Scaling Echocardiographic Cardiac Dimensions to Body Size: A Bayesian Analysis in Healthy Men and Women
- Affiliations
-
- 1Department of Cardiology, Complejo Asistencial Universitario de Leon, Leon, Spain. jiiglesias@saludcastillayleon.es
- 2Department of Occupational Medicine, Complejo Asistencial Universitario de Leon, Leon, Spain.
- KMID: 2468375
- DOI: http://doi.org/10.4250/jcvi.2019.0056
Abstract
- BACKGROUND
Proper scaling of cardiac dimensions is of paramount importance in making correct decisions in clinical cardiology. The usual normalization of cardiac dimensions to overall body size assumes an isometric relationship. We sought to investigate these relationships to obtain the best allometric coefficient (AC) for scaling.
METHODS
Ninety-seven healthy volunteers were included. The dimensions to be scaled were the left atrial volume, the end-diastolic and end-systolic left ventricular volumes, and the diameter of the tricuspid annulus. A Bayesian statistical analysis was applied with isometric coefficients as priors.
RESULTS
The linear correlations between cardiac dimensions and body size were modest, ranging from 0.12 (-0.10-0.32) for the left atrial volume and height to 0.70 (0.58-0.80) for the end-diastolic volume and height. The ACs varied across the different cardiac dimensions and body size measurements. For the best linear relationships, the isometric coefficients were outside the 95% highest density interval of the posterior distribution for the left atrial volume-weight (AC: 0.7; 0.4-0.9) and end-diastolic volume-height (AC: 2.3; 1.7-2.9), whereas they were different from 1 for the left atrial volume-weight, end-diastolic volume, and diameter of the tricuspid annulus-body surface area (AC: 0.6; 0.3-0.8). Not scaling the cardiac dimensions to their corresponding ACs can lead to important errors in size estimations of cardiac structure.
CONCLUSIONS
The ACs found in this study are somewhat different from the corresponding isometric coefficients and often different from 1. This finding should be considered when normalizing cardiac structures to body size when making clinical decisions.
Keyword
Figure
-
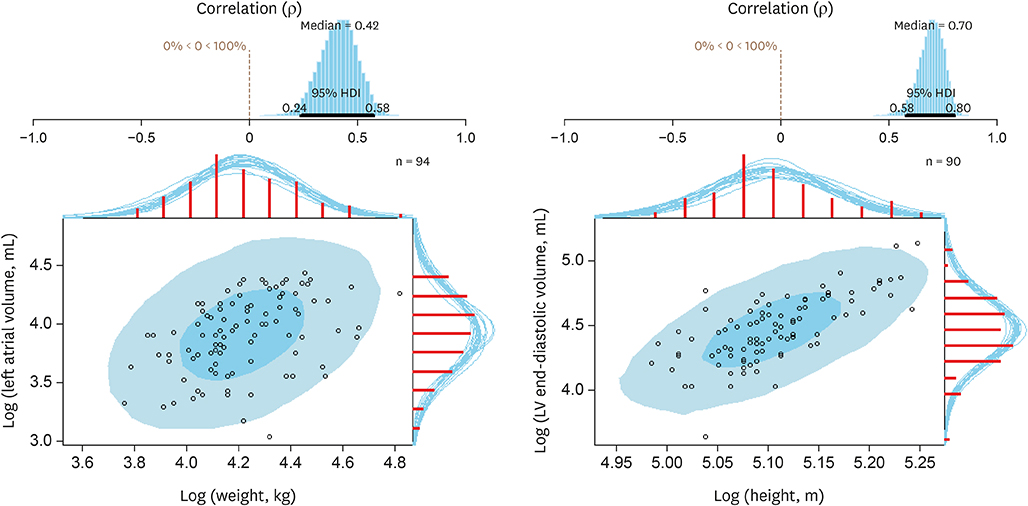
Figure 1 Bayesian correlation between cardiac structures and body size (left atrial volume and weight; LV end-diastolic volume and height). For details, see Table 1. LV: left ventricle.

