Diffusion-Weighted Magnetic Resonance Imaging of Spine
- Affiliations
-
- 1School of Medicine, Sungkyunkwan University, Seoul, Korea. youngcheol.yoon@gmail.com
- 2Department of Radiology, Samsung Medical Center, Seoul, Korea.
- KMID: 2469182
- DOI: http://doi.org/10.3348/jksr.2020.81.1.58
Abstract
- In this study, we evaluated the technical characteristics and usefulness of diffusion-weighted magnetic resonance imaging for discrimination between benign and malignant vertebral fractures, for detection and differentiation of multiple myeloma or metastases, and for response monitoring in malignant vertebral lesions after anticancer drug therapy or radiation therapy.
MeSH Terms
Figure
-
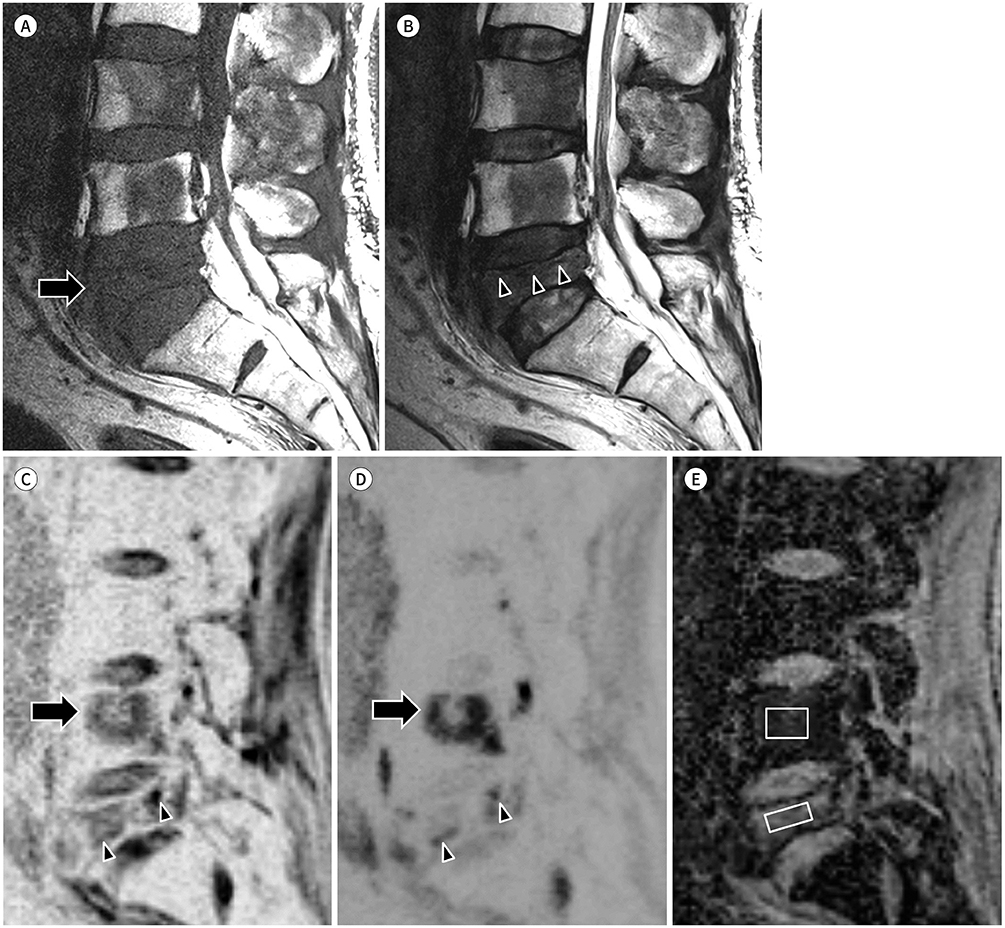
Fig. 1 Benign vertebral fracture in a 62-year-old man with hepatocellular carcinoma with coexisting bone metastasis in the adjacent vertebra. A. T1-weighted sagittal image showing decreased height of the L5 vertebral body (arrow) and low signal intensity lesions in the L3, L4, and L5 vertebral bodies. B. T2-weighted sagittal image showing a band-like low signal (arrowheads) parallel with the upper endplate of the L5 vertebral body. C, D. Diffusion-weighted images of b = 0 (C) and b = 800 (D) showing consistently increased signal in the L4 vertebral body (arrows) and seemingly decreased extent of the high signal area in the L5 vertebral body (arrowheads). E. ADC map showing a low ADC value (0.8 × 10−3 mm2/s) of the L4 lesion, indicating a viable metastasis, and a relatively high ADC value (1.5 × 10−3 mm2/s) of the L5 lesion, indicating a benign compression fracture. ADC = apparent diffusion coefficient

