Dorsal Track Control (DTC): A Modified Surgical Technique for Atraumatic Handling of the Distal Esophagus in Esophagojejunostomy
- Lehwald-Tywuschik N

- Steinfurth F
- Kröpil F
- Krieg A
- Sarikaya H
- Knoefel WT
- Krüger M
- Benhidjeb
- Beshay M
- Schulte am Esch J
- Affiliations
-
- 1Department of Surgery, University Hospital Düsseldorf, Düsseldorf, Germany.
- 2Center of Visceral Medicine, Department of General and Visceral Surgery, Protestant Hospital of Bethel Foundation, Bielefeld, Germany. jan.schulteamEsch@evkb.de
- 3Center of Visceral Medicine, Department of Gastroenterology and Internal Medicine, Protestant Hospital of Bethel Foundation, Bielefeld, Germany.
- 4Department of Thoracic Surgery, Protestant Hospital of Bethel Foundation, Bielefeld, Germany.
- KMID: 2466035
- DOI: http://doi.org/10.5230/jgc.2019.19.e35
Abstract
- Surgical therapy for adenocarcinoma of the esophagogastric junction II requires distal esophagectomy, in which a transhiatal management of the lower esophagus is critical. The "˜dorsal track control' (DTC) maneuver presented here facilitates the atraumatic handling of the distal esophagus, in preparation for a circular-stapled esophagojejunostomy. It is based on a ventral semicircular incision in the distal esophagus, with an intact dorsal wall for traction control of the esophagus. The maneuver facilitates the proper placement of the purse-string suture, up to its tying (around the anvil), thus minimizing the manipulation of the remaining esophagus. Furthermore, the dorsally-exposed inner wall surface of the ventrally-opened esophagus serves as a guiding chute that eases anvil insertion into the esophageal lumen. We performed this novel technique in 21 cases, enabling a safe anastomosis up to 10 cm proximal to the Z-line. No anastomotic insufficiency was observed. The DTC technique improves high transhiatal esophagojejunostomy.
MeSH Terms
Figure
-
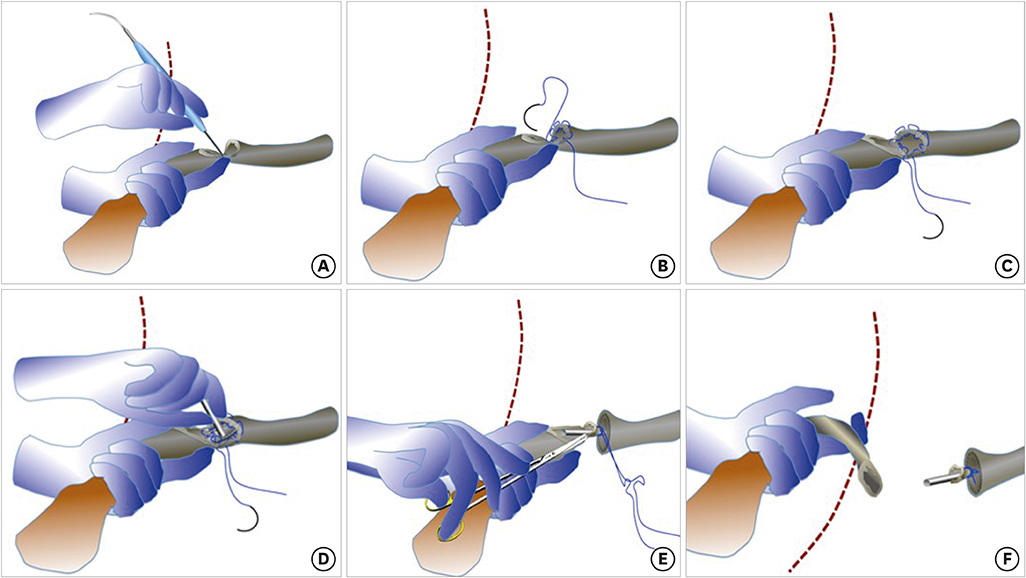
Fig. 1 Description of the DTC maneuver. (A) Transhiatal approach with lower mediastinal en-bloc lymphadenectomy. Ventral semi-circular incision in the esophagus at a level that provides a safety margin of minimum 5 cm cranial to the oral tumor. The posterior esophageal wall remains intact for traction control of the esophagus (naso-gastric tube in place). (B and C) Controlled positioning of the purse-string suture avoiding any manipulation of the remaining intrathoracic esophagus. One hand gently pulls down the esophagus by the posterior wall with DTC. (D) The dorsally-exposed epithelialized inner wall surface of the ventrally-opened esophagus serves as a guiding chute to ease the insertion of the anvil into the upper esophageal lumen; this is paralleled by preventing the retraction of the esophageal end towards the upper mediastinum. (E) Following the insertion of the circular stapler anvil into the upper esophageal lumen, the anvil attachment is tied by the purse string-suture. (F) Following the purse-string suture tie around the anvil attachment, the distal esophagus is cut just below. DTC = dorsal track control.

