Preoperative Coiling of Coexisting Intracranial Aneurysm and Subsequent Brain Tumor Surgery
- Affiliations
-
- 1Department of Neurosurgery, Severance Hospital, Yonsei University College of Medicine, Seoul 03722, Korea.
- 2Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul 03722, Korea. bmoon21@hanmail.net
- KMID: 2466290
- DOI: http://doi.org/10.3348/kjr.2016.17.6.931
Abstract
OBJECTIVE
Few studies have investigated treatment strategies for brain tumor with a coexisting unruptured intracranial aneurysm (cUIA). The purpose of this study was to evaluate the safety and efficacy of preoperative coiling for cUIA, and subsequent brain tumor surgery.
MATERIALS AND METHODS
A total of 19 patients (mean age, 55.2 years; M:F = 4:15) underwent preoperative coiling for 23 cUIAs and subsequent brain tumor surgery. Primary brain tumors were meningiomas (n = 7, 36.8%), pituitary adenomas (n = 7, 36.8%), gliomas (n = 3, 15.8%), vestibular schwannoma (n = 1, 5.3%), and Rathke's cleft cyst (n = 1, 5.3%). cUIAs were located at the distal internal carotid artery (n = 9, 39.1%), anterior cerebral artery (n = 8, 34.8%), middle cerebral artery (n = 4, 17.4%), basilar artery top (n = 1, 4.3%), and posterior cerebral artery, P1 segment (n = 1, 4.3%). The outcomes of preoperative coiling of cUIA and subsequent brain tumor surgery were retrospectively evaluated.
RESULTS
Single-microcatheter technique was used in 13 cases (56.5%), balloon-assisted in 4 cases (17.4%), double-microcatheter in 4 cases (17.4%), and stent-assisted in 2 cases (8.7%). Complete cUIA occlusion was achieved in 18 cases (78.3%), while residual neck occurred in 5 cases (21.7%). The only coiling-related complication was 1 transient ischemic attack (5.3%). Neurological deterioration did not occur in any patient during the period between coiling and tumor surgery. At the latest clinical follow-up (mean, 29 months; range, 2-120 months), 15 patients (78.9%) had favorable outcomes (modified Rankin Scale, 0-2), while 4 patients (21.1%) had unfavorable outcomes due to consequences of brain tumor surgery.
CONCLUSION
Preoperative coiling and subsequent tumor surgery was safe and effective, making it a reasonable treatment option for patients with brain tumor and cUIA.
Keyword
MeSH Terms
Figure
-

Fig. 1 53-year-old woman presenting with pituitary adenoma and coexisting unruptured aneurysm. A. Coronal view of T2 weighted MRI shows 5.3-mm sized aneurysm (arrow) buried in PA. Arrowheads indicate right internal carotid artery. B. Oblique coronal view of flat panel angiographic CT shows small aneurysm (arrow) arising from right internal carotid artery, with dome buried in PA. C. Control angiogram after coiling shows complete aneurysm occlusion. D. 6-month follow-up MR angiogram shows complete occlusion state of aneurysm (white arrow). PA = pituitary adenoma

Fig. 2 55-year-old man presenting with high grade glioma and concurrent unruptured aneurysm. A. Axial view of T2 weighted MRI shows 7.7-mm sized aneurysm (arrow) at anterior communicating artery and brain tumor with cystic portion (T) in left frontotemporal region. Note dome of aneurysm is toward brain tumor. B. Working projection view of angiogram during coiling. C. Control angiogram after coiling shows complete occlusion of aneurysm. D. Axial view of T2 weighted MRI after tumor surgery. Arrow indicated coiled aneurysm.
