3D Printer Application for Endoscope-Assisted Spine Surgery Instrument Development: From Prototype Instruments to Patient-Specific 3D Models
- Affiliations
-
- 1Department of Neurosurgery, Seoul Barunsesang Hospital, Seoul, Korea.
- 2Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. spinepjy@gmail.com
- KMID: 2466341
- DOI: http://doi.org/10.3349/ymj.2020.61.1.94
Abstract
- Developing new surgical instruments is challenging. While making surgical instruments could be a good field of application for 3D printers, attempts to do so have proven limited. We designed a new endoscope-assisted spine surgery system, and using a 3D printer, attempted to create a complex surgical instrument and to evaluate the feasibility thereof. Developing the new surgical instruments using a 3D printer consisted of two parts: one part was the creation of a prototype instrument, and the other was the production of a patient model. We designed a new endoscope-assisted spine surgery system with a cannula for the endoscope and working instruments and extra cannula that could be easily added. Using custom-made patient-specific 3D models, we conducted discectomies for paramedian and foraminal discs with both the newly designed spine surgery system and conventional tubular surgery. The new spine surgery system had an extra portal that can be well bonded in by a magnetic connector and greatly expanded the range of access for instruments without unnecessary bone destruction. In foraminal discectomy, the newly designed spine surgery system showed less facet resection, compared to conventional surgery. We were able to develop and demonstrate the usefulness of a new endoscope-assisted spine surgery system relying on 3D printing technology. Using the extra portal, the usability of endoscope-assisted surgery could be greatly increased. We suggest that 3D printing technology can be very useful for the realization and evaluation of complex surgical instrument systems.
Keyword
MeSH Terms
Figure
-
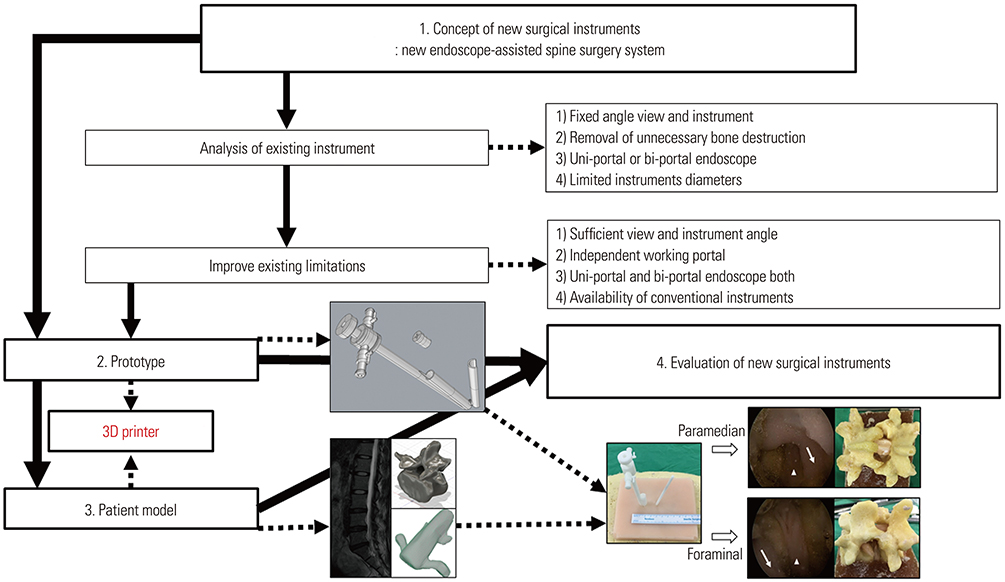
Fig. 1 Workflow diagram of the development and evaluation of new surgical instruments. The solid arrow indicates the conventional application, and the dotted arrow indicates the application of endoscope-assisted spine surgery.

Fig. 2 New endoscope-assisted spine surgery system. (A) Two tubes were joined together: one for an endoscope and the other for an instrument working cannula. The instrument working cannula could be blocked with a rubber cap to maintain proper saline pressure. (B) 3D-printed prototypes of the new endoscope-assisted spine surgery system. A 10-mm incision was needed for patient model application. (C) Photograph of a surgical test using the new endoscope-assisted spine surgery system. An endoscopic drill was inserted at the working cannula. (D) Operation field with the new system. Similar operational views with conventional endoscopic spine surgery. The arrow head is the ligamentum flavum at the inter-laminar space, and the arrows indicate the lamina of the superior and inferior vertebral body.
