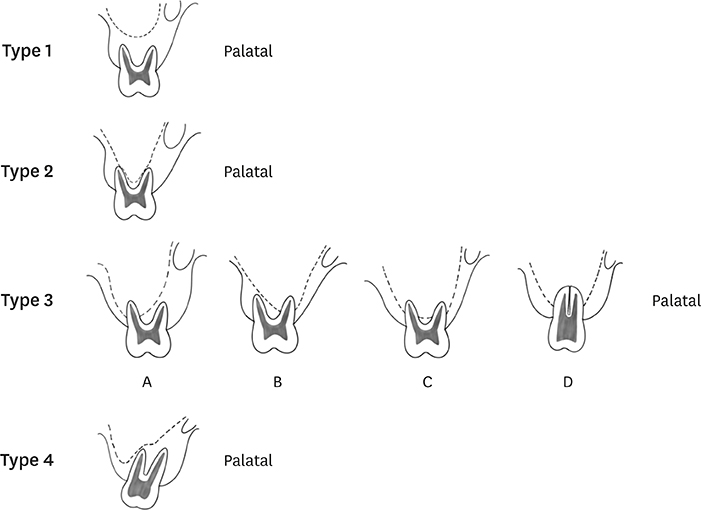
Figure 2 Illustrations of the classification of the relationship between the maxillary molars and the sinus floor.

Figure 3 Measurement of the shortest vertical distance from the furcation midpoint of the maxillary molar to the sinus floor.

Figure 4 The frequency distribution of the classification in the maxillary first molars (A) and second molars (B).
Reference
-
1. Som PM, Curtin HD. Head and neck imaging. 5th ed. St. Louis (MO): Mosby;2003.2. van den Bergh JP, ten Bruggenkate CM, Disch FJ, Tuinzing DB. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000; 11:256–265.
Article3. Tavelli L, Borgonovo AE, Re D, Maiorana C. Sinus presurgical evaluation: a literature review and a new classification proposal. Minerva Stomatol. 2017; 66:115–131.
Article4. Wagner F, Dvorak G, Nemec S, Pietschmann P, Traxler H, Schicho K, et al. Morphometric analysis of sinus depth in the posterior maxilla and proposal of a novel classification. Sci Rep. 2017; 7:45397.
Article5. Jung YH, Cho BH. Assessment of the relationship between the maxillary molars and adjacent structures using cone beam computed tomography. Imaging Sci Dent. 2012; 42:219–224.
Article6. Tian XM, Qian L, Xin XZ, Wei B, Gong Y. An analysis of the proximity of maxillary posterior teeth to the maxillary sinus using cone-beam computed tomography. J Endod. 2016; 42:371–377.
Article7. Kwak HH, Park HD, Yoon HR, Kang MK, Koh KS, Kim HJ. Topographic anatomy of the inferior wall of the maxillary sinus in Koreans. Int J Oral Maxillofac Surg. 2004; 33:382–388.
Article8. Howe RB. First molar radicular bone near the maxillary sinus: a comparison of CBCT analysis and gross anatomic dissection for small bony measurement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:264–269.
Article9. Sharan A, Madjar D. Correlation between maxillary sinus floor topography and related root position of posterior teeth using panoramic and cross-sectional computed tomography imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:375–381.
Article10. Lee SM, Lee SS, Huh KH, Yi WJ, Heo MS, Choi SC. The effects of location of alveolar crest on the vertical bone heights on panoramic radiographs. Dentomaxillofac Radiol. 2012; 41:117–121.
Article11. Liang XH, Kim YM, Cho IH. Residual bone height measured by panoramic radiography in older edentulous Korean patients. J Adv Prosthodont. 2014; 6:53–59.
Article12. Liu H, Liu R, Wang M, Yang J. Immediate implant placement combined with maxillary sinus floor elevation utilizing the transalveolar approach and nonsubmerged healing for failing teeth in the maxillary molar area: A randomized controlled trial clinical study with one-year follow-up. Clin Implant Dent Relat Res. 2019; 21:462–472.
Article13. Eufinger H, Gellrich NC, Sandmann D, Dieckmann J. Descriptive and metric classification of jaw atrophy. An evaluation of 104 mandibles and 96 maxillae of dried skulls. Int J Oral Maxillofac Surg. 1997; 26:23–28.14. Cavalcanti MC, Guirado TE, Sapata VM, Costa C, Pannuti CM, Jung RE, et al. Maxillary sinus floor pneumatization and alveolar ridge resorption after tooth loss: a cross-sectional study. Braz Oral Res. 2018; 32:e64.
Article15. Misch CE, Judy KW. Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol. 1987; 4:7–13.16. Scheid RC, Woelfel JB. Woelfel's dental anatomy: its relevance to dentistry. 8th ed. Philadelphia (PA): Lippincott Williams & Wilkins;2007.17. Han SS, Lee KM, Kim KD. Availability of software-based correction of mandibular plane for the vertical measurement of the mandible in cone beam computed tomography. BioMed Res Int. 2015; 2015:808625.
Article18. Halperin-Sternfeld M, Machtei EE, Horwitz J. Diagnostic accuracy of cone beam computed tomography for dimensional linear measurements in the mandible. Int J Oral Maxillofac Implants. 2014; 29:593–599.
Article19. Perschbacher S. Interpretation of panoramic radiographs. Aust Dent J. 2012; 57 Suppl 1:40–45.
Article20. Gupta J, Ali SP. Cone beam computed tomography in oral implants. Natl J Maxillofac Surg. 2013; 4:2–6.
Article21. Benavides E, Rios HF, Ganz SD, An CH, Resnik R, Reardon GT, et al. Use of cone beam computed tomography in implant dentistry: the International Congress of Oral Implantologists consensus report. Implant Dent. 2012; 21:78–86.22. Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. Int J Oral Maxillofac Implants. 2014; 29 Suppl:55–77.
Article23. Walter C, Dagassan-Berndt DC, Kühl S, Weiger R, Lang NP, Zitzmann NU. Is furcation involvement in maxillary molars a predictor for subsequent bone augmentation prior to implant placement? A pilot study. Clin Oral Implants Res. 2014; 25:1352–1358.
Article24. Matsuda H, Borzabadi-Farahani A, Le BT. Three-dimensional alveolar bone anatomy of the maxillary first molars: a cone-beam computed tomography study with implications for immediate implant placement. Implant Dent. 2016; 25:367–372.25. Pagin O, Centurion BS, Rubira-Bullen IR, Alvares Capelozza AL. Maxillary sinus and posterior teeth: accessing close relationship by cone-beam computed tomographic scanning in a Brazilian population. J Endod. 2013; 39:748–751.
Article26. McNutt MD, Chou CH. Current trends in immediate osseous dental implant case selection criteria. J Dent Educ. 2003; 67:850–859.
Article27. Wagenberg BD, Ginsburg TR. Immediate implant placement on removal of the natural tooth: retrospective analysis of 1,081 implants. Compend Contin Educ Dent. 2001; 22:399–404.28. Misch CE. Maxillary sinus augmentation for endosteal implants: organized alternative treatment plans. Int J Oral Implantol. 1987; 4:49–58.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Morphometrics of alveolar process and anatomical structures around inferior maxillary sinus for maxillary implantation
- Survival rate of Astra Tech implants with maxillary sinus lift
- Assessment of the relationship between the maxillary molars and adjacent structures using cone beam computed tomography
- Anatomical factors of the maxillary tuberosity that influence molar distalization
- CLINICAL STUDY ON KOREAN POSTERIOR MAXILLAE RELATED TO DENTAL IMPLANT TREATMENT