Fig. 2 Intraoperative pictures for extended gastrectomy. (A) Semi-circular opening of the ventral esophagus with a safety margin of minimum 5 cm cranial to the oral tumor (naso-gastric tube in place). (B) The purse-string suture is carefully placed, under observation, by avoiding any manipulation of the esophagus stump. (C) The anastomosis will be placed up to 10 cm intrathoracic in the mid mediastinum.
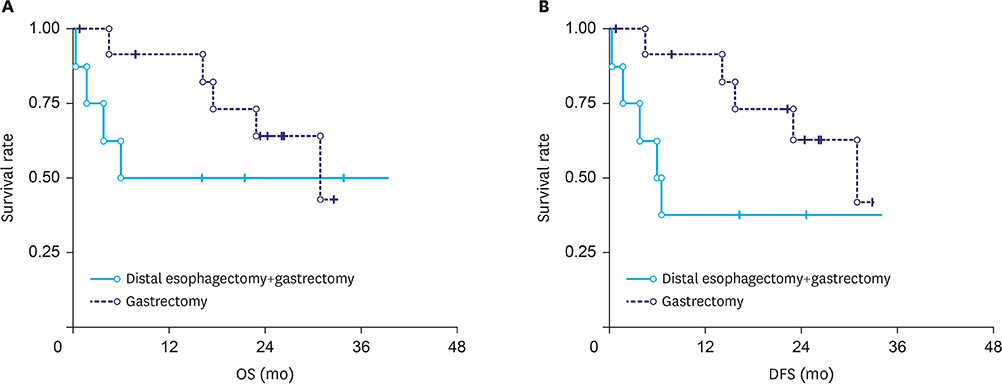
Fig. 3 Kaplan–Meier survival curve demonstrates similar OS and DFS rates in groups I (gastrectomy only, n=12) and II (gastrectomy + distal esophagectomy, n=8). OS = overall survival; DFS = disease free survival.

Fig. 4 Pre-(left panels) and post-(right panels) operative thoraco-abdominal computed tomography-scans of 1 patient operated with the dorsal track control technique (blue ovals—localization of the adenocarcinoma of the esophagogastric junction II; yellow arrows—position of the intrathoracic esophagojejunostomy after transhiatal extended gastrectomy). Pre-op = pre-operative; Post-op = post-operative.
Reference
-
1. Orditura M, Galizia G, Lieto E, De Vita F, Ciardiello F. Treatment of esophagogastric junction carcinoma: an unsolved debate. World J Gastroenterol. 2015; 21:4427–4431.2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63:11–30.3. Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996; 335:462–467.4. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991; 265:1287–1289.5. Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998; 85:1457–1459.6. Rüdiger Siewert J, Feith M, Werner M, Stein HJ. Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg. 2000; 232:353–361.7. Lee IS, Ahn JY, Yook JH, Kim BS. Mediastinal lymph node dissection and distal esophagectomy is not essential in early esophagogastric junction adenocarcinoma. World J Surg Oncol. 2017; 15:28.8. Heger P, Blank S, Gooßen K, Nienhüser H, Diener MK, Ulrich A, et al. Thoracoabdominal versus transhiatal surgical approaches for adenocarcinoma of the esophagogastric junction-a systematic review and meta-analysis. Langenbecks Arch Surg. 2019; 404:103–113.9. Schröder W, Lambertz R, van Hillegesberger R, Bruns C. Differentiated surgical approach for adenocarcinoma of the gastroesophageal junction. Chirurg. 2017; 88:1010–1016.10. Walther BS, Zilling T, Johnsson F, Staël von Holstein C, Joelsson B. Total gastrectomy and oesophagojejunostomy with linear stapling devices. Br J Surg. 1989; 76:909–912.11. Guerra JP, Silva MH, dos Santos JG. An improved technique for a stapled transabdominal esophagojejunostomy. Am J Surg. 1997; 174:61–62.12. Robinson LA, Moulton AL, Fleming WH. Techniques to simplify esophagogastric circular stapled anastomoses. J Surg Oncol. 1994; 57:266–269.13. Hiki N, Fukunaga T, Yamaguchi T, Nunobe S, Tokunaga M, Ohyama S, et al. Laparoscopic esophagogastric circular stapled anastomosis: a modified technique to protect the esophagus. Gastric Cancer. 2007; 10:181–186.14. Ulrich B, Zahedi A. Technical aspects and results of the transhiatal resection in adenocarcinomas of the gastroesophageal junction. Dis Esophagus. 2001; 14:115–119.15. Sato Y, Katai H, Ito M, Yura M, Otsuki S, Yamagata Y, et al. Can proximal gastrectomy be justified for advanced adenocarcinoma of the esophagogastric junction? J Gastric Cancer. 