Efficacy of Retrievable Metallic Stent with Fixation String for Benign Stricture after Upper Gastrointestinal Surgery
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul 03080, Korea. angiointervention@gmail.com
- KMID: 2466286
- DOI: http://doi.org/10.3348/kjr.2016.17.6.893
Abstract
OBJECTIVE
To determine the efficacy of retrievable metallic stent with fixation string for benign anastomotic stricture after upper gastrointestinal (UGI) surgery.
MATERIALS AND METHODS
From June 2009 to May 2015, a total of 56 retrievable metallic stents with fixation string were placed under fluoroscopy guidance in 42 patients who were diagnosed with benign anastomotic stricture after UGI surgery. Clinical success was defined as achieving normal regular diet (NRD).
RESULTS
The clinical success rate after the first stent placement was 57.1% (24/42). After repeated stent placement and/or balloon dilation, the clinical success rate was increased to 83.3% (35/42). Six (14.3%) patients required surgical revision to achieve NRD. One (2.4%) patient failed to achieve NRD. Stent migration occurred in 60.7% (34/56) of patients. Successful rate of removing the stent using fixation string and angiocatheter was 94.6% (53/56). Distal migration occurred in 12 stents. Of the 12 stents, 10 (83.3%) were successfully removed whereas 2 could not be removed. No complication occurred regarding distal migration.
CONCLUSION
Using retrievable metallic stent with a fixation string is a feasible option for managing early benign anastomotic stricture after UGI surgery. It can reduce complications caused by distal migration of the stent.
MeSH Terms
Figure
-
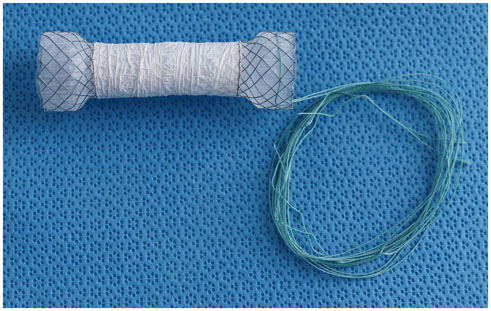
Fig. 1 Stent used in this study. It is composed of single thread of 0.1778 mm nitinol wire. It is fully covered with silicone and polytetrafluoroethylene. Both ends of stent are flared. Polyester string is wrapped around proximal end of stent body. Diameter of stent body is 20 mm. Diameter of proximal or distal end is 28 mm.

Fig. 2 Anterior (A) and oblique (B) view showing how to fix string after stent placement. String outside body is covered by Nelaton tube to reduce pain of nostril and ear. End of string was wound around gauze and anchored around ear using tape to prevent distal migration of stent.

Fig. 3 58-year-old female who had undergone gastrojejunostomy for gastrointestinal stromal tumor of stomach received repositioning of distally migrated stent. A. 20 × 120 mm retrievable stent with string was placed at anastomotic stricture site. Plain radiography obtained 5 days after stent placement revealed complete distal migration of stent. B. 7F guiding catheter was introduced over string to reach proximal end of migrated stent. C. String was pulled and stent was repositioned proximally with guiding catheter. D. When stent was repositioned at original location, string was released and guiding catheter was removed from body.