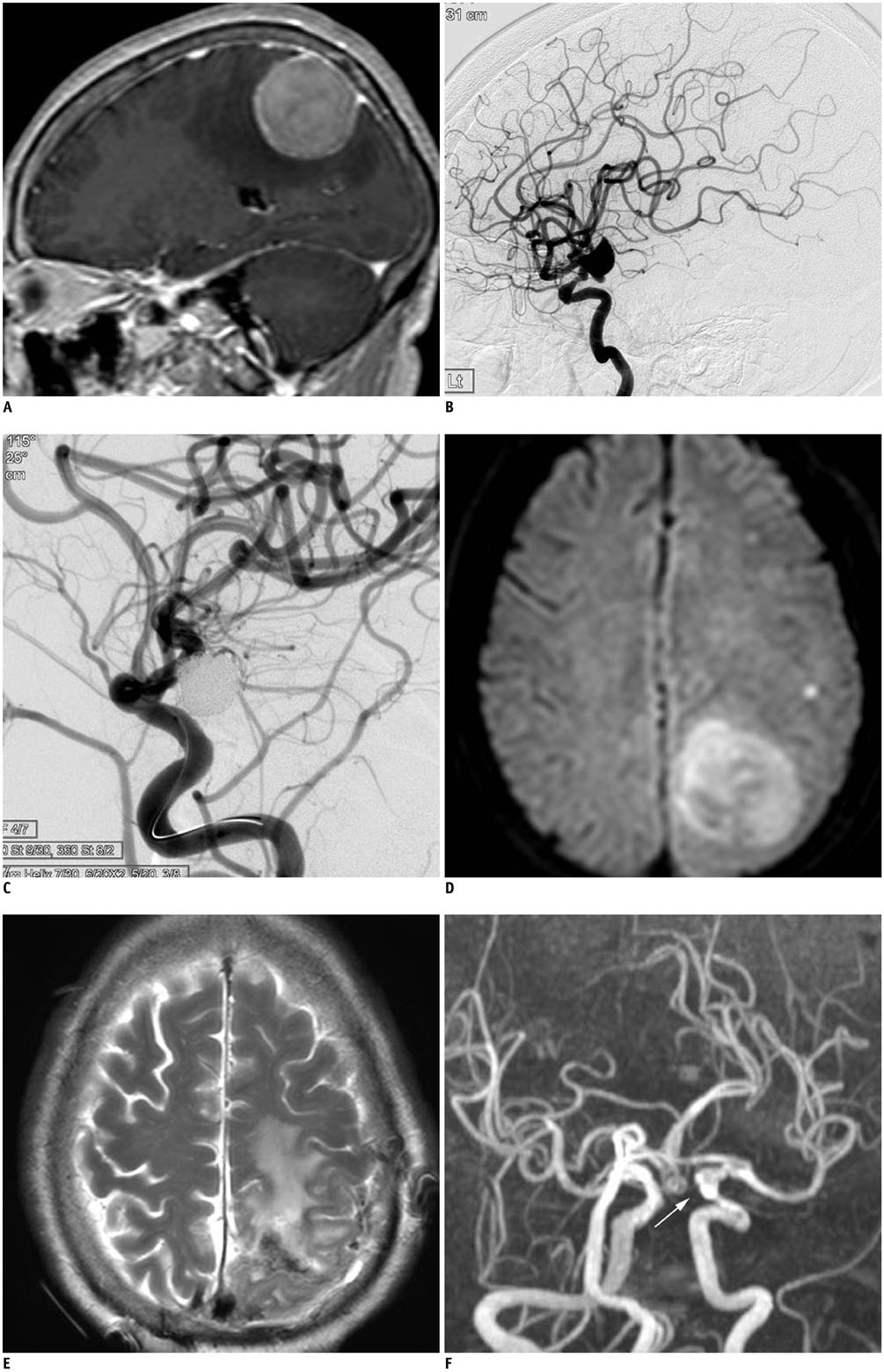
Fig. 3 68-year-old woman presenting with left parietal convexity meningioma and coexisting unruptured aneurysm. A. Sagittal view of enhanced MR shows meningioma with peritumoral edema in left parietal convexity. B. Lateral projection of left internal carotid angiogram shows large aneurysm with daughter sac at left posterior communicating artery origin. C. Control angiogram after coiling shows complete aneurysm occlusion. D. MR-DWI obtained due to transient ischemic attack (grade 4 contralateral hemiparesis) shows several high signal spots. MR-DWI = magnetic resonance diffusion weighted imaging E. Axial view of T2 weighted MRI after tumor removal. Patient had grade 4 contralateral weakness after brain tumor surgery, but recovered over several weeks. F. 2-year follow-up MR angiogram shows complete occlusion state of aneurysm (white arrow). 2-year Functional status of this patient was mRS 1. mRS = modified Rankin Scale
Reference
-
1. Tsuchida T, Tanaka R, Yokoyama M, Sato H. Rupture of anterior communicating artery aneurysm during transsphenoidal surgery for pituitary adenoma. Surg Neurol. 1983; 20:67–70.2. Taylor PE. Delayed postoperative hemorrhage from intracranial aneurysm after craniotomy for tumor. Neurology. 1961; 11:225–231.3. Javalkar V, Guthikonda B, Vannemreddy P, Nanda A. Association of meningioma and intracranial aneurysm: report of five cases and review of literature. Neurol India. 2009; 57:772–776.4. Oh MC, Kim EH, Kim SH. Coexistence of intracranial aneurysm in 800 patients with surgically confirmed pituitary adenoma. J Neurosurg. 2012; 116:942–947.5. Oshino S, Nishino A, Suzuki T, Arita H, Tateishi A, Matsumoto K, et al. Prevalence of cerebral aneurysm in patients with acromegaly. Pituitary. 2013; 16:195–201.6. Pant B, Arita K, Kurisu K, Tominaga A, Eguchi K, Uozumi T. Incidence of intracranial aneurysm associated with pituitary adenoma. Neurosurg Rev. 1997; 20:13–17.7. Fischer BR, Palkovic S, Holling M, Niederstadt T, Jeibmann A, Wassmann H. Coexistence of cerebral aneurysm and meningioma--pure accident? Clin Neurol Neurosurg. 2009; 111:647–654.8. Jakubowski J, Kendall B. Coincidental aneurysms with tumours of pituitary origin. J Neurol Neurosurg Psychiatry. 1978; 41:972–979.9. Kim YH, Lee YJ, Han JH, Ahn S, Lee J, Kim JH, et al. Association of intracranial aneurysms and meningiomas: a case-control study. J Neurosurg. 2015; 123:357–361.10. Akutsu N, Hosoda K, Ohta K, Tanaka H, Taniguchi M, Kohmura E. Subarachnoid hemorrhage due to rupture of an intracavernous carotid artery aneurysm coexisting with a prolactinoma under cabergoline treatment. J Neurol Surg Rep. 2014; 75:e73–e76.11. Cheng WY, Shen CC. Minimally invasive approaches to treat simultaneous occurrence of glioblastoma multiforme and intracranial aneurysm -- case report. Minim Invasive Neurosurg. 2004; 47:181–185.12. Hoya K, Yoshimoto Y, Shin M, Nemoto S. Rupture of an internal carotid artery aneurysm within a clinoidal meningioma following stereotactic radiosurgery. Acta Neurochir (Wien). 