Basic Arterial Anatomy and Interpretation of CT Angiography for Intra-Abdominal or Gastrointestinal Bleeding: Correlation with Conventional Angiographic Findings for Beginners
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Medical Center, College of Medicine, Kyung Hee University, Seoul, Korea. kwon98@khu.ac.kr
- 2Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea University, Seoul, Korea.
- KMID: 2469186
- DOI: http://doi.org/10.3348/jksr.2020.81.1.119
Abstract
- It is essential to identify the causative artery in case of active intra-abdominal or gastrointestinal bleeding. A thorough understanding of the basic arterial anatomy is required to identify the causative artery on contrast-enhanced CT angiography and conventional catheter angiography. If one is familiar with the basic arterial anatomy, obtaining access to the bleeding artery will be easier, despite the variations in the origin and course of the vessels. We describe the basic arterial anatomy that will help beginners in diagnostic radiology to identify the blood vessels that can cause active intra-abdominal or gastrointestinal bleeding.
MeSH Terms
Figure
-
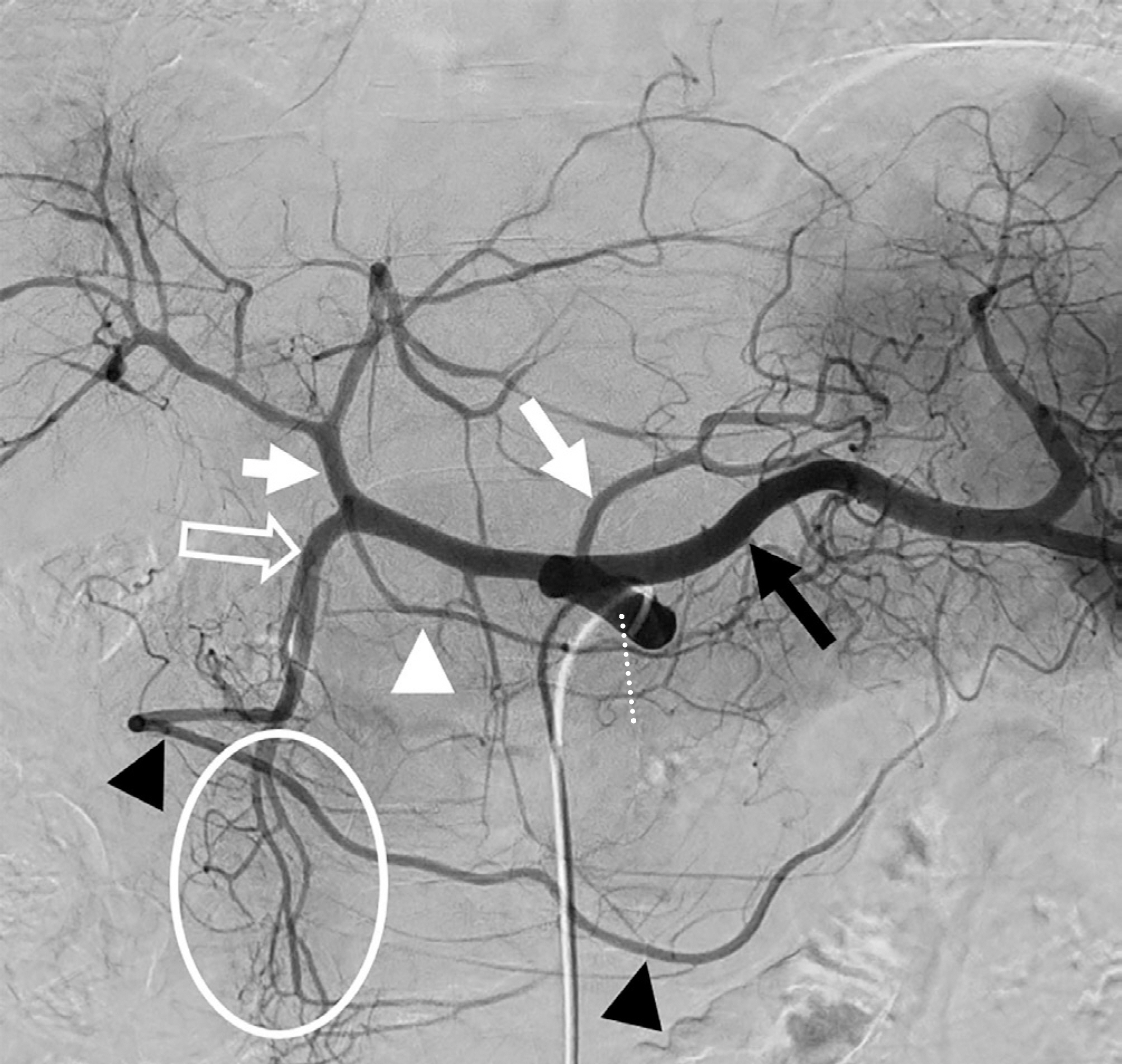
Fig. 1. Celiac trunk angiogram before transarterial chemoembolization of hepatocellular carcinoma in a 62- year-old man. The celiac trunk (dotted line) divides into three major branches—left gastric artery (white arrow), splenic artery (black arrow), and common hepatic artery. The common hepatic artery divides into the proper hepatic artery (short arrow) and gastroduodenal artery (empty arrow) after branching the right gastric artery (white arrowhead). From the gastroduodenal artery, right gas-troepiploic artery (black arrowheads) and superior pancreaticoduodenal artery (circle) arise. The superior pancreaticoduodenal artery divides into anterior and posterior divisions.

Fig. 2. Liver contusion from a motorcycle traffic accident in a 17-year-old boy. A, B. Active bleeding is well observed in liver segment 4A, characterized by increased contrast enhancement in the portal phase when compared to that in the delayed phase. C. The proper hepatic artery angiogram shows the right hepatic artery (arrowhead) and the left hepatic artery (empty arrowhead). The active bleeding (arrow) originates from the left hepatic artery branch.