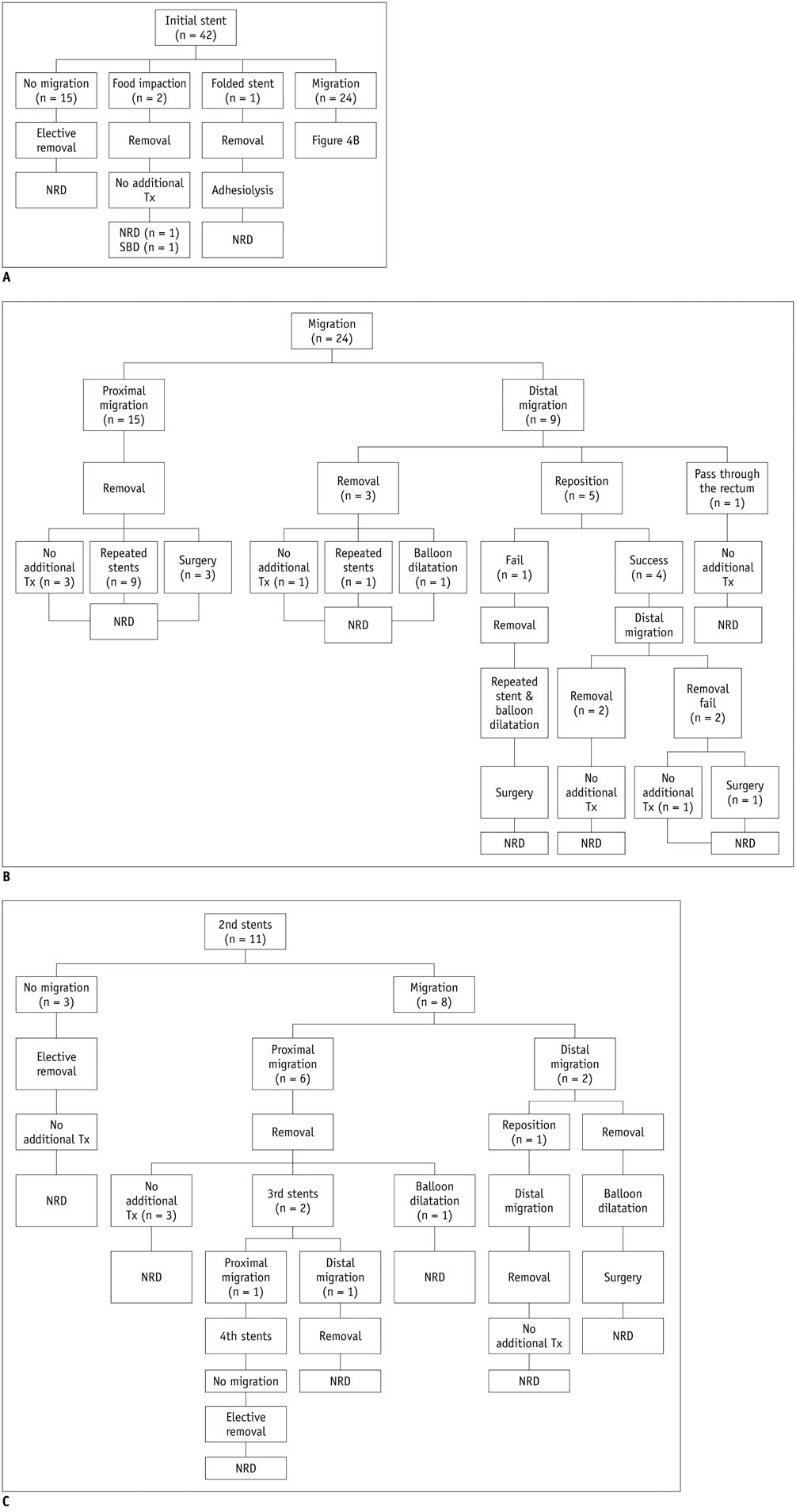
Fig. 4 Clinical outcome of study population. A. Results of 42 initially placed stents. B. Results of 24 migrated initial stents. NRD = normal regular diet, SBD = soft blend diet, Tx = treatment C. Results of 14 repeated stents. NRD = normal regular diet
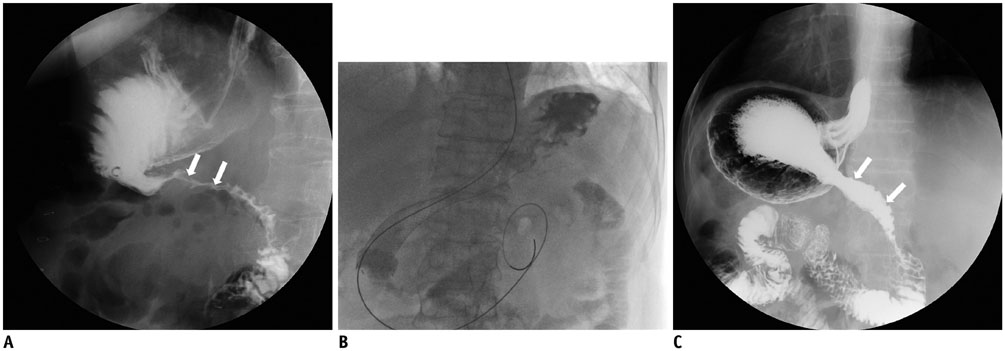
Fig. 5 63-year-old man with anastomotic stricture after Billroth I subtotal gastrectomy for gastric lipoma. A. UGI study obtained 8 days after surgery showing segmental narrowing (arrows) at anastomotic site with passage disturbance. B. 20 × 120 mm retrievable stent was placed covering stricture site. C. Stent was removed electively 20 days after placement. Follow-up UGI study obtained after stent removal showed widened previous stricture site (arrows) and good passage of contrast medium. UGI = upper gastrointestinal
Reference
-
1. Kim JH, Song HY, Park SW, Yoon CJ, Shin JH, Yook JH, et al. Early symptomatic strictures after gastric surgery: palliation with balloon dilation and stent placement. J Vasc Interv Radiol. 2008; 19:565–570.2. Palermo M, Acquafresca PA, Rogula T, Duza GE, Serra E. Late surgical complications after gastric by-pass: a literature review. Arq Bras Cir Dig. 2015; 28:139–143.3. Kim JH, Shin JH, Song HY. Fluoroscopically guided balloon dilation for benign anastomotic stricture in the upper gastrointestinal tract. Korean J Radiol. 2008; 9:364–370.4. Kim JH, Shin JH, Di ZH, Ko GY, Yoon HK, Sung KB, et al. Benign duodenal strictures: treatment by means of fluoroscopically guided balloon dilation. J Vasc Interv Radiol. 2005; 16:543–548.5. Song HY, Jung HY, Park SI, Kim SB, Lee DH, Kang SG, et al. Covered retrievable expandable nitinol stents in patients with benign esophageal strictures: initial experience. Radiology. 2000; 217:551–557.6. Yaffee DW, Solomon B, Xia Y, Grossi EA, Zervos MD, Bizekis CS. Initial outcomes of symmetrically flared covered nitinol stents for esophageal pathologies. Surg Laparosc Endosc Percutan Tech. 2015; 25:420–423.7. Ko HK, Song HY, Shin JH, Lee GH, Jung HY, Park SI. Fate of migrated esophageal and gastroduodenal stents: experience in 70 patients. J Vasc Interv Radiol. 2007; 18:725–732.8. Song HY, Lee DH, Seo TS, Kim SB, Jung HY, Kim JH, et al. Retrievable covered nitinol stents: experiences in 108 patients with malignant esophageal strictures. J Vasc Interv Radiol. 