Fig. 2 Pathologic fracture in a 71-year-old man with non-small cell lung cancer. A, B. T1-weighted (A) and T2-weighted (B) images showing areas with heterogeneous low signal in the vertebral bodies and anterior wedging deformity (arrows) with posterior convexity of the T11 vertebral body (arrowheads). C, D. Diffusion-weighted images with b = 0 (C) and b = 800 (D) showing diffusion restriction in multiple thoracolumbar vertebral bodies and spinous processes. E. ADC map showing a low ADC value (0.9 × 10−3 mm2/s) of the T11 lesion, indicating a pathologic compression fracture. ADC = apparent diffusion coefficient

Fig. 3 Bone marrow edema adjacent to a Schmorl's node in a 24-year-old man with low back pain. A, B. T1-weighted image (A) showing poorly defined slightly low signal area in the bone marrow of the L4 vertebral body (arrowheads); T2-weighted image (B) showing poorly defined fluid-like high signal area (arrow) with adjacent intermediate-to-low signal area in the bone marrow of the L4 vertebral body (arrowheads). C, D. Diffusion-weighted images of b = 0 (C), showing increased signal area in the upper portion of the L4 vertebral body, and b = 800 (D), showing increased signal intensity (T2 shine-through effect) in the upper portion of the L4 vertebral body. E. ADC map showing a high ADC value (2.3 × 10−3 mm2/s) of the L4 lesion, indicating a benign process. ADC = apparent diffusion coefficient