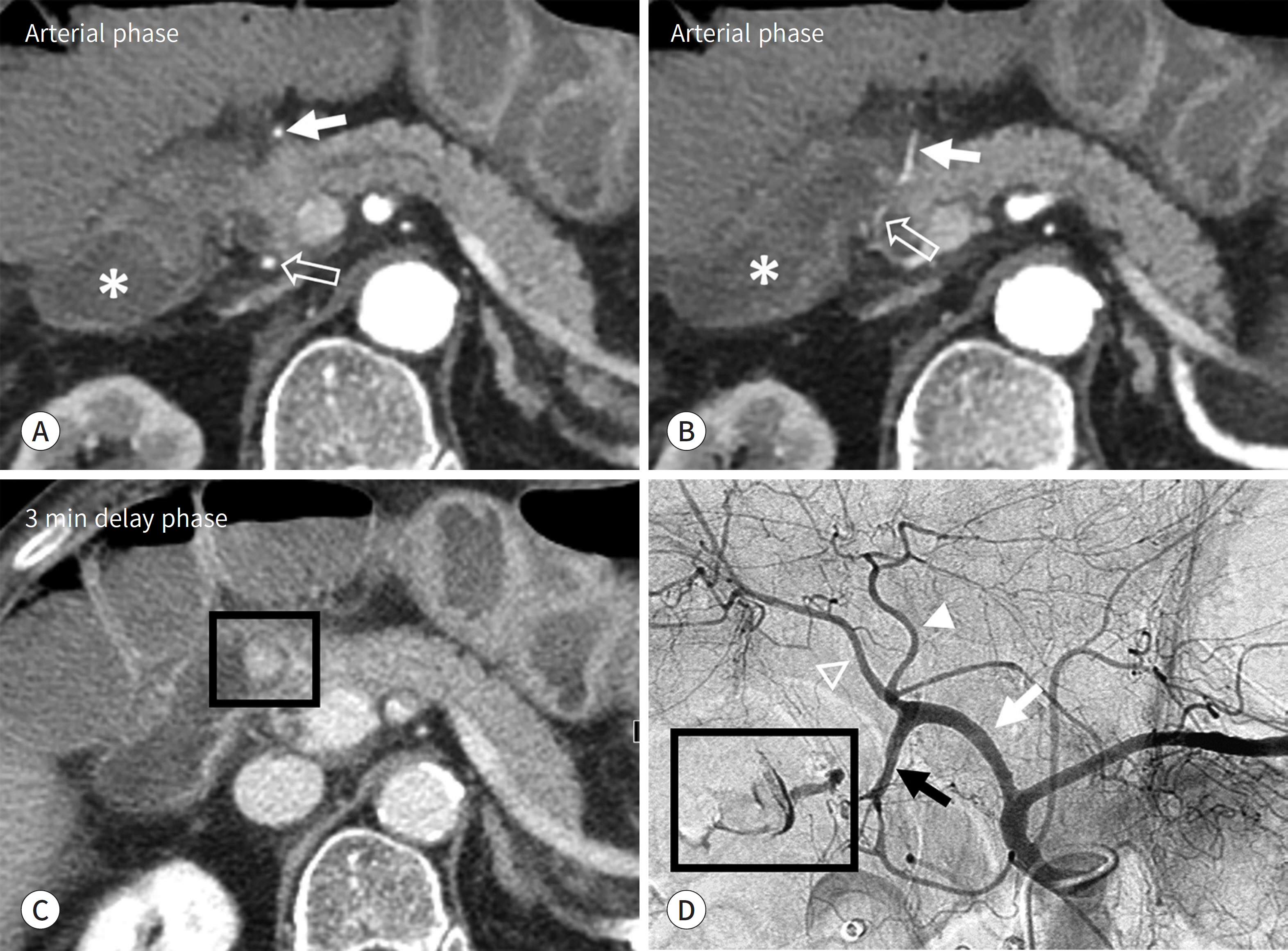
Fig. 3. Ulcer of duodenal 2nd portion on endoscopy in a 80-year-old woman. rows, A and B) and posterior (empty arrows, A and B) branches of the superior pancreaticoduodenal artery thought to be the causative artery, because it supplies the blood in this area. denal artery. Superior pancreaticoduodenal artery arises from the gastroduodenal artery (black arrow). In-row), LHA (arrowhead) and RHA (empty arrowhead), there was no evidence of active bleeding. A-C. Active bleeding (black box, C) is prominent in the proximal duodenum (asterisks) and the anterior (ar-are observed. A branch of the gastroduodenal artery, such as the superior pancreaticoduodenal artery, was D. Celiac trunk angiogram demonstrates the active bleeding (black box) from the superior pancreaticoduo-traluminal contour of the duodenum is visualized. In other major vessel branches such as CHA (white ar-CHA = common hepatic artery, LHA = left hepatic artery, RHA = right hepatic artery

Fig. 4. Massive hematochezia in a 56-year-old man. A-C. In the arterial phase, highly attenuated area (arrows) is observed in the jejunal loop. While the measured attenuation decreased in the delayed phase, the extent gradually increased in the portal and delayed phases. One explanation for such phenomenon is that the blood vessel supplying the jejunum is the causative artery. D. On the superior mesenteric angiogram, active extravasation (black box) in the jejunal branches (circle) is visualized. The ileal branches (dotted circle) are also visualized.
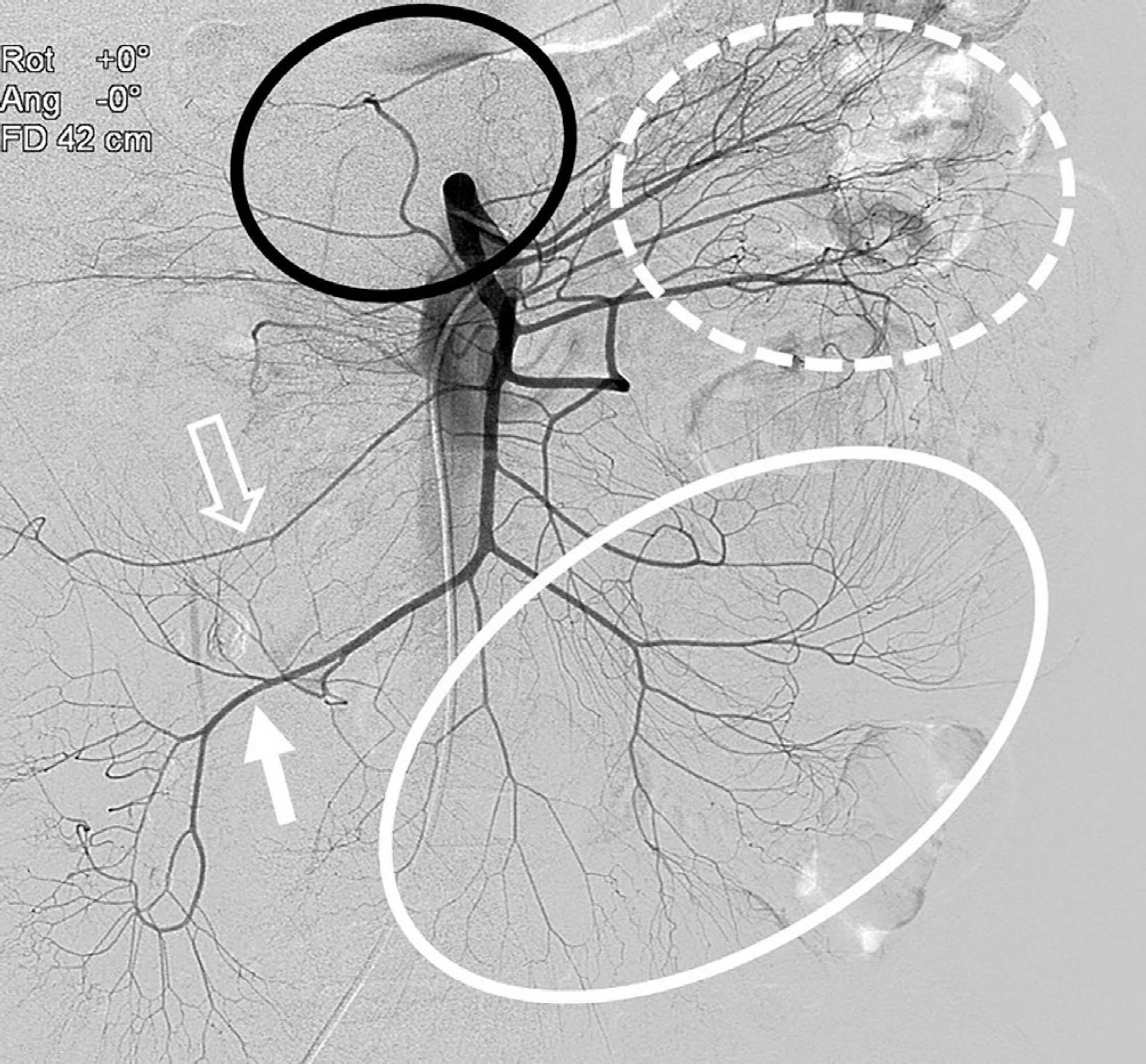
Fig. 5. Superior mesenteric angiogram for suspected active bleeding from a jejunal branch in a 56-year-old man. The superior mesenteric angiogram shows the jejunal branch (dotted circle), ileal branch (white circle), middle colic artery (black circle), right colic artery (empty arrow), and ileocolic artery (arrow). The inferior pancreaticoduodenal artery is barely visible on this angiographic image.