2002; 13:285–293.9. Eloubeidi MA, Talreja JP, Lopes TL, Al-Awabdy BS, Shami VM, Kahaleh M. Success and complications associated with placement of fully covered removable self-expandable metal stents for benign esophageal diseases (with videos). Gastrointest Endosc. 2011; 73:673–681.10. Kim HC, Han JK, Kim TK, Do KH, Kim HB, Park JH, et al. Duodenal perforation as a delayed complication of placement of an esophageal stent. J Vasc Interv Radiol. 2000; 11:902–904.11. Henne TH, Schaeff B, Paolucci V. Small-bowel obstruction and perforation. A rare complication of an esophageal stent. Surg Endosc. 1997; 11:383–338.12. Zhang W, Meng WJ, Zhou ZG. Multiple perforations of the jejunum caused by a migrated esophageal stent. Endoscopy. 2011; 43:Suppl 2 UCTN. E145–E146.13. Moxey PW, Khan AZ, Karanjia ND. A case of small-bowel perforation caused by a migrated duodenal stent. Endoscopy. 2007; Suppl 1. 39:E54.14. Karatepe O, Acet E, Altiok M, Battal M, Adas G, Karahan S. Esophageal stent migration can lead to intestinal obstruction. N Am J Med Sci. 2009; 1:63–65.15. Endo M, Kaminou T, Ohuchi Y, Sugiura K, Yata S, Adachi A, et al. Development of a new hanging-type esophageal stent for preventing migration: a preliminary study in an animal model of esophagotracheal fistula. Cardiovasc Intervent Radiol. 2012; 35:1188–1194.16. Lyons CD, Kim MP, Blackmon SH. A novel fixation procedure to eliminate covered self-expanding metal stent migration. Ann Thorac Surg. 2012; 94:1748–1750.17. Bae JS, Kim SH, Shin CI, Joo I, Yoon JH, Lee HJ, et al. Efficacy of gastric balloon dilatation and/or retrievable stent insertion for pyloric spasms after pyloruspreserving gastrectomy: retrospective analysis. PLoS One. 2015; 10:e0144470.18. Bae JI, Shin JH, Song HY, Lee GH. Treatment of a benign anastomotic duodenojejunal stricture with a polytetrafluoroethylene-covered retrievable expandable nitinol stent. J Vasc Interv Radiol. 2004; 15:769–772.19. Kim HC, Shin JH, Song HY, Park SI, Ko GY, Youn HK, et al. Fluoroscopically guided balloon dilation for benign anastomotic stricture after Ivor-Lewis esophagectomy: experience in 62 patients. J Vasc Interv Radiol. 2005; 16:1699–1704.20. Kim JH, Shin JH, Bae JI, Di ZH, Lim JO, Kim TH, et al. Gastric outlet obstruction caused by benign anastomotic stricture: treatment by fluoroscopically guided balloon dilation. J Vasc Interv Radiol. 