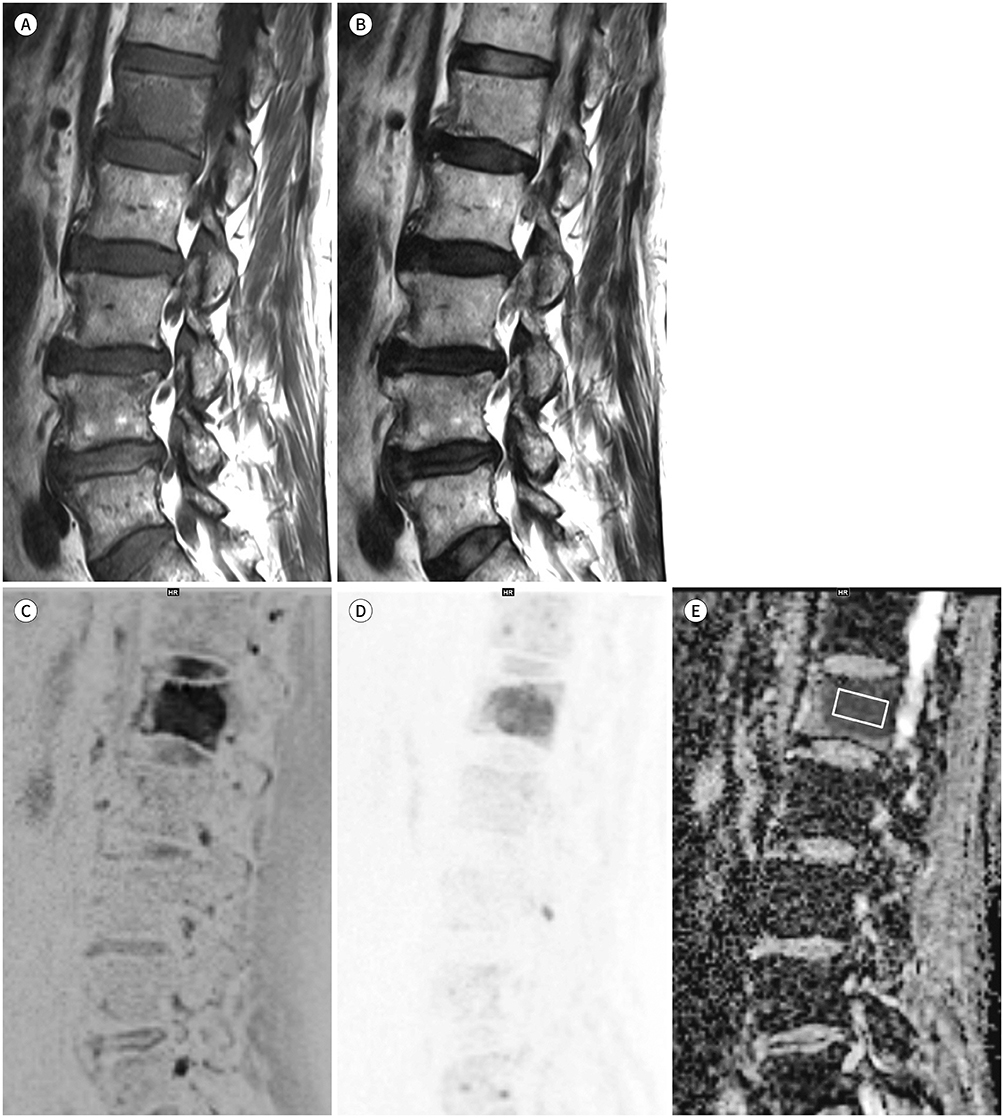
Fig. 4 Bone metastasis in the L1 vertebral body of a 56-year-old woman with advanced gastric cancer. A. T1-weighted image showing an ovoid area with low signal intensity in the L1 vertebral body. B. T2-weighted image showing iso- to slightly low signal intensity in the same area of the L1 vertebral body. C, D. Diffusion-weighted images with b = 0 (C) and b = 800 (D) showing high signal intensity in the area of the L1 vertebral body, indicating diffusion restriction. E. ADC map showing a low ADC value (0.8 × 10−3mm2/s) of the L1 lesion, indicating a viable bone metastasis. ADC = apparent diffusion coefficient
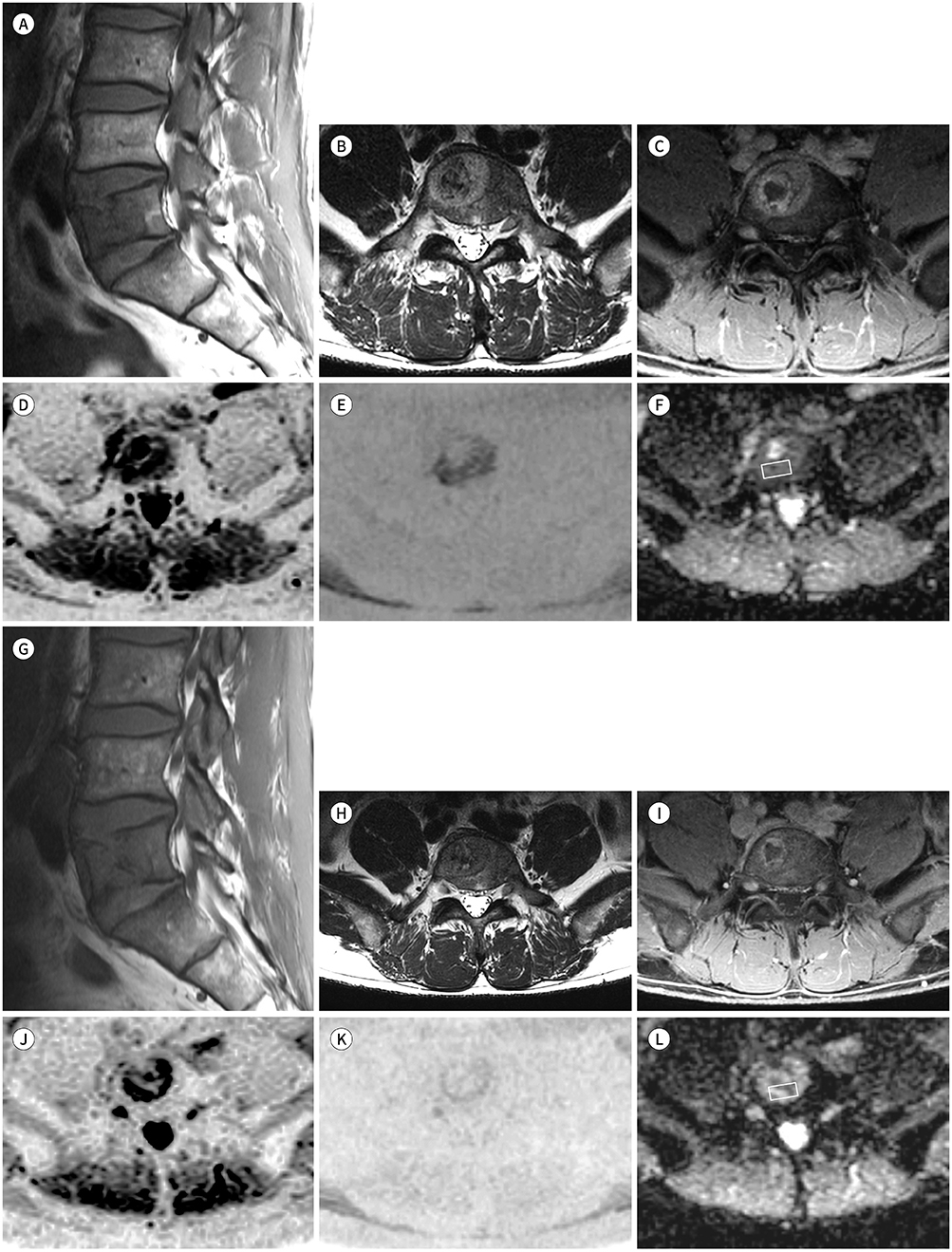
Fig. 5 MRI at baseline (A–F) and at 3 months follow-up (G–L) after radiation therapy for metastatic bone tumor in a 50-year-old woman with hepatocellular carcinoma. A–C. T1-weighted sagittal (A), T2-weighted axial (B), and post-contrast T1-weighted axial (C) images showing a metastatic bone lesion with enhancement and central necrosis in the L5 vertebral body. D, E. Diffusion-weighted images of b = 0 (D) and b = 1000 (E) showing diffusion restriction in the periphery of the bone lesion. F. ADC map showing a relatively low ADC value (0.7 × 10−3mm2/s) in the non-necrotic enhancing portion, indicating a viable tumor with high cellularity. G–I. T1-weighted sagittal (G), T2-weighted axial (H) and post-contrast T1-weighted axial (I) images showing decreased extent of the metastatic bone lesion with