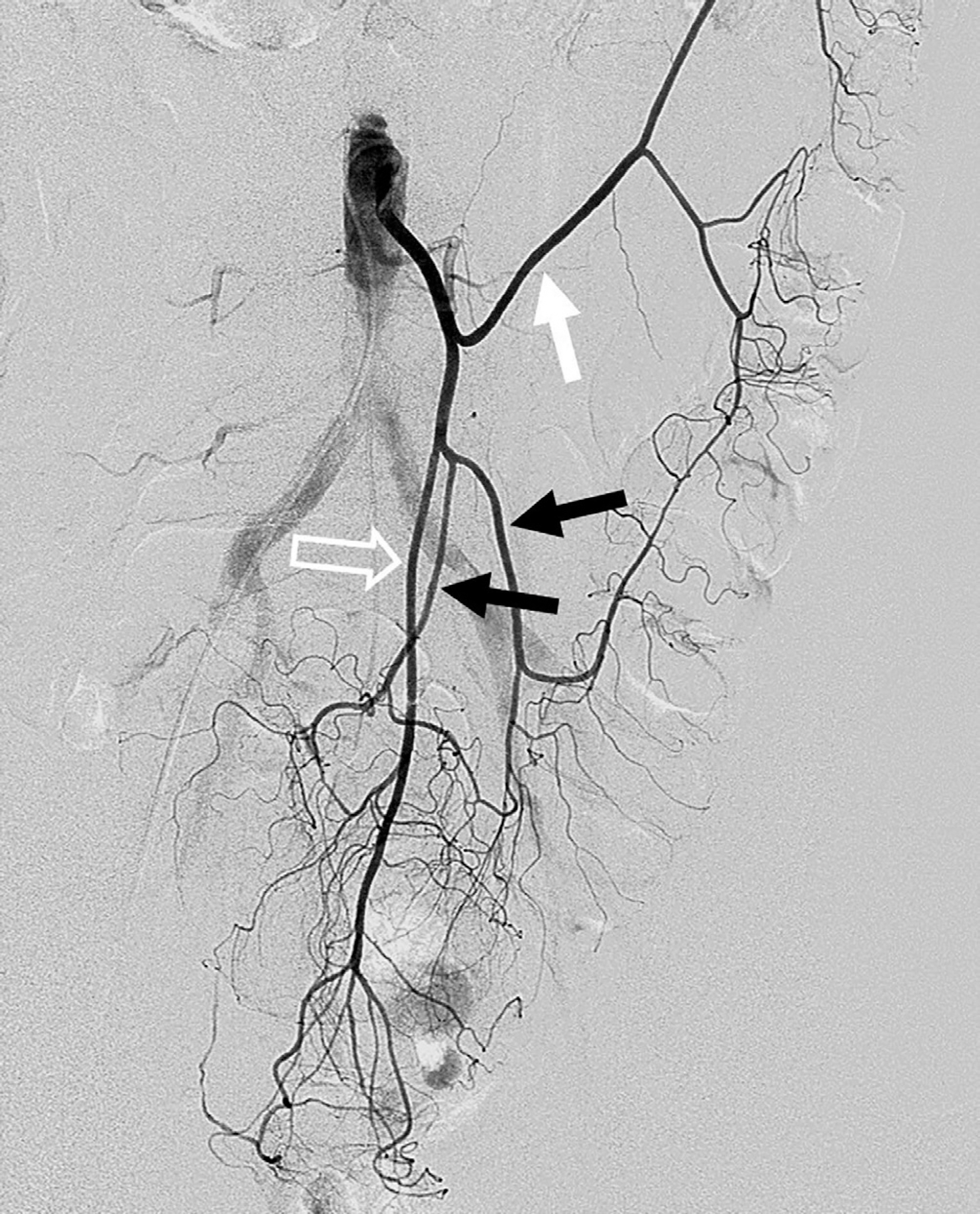
Fig. 6. Inferior mesenteric angiogram for suspected active bleeding from a jejunal branch in a 56-year-old man. The inferior mesenteric artery branches into the left colic (white arrow) and sigmoid arteries (black arrows). In the pelvic cavity, the inferior mesenteric artery continues its journey as the superior rectal artery (empty arrow).