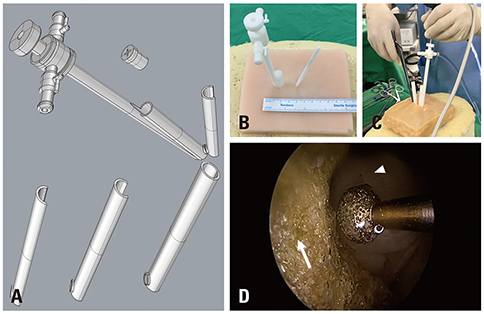
Fig. 3 New endoscope-assisted spine surgery system with an additional working portal. (A) After blocking of the instrument working cannula, only the endoscope cannula was used. Various shapes (semicircular or circular) of an additional working portal could be used. (B) 3D-printed prototype of the new endoscope-assisted spine surgery system with an additional working portal. A 10-mm incision and 5-mm additional incision were needed for patient model application. (C) Photograph of a surgical test using the new endoscope-assisted spine surgery system with a semicircular additional working portal. Conventional punch and instruments could be used. (D) A conventional drill was inserted at the working cannula. The operation field was well-visualized with the new system with the additional working portal. Instrument movement was freer, compared to conventional endoscopic spine surgery, such as bi-portal endoscopic spine surgery. The arrow head indicates the ligamentum flavum at the inter-laminar space, and the arrow shows the lamina of the superior vertebral body.
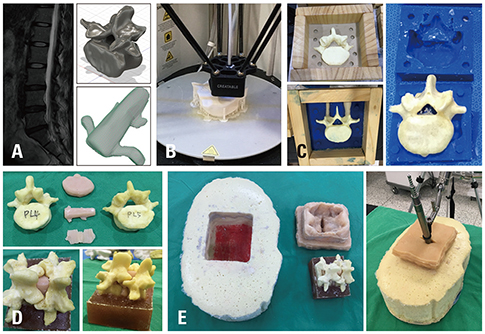
Fig. 4 Patient-based model created with the 3D printing technique. (A) 3D modeling of spine components using patient MRI data. (B) Printing spine components using a 3D printer. (C) Making silicone molds for patient-based 3D-printed spine components. (D) Making spinal components considering physical properties (vertebra, discs, nerves, ligaments) using patient-based spine component molds. (E) Making a patient model after assembling the body frame, spine components, and skin with soft tissue.

Fig. 5 Discectomy with a tubular retractor. A paramedian approach is shown above, and a foraminal approach is shown below. The arrows indicate the nerve root, and arrow heads show the discs.
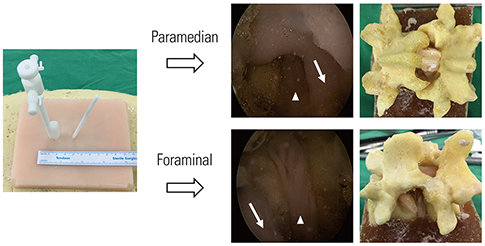
Fig. 6 Discectomy with the new endoscope-assisted spine surgery system. A paramedian approach is shown above, and a foraminal approach is shown below. The arrows indicate the nerve root, and arrow heads show the discs. Less bone destruction was observed with the new system, compared to the conventional tubular retractor in the foraminal approach.
Reference
-
1. Mavili ME, Canter HI, Saglam-Aydinatay B, Kamaci S, Kocadereli I. Use of three-dimensional medical modeling methods for precise planning of orthognathic surgery. J Craniofac Surg. 2007; 18:740–747.
Article2. Lee S, Kim JY, Hong J, Baek SH, Kim SY. CT-based navigation system using a patient-specific instrument for femoral component positioning: an experimental in vitro study with a sawbone model. Yonsei Med J. 2018; 59:769–780.
Article3. Christoudias GC. The making of an instrument: from concept to market. JSLS. 1998; 2:301–307.4. Kim JE, Choi DJ. Clinical and radiological outcomes of unilateral biportal endoscopic decompression by 30° arthroscopy in lumbar spinal stenosis: minimum 2-year follow-up. Clin Orthop Surg. 2018; 10:328–336.