enhancement and central necrosis in the L5 vertebral body. J–L. Diffusion-weighted images of b = 0 (J) and b = 1000 (K) showing decreased extent of diffusion restriction in the periphery of the bone lesion; ADC map (L) showing an increased ADC value (1.2 × 10−3mm2/s) in the non-necrotic enhancing portion, indicating decreased viable tumor burden. ADC = apparent diffusion coefficient
Reference
-
1. Chokshi FH, Law M, Gibbs WN. Conventional and advanced imaging of spine oncologic disease, nonoperative post-treatment effects, and unique spinal conditions. Neurosurgery. 2018; 82:1–23.
Article2. Gibbs WN, Nael K, Doshi AH, Tanenbaum LN. Spine oncology: imaging and intervention. Radiol Clin North Am. 2019; 57:377–395.3. Tanenbaum LN. Clinical applications of diffusion imaging in the spine. Magn Reson Imaging Clin N Am. 2013; 21:299–320.
Article4. Dietrich O, Geith T, Reiser MF, Baur-Melnyk A. Diffusion imaging of the vertebral bone marrow. NMR Biomed. 2017; 30:e3333.
Article5. Moore WA, Khatri G, Madhuranthakam AJ, Sims RD, Pedrosa I. Added value of diffusion-weighted acquisitions in MRI of the abdomen and pelvis. AJR Am J Roentgenol. 2014; 202:995–1006.
Article6. Maier SE, Sun Y, Mulkern RV. Diffusion imaging of brain tumors. NMR Biomed. 2010; 23:849–864.
Article7. Park HJ, Lee SY, Rho MH, Chung EC, Kim MS, Kwon HJ, et al. Single-shot echo-planar diffusion-weighted MR imaging at 3T and 1.5T for differentiation of benign vertebral fracture edema and tumor infiltration. Korean J Radiol. 2016; 17:590–597.