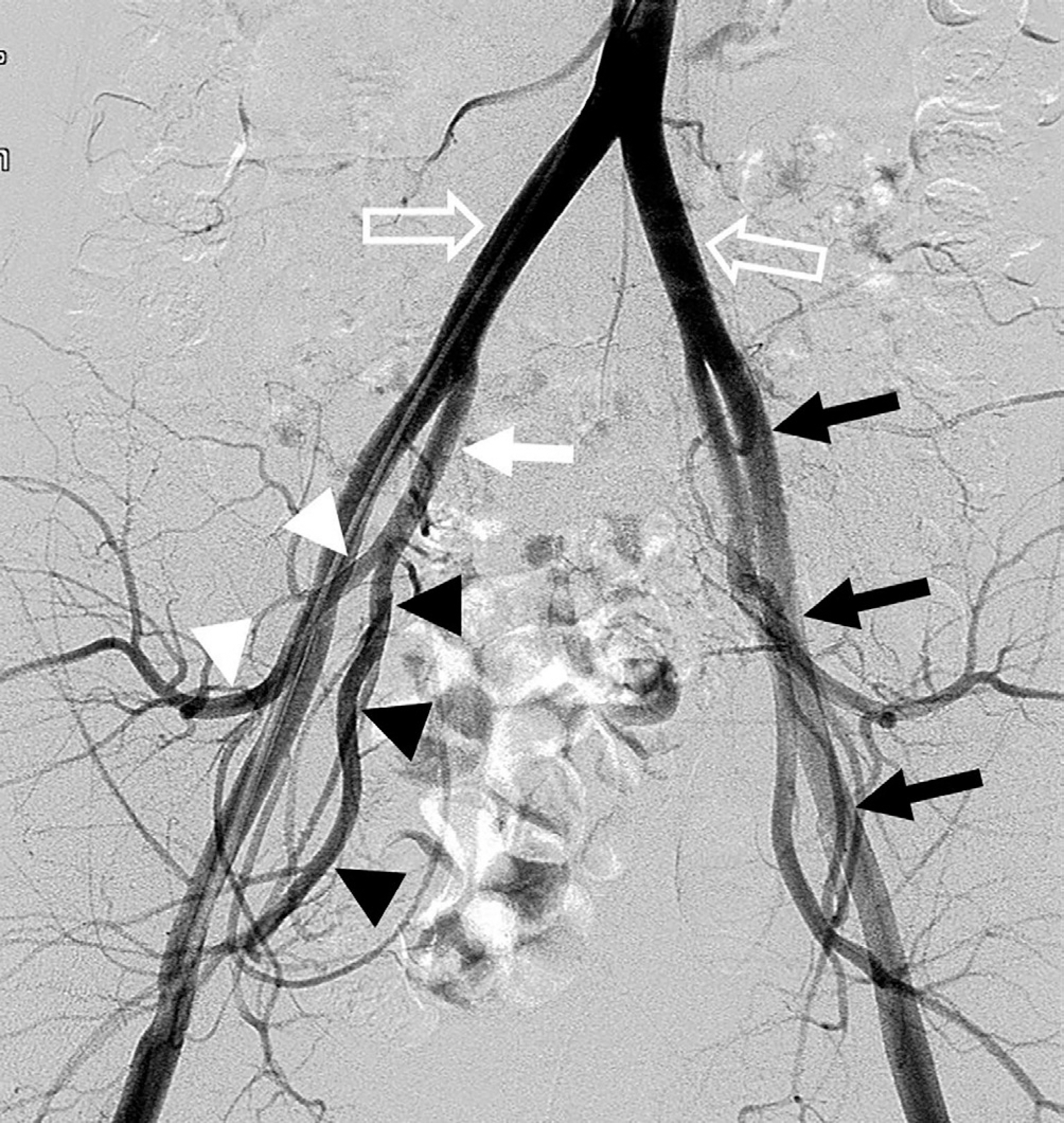
Fig. 7. The abdominal aorta divides into the common iliac arteries (empty arrows). The common iliac artery divides into the external iliac artery (black arrows) and the internal iliac artery (white arrow). The external iliac artery continues as the common femoral artery. The internal iliac artery divides into anterior (black arrowheads) and posterior (white arrowheads) divisions.
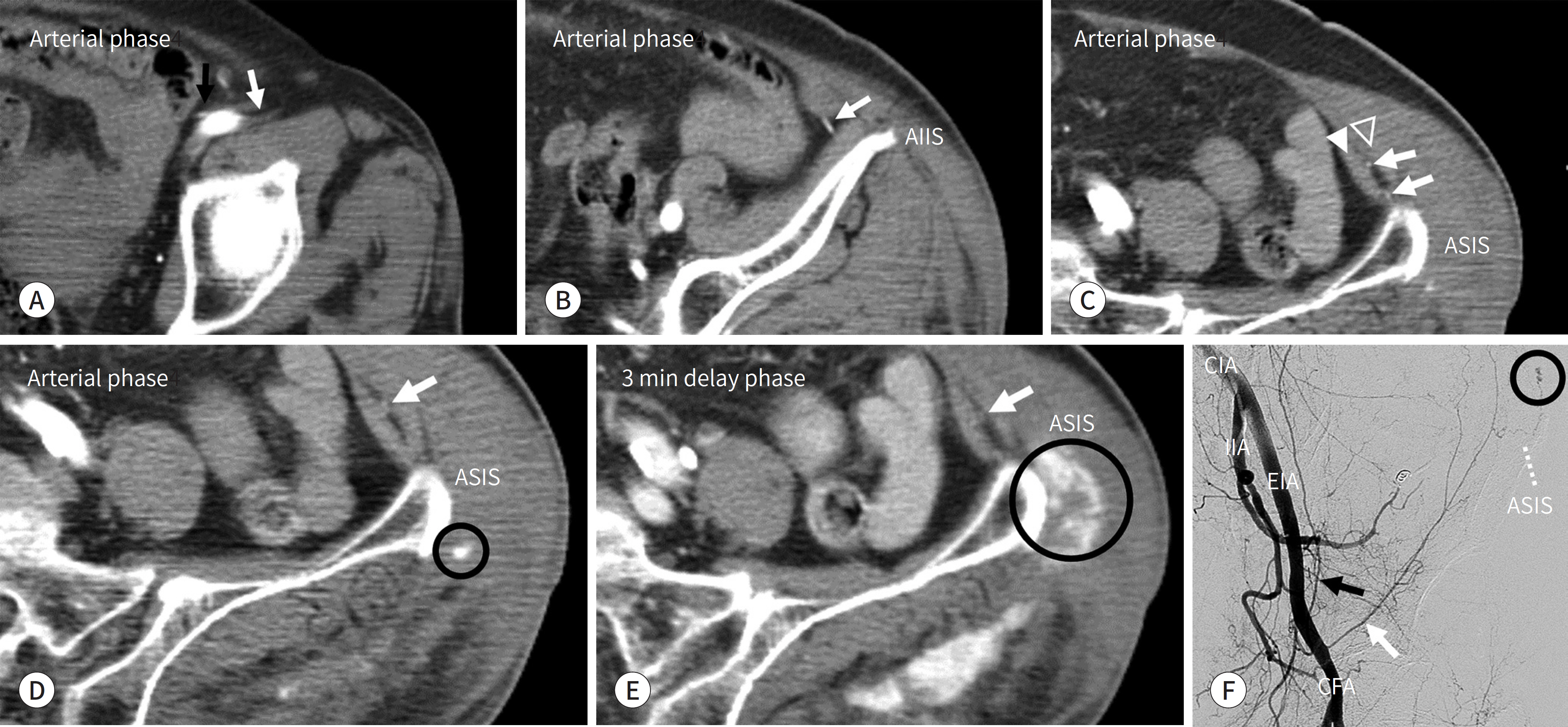
Fig. 8. An 83-year-old woman involved in an out car traffic accident.