2005; 16:699–704.21. Zhang J, Ren L, Huo J, Zhu Z, Liu D. The use of retrievable fully covered self-expanding metal stent in refractory postoperative restenosis of benign esophageal stricture in children. J Pediatr Surg. 2013; 48:2235–2240.22. Kim JH, Song HY, Choi EK, Kim KR, Shin JH, Lim JO. Temporary metallic stent placement in the treatment of refractory benign esophageal strictures: results and factors associated with outcome in 55 patients. Eur Radiol. 2009; 19:384–390.23. Chung KH, Lee SH, Park JM, Lee JM, Shin CM, Ahn SH, et al. Partially covered self-expandable metallic stent for postoperative benign strictures associated with laparoscopy-assisted gastrectomy. Gastric Cancer. 2016; 19:280–286.24. Gangloff A, Lecleire S, Di Fiore A, Huet E, Iwanicki-Caron I, Antonietti M, et al. Fully versus partially covered self-expandable metal stents in benign esophageal strictures. Dis Esophagus. 2015; 28:678–683.25. Park JH, Song HY, Shin JH, Cho YC, Kim JH, Kim SH, et al. Migration of retrievable expandable metallic stents inserted for malignant esophageal strictures: incidence, management, and prognostic factors in 332 patients. AJR Am J Roentgenol. 2015; 204:1109–1114.26. Choi WJ, Park JJ, Park J, Lim EH, Joo MK, Yun JW, et al. Effects of the temporary placement of a self-expandable metallic stent in benign pyloric stenosis. Gut Liver. 2013; 7:417–422.27. Yoon CJ, Shin JH, Song HY, Lim JO, Yoon HK, Sung KB. Removal of retrievable esophageal and gastrointestinal stents: experience in 113 patients. AJR Am J Roentgenol. 2004; 183:1437–1444.28. Cheng YS, Li MH, Chen WX, Chen NW, Zhuang QX, Shang KZ. Complications of stent placement for benign stricture of gastrointestinal tract. World J Gastroenterol. 2004; 10:284–286.29. Song HY, Park SI, Do YS, Yoon HK, Sung KB, Sohn KH, et al. Expandable metallic stent placement in patients with benign esophageal strictures: results of long-term follow-up. Radiology. 1997; 203:131–136.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Self-Expandable Metallic Stent Therapy for a Gastrointestinal Benign Stricture
- Gastrointestinal Stent Update
- Stent Flange-Induced Esophageal Stricture Treated with an Oral Steroid
- Percutaneous Transhepatic Treatment of Benign Bile Duct Strictures Using Retrievable Covered Stents: Long-Term Outcomes in 148 Patients
- A Case of Aortoesophageal Fistula Complicated by a Stent for Benign Esophageal Stricture