Article8. Turner R, Le Bihan D, Maier J, Vavrek R, Hedges LK, Pekar J. Echo-planar imaging of intravoxel incoherent motion. Radiology. 1990; 177:407–414.
Article9. Stehling MK, Turner R, Mansfield P. Echo-planar imaging: magnetic resonance imaging in a fraction of a second. Science. 1991; 254:43–50.
Article10. Jeong EK, Kim SE, Guo J, Kholmovski EG, Parker DL. High-resolution DTI with 2D interleaved multislice reduced FOV single-shot diffusion-weighted EPI (2D ss-rFOV-DWEPI). Magn Reson Med. 2005; 54:1575–1579.
Article11. Saritas EU, Cunningham CH, Lee JH, Han ET, Nishimura DG. DWI of the spinal cord with reduced FOV single-shot EPI. Magn Reson Med. 2008; 60:468–473.
Article12. Riffel P, Michaely HJ, Morelli JN, Pfeuffer J, Attenberger UI, Schoenberg SO, et al. Zoomed EPI-DWI of the head and neck with two-dimensional, spatially-selective radiofrequency excitation pulses. Eur Radiol. 2014; 24:2507–2512.
Article13. Lee SK, Tan ET, Govenkar A, Hancu I. Dynamic slice-dependent shim and center frequency update in 3 T breast diffusion weighted imaging. Magn Reson Med. 2014; 71:1813–1818.
Article14. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, et al. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002; 47:1202–1210.
Article15. Castillo M, Arbelaez A, Smith JK, Fisher LL. Diffusion-weighted MR imaging offers no advantage over routine noncontrast MR imaging in the detection of vertebral metastases. AJNR Am J Neuroradiol. 2000; 21:948–953.16. Ortiz Gómez JA. The incidence of vertebral body metastases. Int Orthop. 1995; 19:309–311.
Article17. Schwaiger BJ, Gersing AS, Baum T, Krestan CR, Kirschke JS. Distinguishing benign and malignant vertebral fractures using CT and MRI. Semin Musculoskelet Radiol. 2016; 20:345–352.
Article18. Rizzoli R, Body JJ, Brandi ML, Cannata-Andia J, Chappard D, El Maghraoui A, et al. Cancer-associated bone disease. Osteoporos Int. 2013; 24:2929–2953.
Article19. Roodman GD. Mechanisms of bone metastasis. Discov Med. 2004; 4:144–148.
Article20. Smith JK, Lury K, Castillo M. Imaging of spinal and spinal cord tumors. Semin Roentgenol. 2006; 41:274–293.
Article21. Jung HS, Jee WH, McCauley TR, Ha KY, Choi KH. Discrimination of metastatic from acute osteoporotic compression spinal fractures with MR imaging. Radiographics. 2003; 23:179–187.22. Suh CH, Yun SJ, Jin W, Lee SH, Park SY, Ryu CW. ADC as a useful diagnostic tool for differentiating benign and malignant vertebral bone marrow lesions and compression fractures: a systematic review and metaanalysis. Eur Radiol. 2018; 28:2890–2902.
Article23. Biffar A, Baur-Melnyk A, Schmidt GP, Reiser MF, Dietrich O. Quantitative analysis of the diffusion-weighted steady-state free precession signal in vertebral bone marrow lesions. Invest Radiol. 2011; 46:601–609.
Article24. Baur A, Stäbler A, Brüning R, Bartl R, Krödel A, Reiser M, et al. Diffusion-weighted MR imaging of bone marrow: differentiation of benign versus pathologic compression fractures. Radiology. 1998; 207:349–356.
Article25. Koh DM, Collins DJ. Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol. 2007; 188:1622–1635.
Article26. Kwee TC, Takahara T, Ochiai R, Nievelstein RA, Luijten PR. Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology. Eur Radiol. 2008; 18:1937–1952.
Article27. Herneth AM, Philipp MO, Naude J, Funovics M, Beichel RR, Bammer R, et al. Vertebral metastases: assessment with apparent diffusion coefficient. Radiology. 2002; 225:889–894.