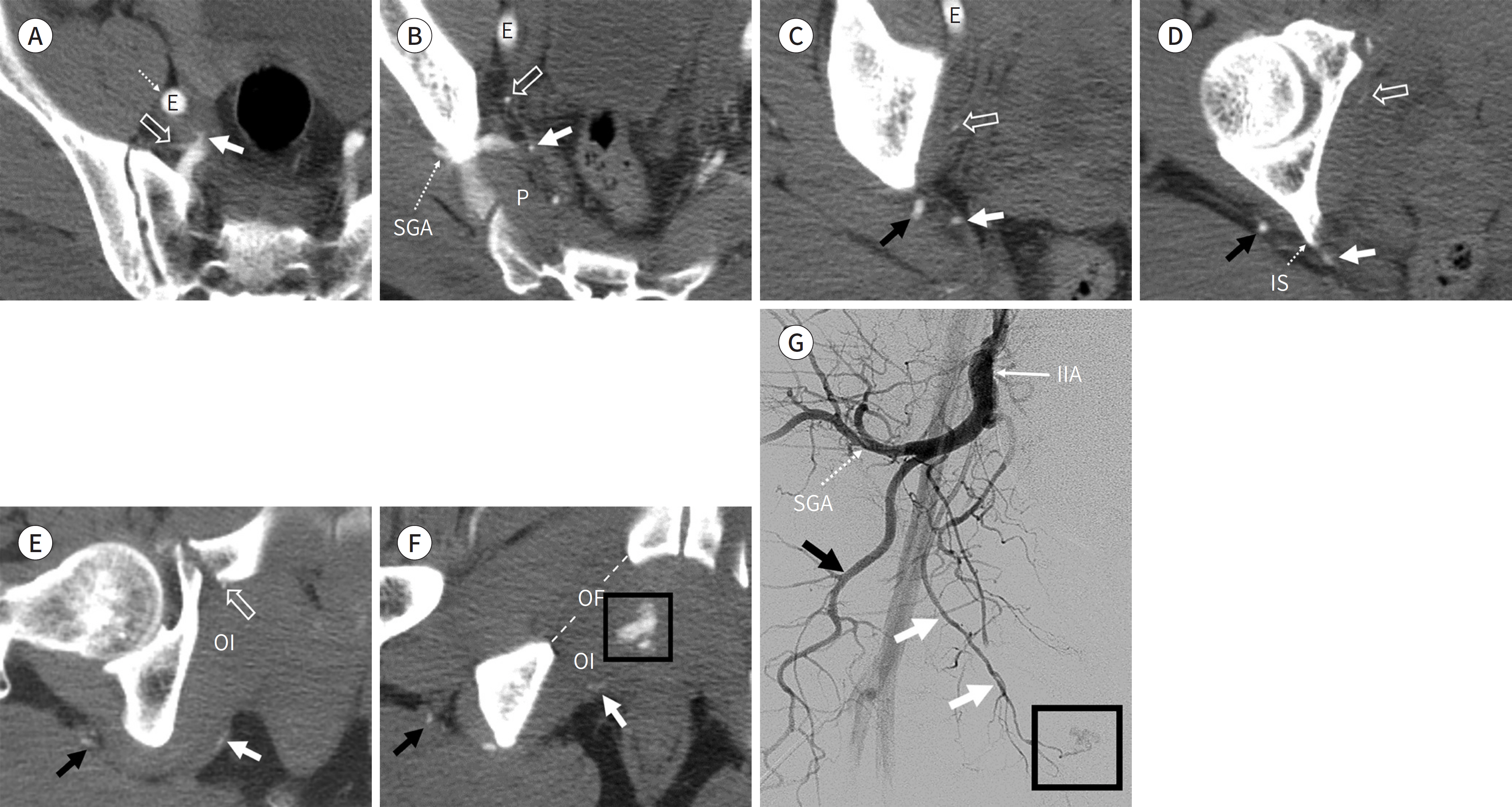
Fig. 9. Out car traffic accident with fracture of the right superior pubic ramus in a 52-year-old man. A-F. The internal pudendal artery (white arrows) exits the pelvis with the inferior gluteal artery (black arrows) through the lower part of the greater sciatic foramen. The lower part means the gap below the P and above the inferior margin of the greater sciatic foramen. The internal pudendal artery crosses behind the IS, then reenters the pelvis through the lesser sciatic foramen and runs medial to the OI muscle. The active bleeding (black box) is at the course of the right internal pudendal artery. The obturator artery (empty arrows) runs along the obturator fascia of the pelvic sidewall to reach the OF. The SGA passes the upper part of the greater sciatic foramen. G. Right internal iliac angiography shows active bleeding (black box) at the end of the internal pudendal artery (white arrows). The SGA (dotted arrow) and the inferior gluteal artery (black arrow) are visualized. This patient has an anatomical variation (commonly, the superior and inferior gluteal arteries arise from a common trunk). E = external iliac artery, IIA = internal iliac artery, IS = ischial spine, OF = obturator foramen, OI = obturator internus, P = piriformis muscle, SGA = superior gluteal artery
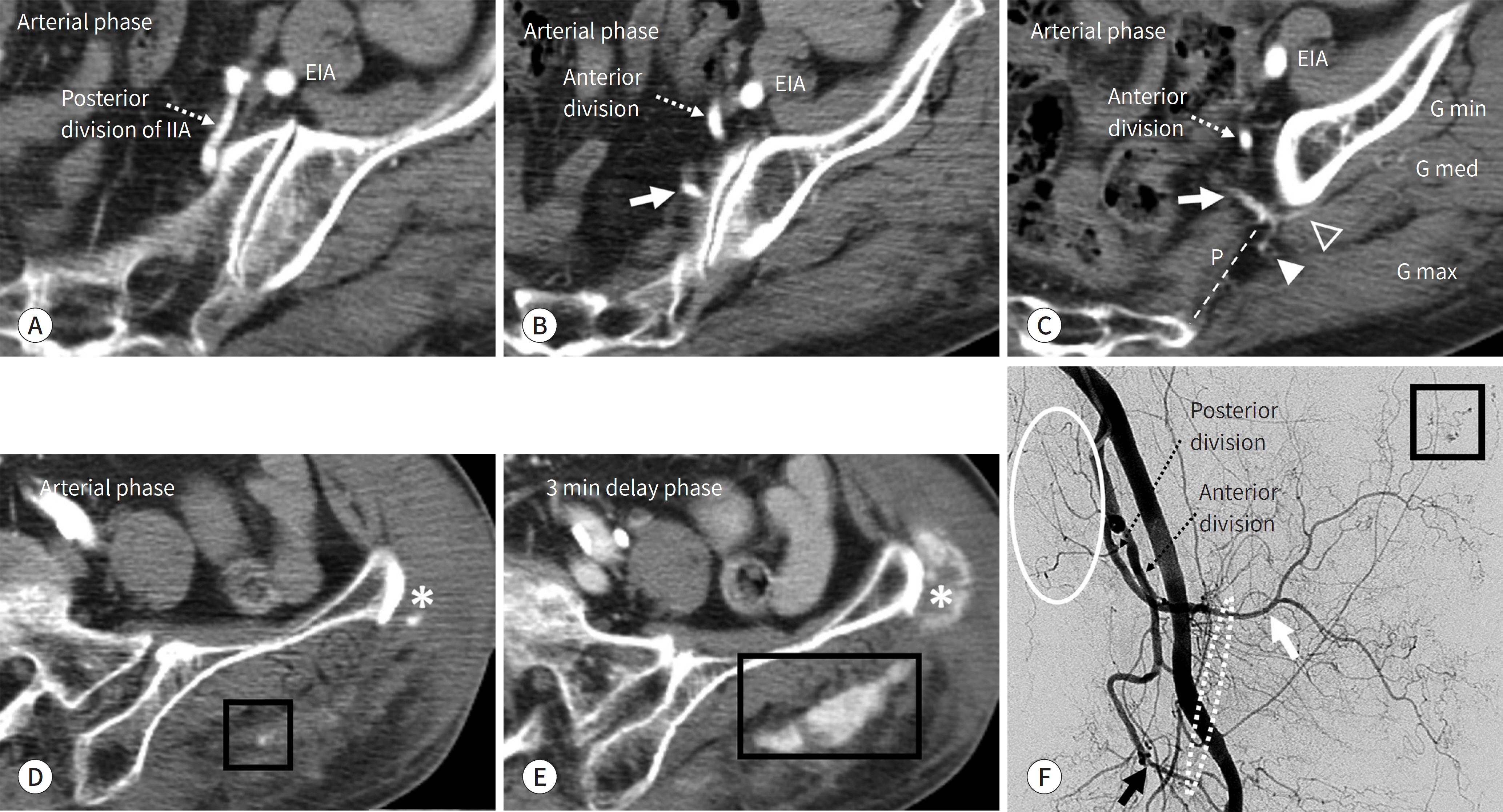
Fig. 10. Out car traffic accidenct in an 83-year-old woman. A-C. CT scan shows the superior gluteal artery (white arrows) arising from the posterior division of the IIA. The superior gluteal artery exits the pelvis through the greater sciatic foramen (dotted line), above the P. The superficial branch (arrowhead) runs between the G max and the G med muscles. The deep branch (empty arrowhead) runs between the G med and the G min muscles. D, E. A focal, highly attenuated area (black boxs) in the arterial phase increased in size in the delayed phase, mainly in the G max muscle. Injury to the superior gluteal artery was considered as the cause of the active bleeding in the left buttock area. Another active bleeding (asterisks) was mentioned in Fig. 8. F. An angiogram demonstrates active bleeding (black box) from the superior gluteal artery (white arrow). The superior gluteal artery passes the superior portion of the greater sciatic foramen, while the inferior gluteal artery (black arrow) passes the inferior portion of the same foramen. Therefore, the greater sciatic foramen would be located at the dotted circle area. The lateral sacral artery is also visualized (circle). EIA = external iliac artery, G max = gluteus maximus, G med = gluteus medius, G min = gluteus minimus, IIA = internal iliac artery, P = piriformis muscle
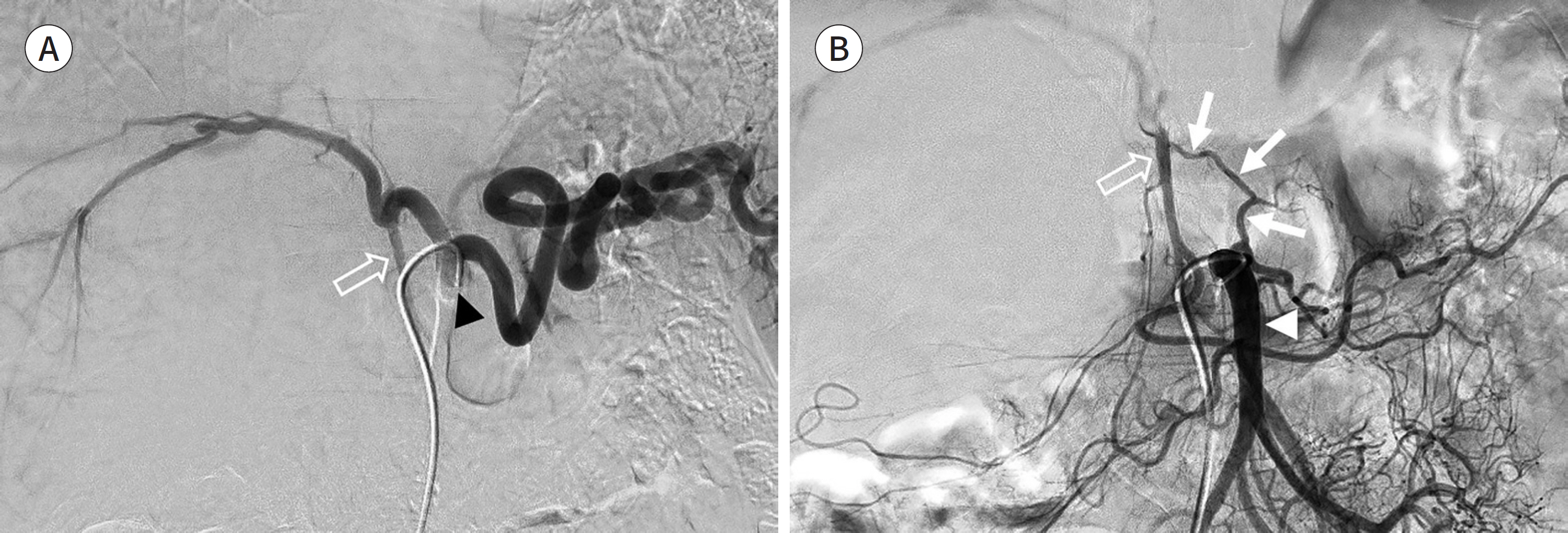
Fig. 11. Celiac trunk angiogram and superior mesenteric angiogram for transarterial chemoembolization in a 42-year-old man. A. Celiac trunk angiogram shows the gastroduodenal artery (empty arrow) arising from the celiac trunk (arrowhead). B. On the SMA angiogram, the gastroduodenal artery (empty arrow) is visualized in the arterial structure from SMA (arrowhead). This anastomosis between the SMA and the gastroduodenal artery (branch of the celiac trunk) forms an arc of Bühler (arrows).