2011; 153:1995–1996.13. Rustagi T, Uy EM, Rai M, Kannan S, Senatus P. Intracranial hemorrhage from undetected aneurysmal rupture complicating transphenoidal pituitary adenoma resection. Conn Med. 2011; 75:393–398.14. Berker M, Aghayev K, Saatci I, Palaoğlu S, Onerci M. Overview of vascular complications of pituitary surgery with special emphasis on unexpected abnormality. Pituitary. 2010; 13:160–167.15. Zhong Z, Sun Y, Lin D, Sun Q, Bian L. Surgical treatment of brain tumor coexisted with intracranial aneurysm--case series and review of the literature. Neurosurg Rev. 2013; 36:645–656. discussion 656.16. Licata C, Pasqualin A, Freschini A, Barone G, Da Pian R. Management of associated primary cerebral neoplasms and vascular malformations: 1. intracranial aneurysms. Acta Neurochir (Wien). 1986; 82:28–38.17. Yamada S, Yamada SM, Hirohata T, Ishii Y, Hoya K, Murakami M, et al. Endoscopic extracapsular removal of pituitary adenoma: the importance of pretreatment of an adjacent unruptured internal carotid artery aneurysm. Case Rep Neurol Med. 2012; 2012:891847.18. Xia X, Ramanathan M, Orr BA, Salmasi V, Salvatori R, Reh DD, et al. Expanded endonasal endoscopic approach for resection of a growth hormone-secreting pituitary macroadenoma coexistent with a cavernous carotid artery aneurysm. J Clin Neurosci. 2012; 19:1437–1441.19. Yu K, Herwadkar A, Kearney T, Gnanalingham KK. Pituitary adenoma and incidental superior hypophyseal aneurysm. Br J Neurosurg. 2011; 25:432–433.20. Cho YD, Rhim JK, Kang HS, Park JJ, Jeon JP, Kim JE, et al. Use of triple microcatheters for endovascular treatment of wide-necked intracranial aneurysms: a single center experience. Korean J Radiol. 2015; 16:1109–1118.21. Cho YD, Rhim JK, Park JJ, Jeon JS, Yoo RE, Kang HS, et al. Microcatheter looping to facilitate aneurysm selection in coil embolization of paraclinoid aneurysms. Korean J Radiol. 2015; 16:899–905.22. Kim BM, Shin YS, Baik MW, Lee DH, Jeon P, Baik SK, et al. Pipeline embolization device for large/giant or fusiform aneurysms: an initial multi-center experience in Korea. Neurointervention. 2016; 11:10–17.23. Kwon WH, Jeong HW, Kim ST, Seo JH. Angiographic and clinical result of endovascular treatment in paraclinoid aneurysms. Neurointervention. 2014; 9:83–88.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Life-threatening Blood-Brain Barrier Disruption after Coiling of Unruptured Intracranial Aneurysm: Role of Immediate Postembolization CT scanning
- Coiling as Retreatment in Intracranial Aneurysm of de novo Formation or Regrowth: Case Report
- Current Update on the Randomized Controlled Trials of Intracranial Aneurysms
- Delayed Self-expansion Phenomenon as a Complication of Neuroform Stent Assisted Coiling for Ruptured Intracranial Aneurysm
- Comprehension of Two Modalities: Endovascular Coiling and Microsurgical Clipping in Treatment of Intracranial Aneurysms