Article28. Castillo M. Diffusion-weighted imaging of the spine: is it reliable? AJNR Am J Neuroradiol. 2003; 24:1251–1253.29. Tang G, Liu Y, Li W, Yao J, Li B, Li P. Optimization of b value in diffusion-weighted MRI for the differential diagnosis of benign and malignant vertebral fractures. Skeletal Radiol. 2007; 36:1035–1041.
Article30. Kugel H, Jung C, Schulte O, Heindel W. Age- and sex-specific differences in the 1H-spectrum of vertebral bone marrow. J Magn Reson Imaging. 2001; 13:263–268.31. Kricun ME. Red-yellow marrow conversion: its effect on the location of some solitary bone lesions. Skeletal Radiol. 1985; 14:10–19.
Article32. Shellock FG, Morris E, Deutsch AL, Mink JH, Kerr R, Boden SD. Hematopoietic bone marrow hyperplasia: high prevalence on MR images of the knee in asymptomatic marathon runners. AJR Am J Roentgenol. 1992; 158:335–338.
Article33. Hoffbrand V, Provan D. ABC of clinical haematology. Macrocytic anaemias. BMJ. 1997; 314:430–433.
Article34. Kim HJ, Ryu KN, Choi WS, Choi BK, Choi JM, Yoon Y. Spinal involvement of hematopoietic malignancies and metastasis: differentiation using MR imaging. Clin Imaging. 1999; 23:125–133.35. Zhadanov SI, Doshi AH, Pawha PS, Corcuera-Solano I, Tanenbaum LN. Contrast-enhanced dixon fat-water separation imaging of the spine: added value of fat, in-phase and opposed-phase imaging in marrow lesion detection. J Comput Assist Tomogr. 2016; 40:985–990.36. Soliman M, Taunk NK, Simons RE, Osborne JR, Kim MM, Szerlip NJ, et al. Anatomic and functional imaging in the diagnosis of spine metastases and response assessment after spine radiosurgery. Neurosurg Focus. 2017; 42:E5.
Article37. Terpos E, Dimopoulos MA, Moulopoulos LA. The role of imaging in the treatment of patients with multiple myeloma in 2016. Am Soc Clin Oncol Educ Book. 2016; 35:e407–e417.
Article38. Dutoit JC, Verstraete KL. MRI in multiple myeloma: a pictorial review of diagnostic and post-treatment findings. Insights Imaging. 2016; 7:553–569.
Article39. Sachpekidis C, Mosebach J, Freitag MT, Wilhelm T, Mai EK, Goldschmidt H, et al. Application of 18F-FDG PET and diffusion weighted imaging (DWI) in multiple myeloma: comparison of functional imaging modalities. Am J Nucl Med Mol Imaging. 2015; 5:479–492.40. Balliu E, Vilanova JC, Peláez I, Puig J, Remollo S, Barceló C, et al. Diagnostic value of apparent diffusion coefficients to differentiate benign from malignant vertebral bone marrow lesions. Eur J Radiol. 2009; 69:560–566.
Article41. Switlyk MD. Magnetic resonance imaging for assessing treatment response in bone marrow metastases. Acta Radiol. 2019; 06. 01. DOI: 10.1177/0284185119851234. [Epub ahead of print].
Article42. Byun WM, Shin SO, Chang Y, Lee SJ, Finsterbusch J, Frahm J. Diffusion-weighted MR imaging of metastatic disease of the spine: assessment of response to therapy. AJNR Am J Neuroradiol. 2002; 23:906–912.43. Messiou C, Giles S, Collins DJ, West S, Davies FE, Morgan GJ, et al. Assessing response of myeloma bone disease with diffusion-weighted MRI. Br J Radiol. 2012; 85:e1198–e1203.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- RE: Diffusion-Weighted Imaging of Prostate Cancer: How Can We Use It Accurately?
- The Usefulness of Diffusion-weighted MR Imaging for Differentiation between Degenerative Spines and Infectious Spondylitis
- Diffusion-Weighted Magnetic Resonance Imaging Findings in a Patient with Trigeminal Ganglioneuroma
- Advanced Magnetic Resonance Imaging for Pediatric Brain Tumors: Current Imaging Techniques and Interpretation Algorithms
- The Value of PROPELLER Diffusion-Weighted Image in the Detection of Cholesteatoma