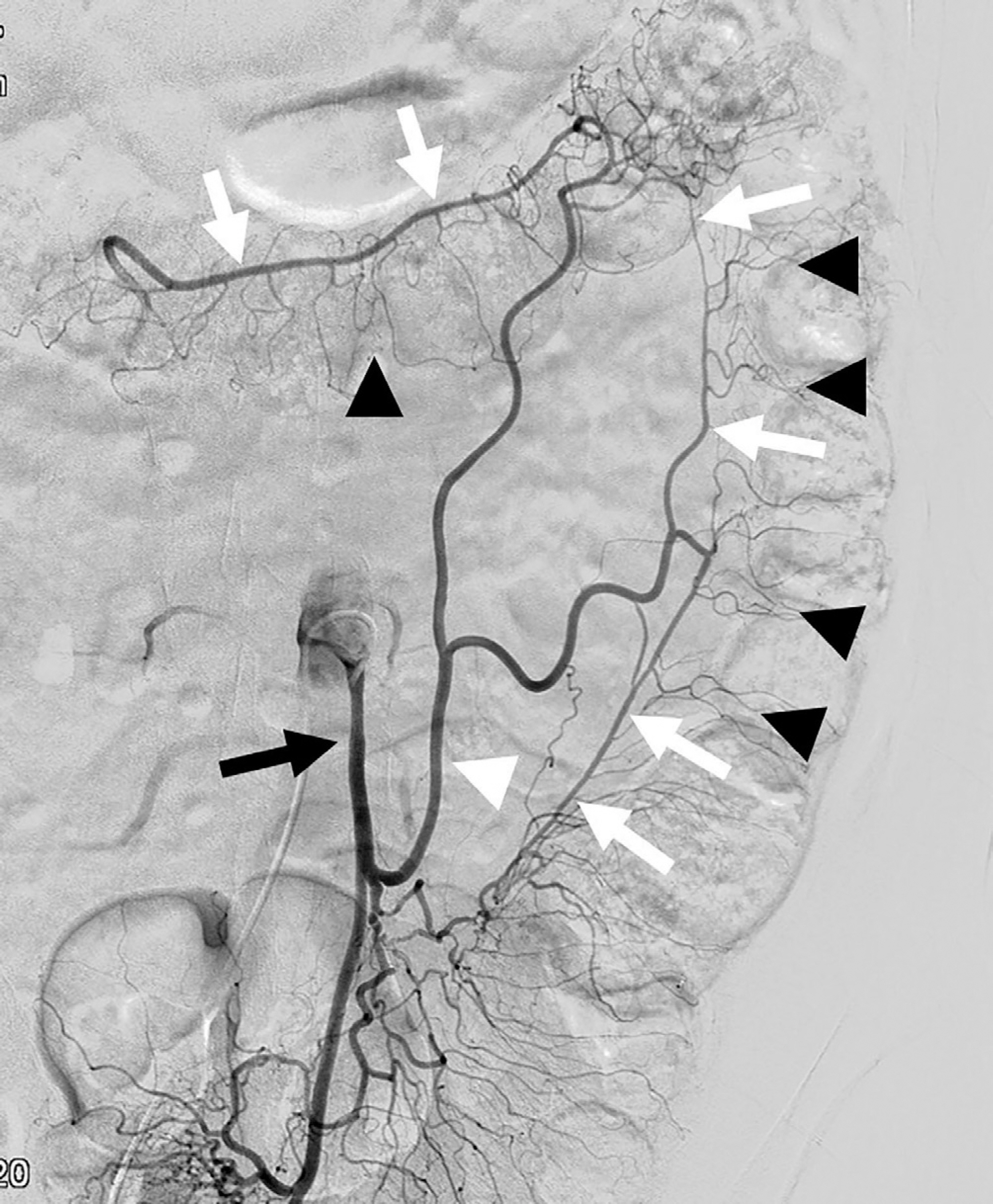
Fig. 12. On the angiogram of the inferior mesenteric artery (black arrow), the marginal artery of Drummond (white arrows) of the left colic artery (white arrowhead) is visualized. Vasa recta (black arrowheads) are visualized as fine straight arteries arising from this marginal artery.
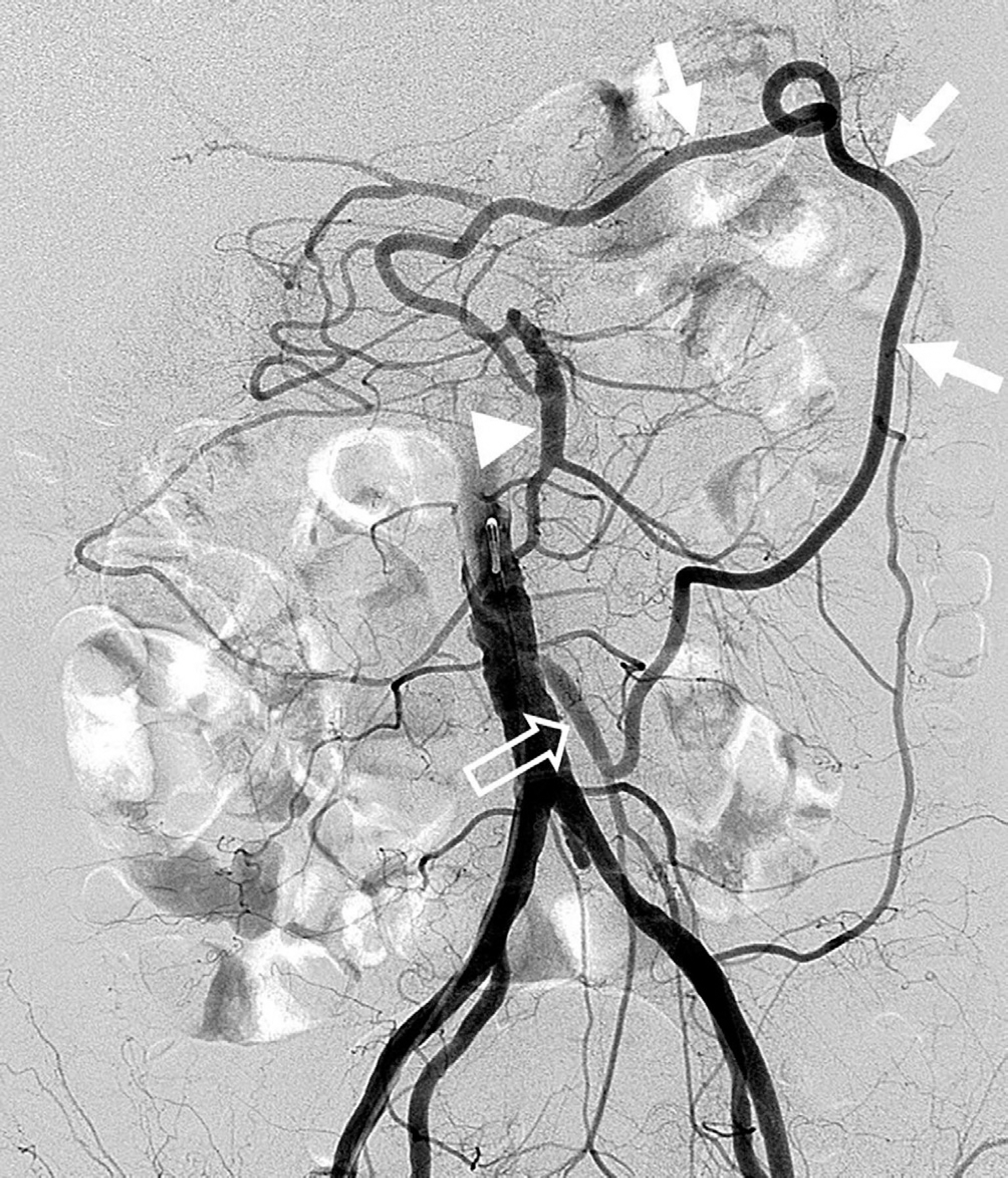
Fig. 13. On the aortogram, there is an arterial loop (white arrows) between the middle colic artery (arrowhead) of the SMA and the left colic artery of the IMA (empty arrow). This arc of Riolan (white arrows) runs close to the root of the mesentery as compared to the course of marginal artery of Drummond.