Figure 2 Bayesian correlation between cardiac structures and body size (LV end-systolic volume and body surface area; tricuspid annulus diameter and body surface area). For details, see Table 1. LV: left ventricle.
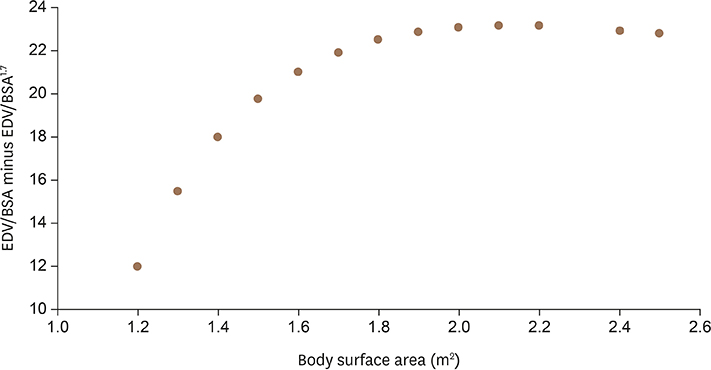
Figure 3 Difference between indexed left ventricular EDV to the BSA to power of 1 and 1.5 across different BSAs for a theoretical absolute value of 120 mL. BSA: body surface area, EDV: end-diastolic volume.
Cited by 1 articles
-
Normalization of Cardiac Measurements: Isometric vs. Allometric Method
Sung Hye Kim
J Cardiovasc Imaging. 2020;28(1):18-20. doi: 10.4250/jcvi.2019.0114.
Reference
-
1. Gayon J. History of the concept of allometry. Am Zool. 2000; 40:748–758.
Article2. de Simone G, Daniels SR, Devereux RB, et al. Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweight. J Am Coll Cardiol. 1992; 20:1251–1260.
Article3. McMahon T. Size and shape in biology. Science. 1973; 179:1201–1204.4. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016; 37:2129–2200.5. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg. 2012; 42:S1–S44.6. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:e57–185.7. Bolstad WM, Curran JM. Introduction to Bayesian Statistics. 3rd edition. New Jersey: John Wiley & Sons;2016. p. 235.8. Wakefield JC, Smith AF, Racine‐Poon A, Gelfand AE. Bayesian analysis of linear and non‐linear population models by using the Gibbs sampler. J R Stat Soc Ser C Appl Stat. 1994; 43:201–221.
Article9. Dewey FE, Rosenthal D, Murphy DJ Jr, Froelicher VF, Ashley EA. Does size matter? Clinical applications of scaling cardiac size and function for body size. Circulation. 2008; 117:2279–2287.10. Pelliccia A, Culasso F, Di Paolo FM, Maron BJ. Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med. 1999; 130:23–31.
Article11. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1–39.e14.
Article12. Gutgesell HP, Rembold CM. Growth of the human heart relative to body surface area. Am J Cardiol. 1990; 65:662–668.
Article13. Chirinos JA, Segers P, De Buyzere ML, et al. Left ventricular mass: allometric scaling, normative values, effect of obesity, and prognostic performance. Hypertension. 2010; 56:91–98.14. de Simone G, Kizer JR, Chinali M, et al. Normalization for body size and population-attributable risk of left ventricular hypertrophy: the Strong Heart Study. Am J Hypertens. 2005; 18:191–196.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spinal Dimensions and Shape Variation in Koreans: Radiographic Quantitative Morphometry
- Echocardiographic parameters and indices in 23 healthy Maltese dogs
- Serial investigation on the interrelationship between body height, weight and selected craniofacial dimensions during mixed dentition period
- Multicenter Trial for Estimation of Normal Values of Echocardiographic Indices in Korea
- Coronary Artery Size in Korean: Normal Value and its Determinants