Article5. Wang YP, Zhang W, Li BL, Sun YP, Ding WY, Shen Y. Suprapedicular foraminal endoscopic approach to lumbar lateral recess decompression surgery to treat degenerative lumbar spinal stenosis. Med Sci Monit. 2016; 22:4604–4611.
Article6. Heo DH, Quillo-Olvera J, Park CK. Can percutaneous biportal endoscopic surgery achieve enough canal decompression for degenerative lumbar stenosis? Prospective case-control study. World Neurosurg. 2018; 120:e684–e689.
Article7. Sayed Aluwee SAZB, Zhou X, Kato H, Makino H, Muramatsu C, Hara T, et al. Evaluation of pre-surgical models for uterine surgery by use of three-dimensional printing and mold casting. Radiol Phys Technol. 2017; 10:279–285.
Article8. Siu TL, Lin K. Microscopic tubular discectomy for far lateral lumbar disc herniation. J Clin Neurosci. 2016; 33:129–133.
Article9. Clark AJ, Safaee MM, Khan NR, Brown MT, Foley KT. Tubular microdiscectomy: techniques, complication avoidance, and review of the literature. Neurosurg Focus. 2017; 43:E7.
Article10. Ruetten S, Komp M, Merk H, Godolias G. Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: a prospective, randomized, controlled study. J Neurosurg Spine. 2009; 10:476–485.
Article11. Maroon JC. Current concepts in minimally invasive discectomy. Neurosurgery. 2002; 51:5 Suppl. S137–S145.
Article12. Akbary K, Kim JS, Park CW, Jun SG, Hwang JH. Biportal endoscopic decompression of exiting and traversing nerve roots through a single interlaminar window using a contralateral approach: technical feasibilities and morphometric changes of the lumbar canal and foramen. World Neurosurg. 2018; 117:153–161.
Article13. Rankin TM, Giovinco NA, Cucher DJ, Watts G, Hurwitz B, Armstrong DG. Three-dimensional printing surgical instruments: are we there yet? J Surg Res. 2014; 189:193–197.
Article14. Wu AM, Shao ZX, Wang JS, Yang XD, Weng WQ, Wang XY, et al. The accuracy of a method for printing three-dimensional spinal models. PLoS One. 2015; 10:e0124291.
Article15. Wu XB, Wang JQ, Zhao CP, Sun X, Shi Y, Zhang ZA, et al. Printed three-dimensional anatomic templates for virtual preoperative planning before reconstruction of old pelvic injuries: initial results. Chin Med J (Engl). 2015; 128:477–482.
Article16. Adams F, Qiu T, Mark A, Fritz B, Kramer L, Schlager D, et al. Soft 3D-printed phantom of the human kidney with collecting system. Ann Biomed Eng. 2017; 45:963–972.
Article17. Xu N, Wei F, Liu X, Jiang L, Cai H, Li Z, et al. Reconstruction of the upper cervical spine using a personalized 3D-printed vertebral body in an adolescent with Ewing sarcoma. Spine (Phila Pa 1976). 2016; 41:E50–E54.
Article18. Kim D, Lim JY, Shim KW, Han JW, Yi S, Yoon DH, et al. Sacral reconstruction with a 3D-printed implant after hemisacrectomy in a patient with sacral osteosarcoma: 1-year follow-up result. Yonsei Med J. 2017; 58:453–457.
Article19. Spetzger U, Frasca M, König SA. Surgical planning, manufacturing and implantation of an individualized cervical fusion titanium cage using patient-specific data. Eur Spine J. 2016; 25:2239–2246.
Article20. George M, Aroom KR, Hawes HG, Gill BS, Love J. 3D printed surgical instruments: the design and fabrication process. World J Surg. 2017; 41:314–319.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Application of Solid Model Based on Trabecular Tibia Bone CT Images Created by 3D Printer
- Utilization of desktop 3D printer-fabricated “Cost-Effective” 3D models in orthognathic surgery
- Three-Dimensional Bio-Printing Equipment Technologies for Tissue Engineering and Regenerative Medicine
- Clinical Application of Three-Dimensional Printing Technology in Craniofacial Plastic Surgery
- Three-Dimensional Printing Technology in Orthopedic Surgery