Reference
-
1. Artigas JM, Martí M, Soto JA, Esteban H, Pinilla I, Guillén E. Multidetector CT angiography for acute gastrointestinal bleeding: technique and findings. Radiographics. 2013; 33:1453–1470.
Article2. Dobritz M, Engels HP, Schneider A, Wieder H, Feussner H, Rummeny EJ, et al. Evaluation of dual-phase multidetector-row CT for detection of intestinal bleeding using an experimental bowel model. Eur Radiol. 2009; 19:875–881.
Article3. Kuhle WG, Sheiman RG. Detection of active colonic hemorrhage with use of helical CT: findings in a swine model. Radiology. 2003; 228:743–752.
Article4. Rimola J, Perendreu J, Falcó J, Fortuño JR, Massuet A, Branera J. Percutaneous arterial embolization in the management of rectus sheath hematoma. AJR Am J Roentgenol. 2007; 188:W497–W502.
Article5. Nakayama T, Ishibashi T, Eguchi D, Yamada K, Tsurumaru D, Sakamoto K, et al. Spontaneous internal oblique hematoma successfully treated by transcatheter arterial embolization. Radiat Med. 2008; 26:446–449.
Article6. Garg A, Gupta AK, Khandelwal N. Diagnostic radiology: chest and cardiovascular imaging. 4th ed. New Delhi: Jaypee Brothers Medical Pub 2018:2.7. White RD, Weir-McCall JR, Sullivan CM, Mustafa SA, Yeap PM, Budak MJ, et al. The celiac axis revisited: anatomic variants, pathologic features, and implications for modern endovascular management. Radiographics. 2015; 35:879–898.
Article8. Ahluwalia N, Futterman B. Anatomy, abdomen and pelvis, celiac trunk. Treasure Island: StatPearls Publish-ing LLC;2019.9. Korean Society of Interventional Radiology. Interventional radiology. 2nd ed. Seoul: Ilchokak;2014.10. Madoff DC, Denys A, Wallace MJ, Murthy R, Gupta S, Pillsbury EP, et al. Splenic arterial interventions: anatomy, indications, technical considerations, and potential complications. Radiographics. 2005; 25(Suppl 1):S191–S211.
Article11. Oderich GS. Mesenteric vascular disease current therapy. Berlin: Spinger;2015. p. 15.12. Horton KM, Fishman EK. Volume-rendered 3D CT of the mesenteric vasculature: normal anatomy, anatomic variants, and pathologic conditions. Radiographics. 2002; 22:161–172.
Article13. Joy P, Prithishkumar IJ, Isaac B. Clinical anatomy of the inferior epigastric artery with special relevance to invasive procedures of the anterior abdominal wall. J Minim Access Surg. 2017; 13:18–21.14. Selçuk I, Yassa M, Tatar I, Huri E. Anatomic structure of the internal iliac artery and its educative dissection for peripartum and pelvic hemorrhage. Turk J Obstet Gynecol. 2018; 15:126–129.
Article15. Yoon W, Kim JK, Jeong YY, Seo JJ, Park JG, Kang HK. Pelvic arterial hemorrhage in patients with pelvic frac-tures: detection with contrast-enhanced CT. Radiographics. 2004; 24:1591–1605. discussion 1605-1606.
Article16. Tansatit T, Chokrungyaranont P, Sanguansit P, Wanidchaphloi S. Anatomical study of the superior gluteal artery perforator (S-GAP) for free flap harvesting. J Med Assoc Thai. 2008; 91:1244–1249.17. Song SY, Chung JW, Kwon JW, Joh JH, Shin SJ, Kim HB, et al. Collateral pathways in patients with celiac axis stenosis: angiographic-spiral CT correlation. Radiographics. 2002; 22:881–893.
Article18. Kalva SP, Athanasoulis CA, Greenfield AJ, Fan CM, Curvelo M, Waltman AC, et al. Inferior pancreaticoduodenal artery aneurysms in association with celiac axis stenosis or occlusion. Eur J Vasc Endovasc Surg. 2007; 33:670–675.
Article19. Kwon SH, Ahn HJ, Oh JH. Is it the Arc of riolan or meandering mesenteric artery?J Endovasc Ther. 2015; 22:825–826.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multidetector-row CT Angiography of Hepatic Artery: Comparison with Conventional Angiography
- Identifying Small Bowel Gastrointestinal Stromal Tumor as the Culprit Lesion in Obscure Gastrointestinal Bleeding: Emphasis on Angiographic Findings
- Correlation of CT and angiographic findings in cerebrovascular occlusive disease
- Clinical Progression of Segmental Arterial Mediolysis; Renal Infarction and Intra-abdominal Hemorrhage
- Transcatheter Arterial Embolization of Arterial Esophageal Bleeding with the Use of N-Butyl Cyanoacrylate