2018; 18:339–347.16. Siewert JR, Fink U, Sendler A, Becker K, Böttcher K, Feldmann HJ, et al. Gastric cancer. Curr Probl Surg. 1997; 34:835–939.17. Omori T, Oyama T, Mizutani S, Tori M, Nakajima K, Akamatsu H, et al. A simple and safe technique for esophagojejunostomy using the hemidouble stapling technique in laparoscopy-assisted total gastrectomy. Am J Surg. 2009; 197:e13–e17.18. Takiguchi S, Sekimoto M, Fujiwara Y, Miyata H, Yasuda T, Doki Y, et al. A simple technique for performing laparoscopic purse-string suturing during circular stapling anastomosis. Surg Today. 2005; 35:896–899.19. Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002; 347:1662–1669.20. Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T, et al. Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol. 2006; 7:644–651.21. Mariette C, Piessen G, Triboulet JP. Therapeutic strategies in oesophageal carcinoma: role of surgery and other modalities. Lancet Oncol. 2007; 8:545–553.22. Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003; 349:2241–2252.23. Zheng Z, Cai J, Yin J, Zhang J, Zhang ZT, Wang KL. Transthoracic versus abdominal-transhiatal resection for treating Siewert type II/III adenocarcinoma of the esophagogastric junction: a meta-analysis. Int J Clin Exp Med. 2015; 8:17167–17182.24. Walther BS, Oscarson JE, Graffner HO, Vallgren S, Evander A. Esophagojejunostomy with the EEA stapler. Surgery. 1986; 99:598–603.25. Vauthey JN, Maddern GJ, Gertsch P. A simplified technique of esophagojejunostomy. Surg Gynecol Obstet. 1991; 173:499–500.26. Lygidakis NJ. Total gastrectomy for gastric carcinoma: a retrospective study of different procedures and assessment of a new technique of gastric reconstruction. Br J Surg. 1981; 68:649–655.27. Basso N, Minervini S, Marcelli M, Di Marco M. A technical aid in stapled esophagojejunal anastomosis. Surg Gynecol Obstet. 1988; 167:525–526.28. West PN, Marbarger JP, Martz MN, Roper CL. Esophagogastrostomy with the EEA stapler. Ann Surg. 1981; 193:76–81.29. Campion JP, Grossetti D, Launois B. Circular anastomosis stapler. An alternative to pursestring suture. Arch Surg. 1984; 119:232–233.30. Alexander-Williams J. To facilitate the insertion of the EEA autosuture head into the oesophagus. Br J Surg. 1982; 69:196.31. Legaspi A, Irani H. Stapled transabdominal lower esophageal anastomosis without purse-string suture. Surg Gynecol Obstet. 1990; 170:156–158.32. Liu B, Zhang R, Tao G, Lehwald NC, Liu B, Koh Y, et al. Augmented Wnt signaling as a therapeutic tool to prevent ischemia/reperfusion injury in liver: preclinical studies in a mouse model. Liver Transpl. 2015; 21:1533–1542.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A modified free gingival graft technique for the treatment of oro-antral sinus track: A case report
- Dorsal Approach for Distal Radius Fractures
- A Novel Technique of Hand-Sewn Purse-String Suturing by Double Ligation Method (DLM) for Intracorporeal Circular Esophagojejunostomy
- Left Dorsal Wall Anastomosis Compared with Parallel-Line Anastomosis for Intracorporeal Overlap Esophagojejunostomy during Laparoscopic Total Gastrectomy
- Direct-to-consumer genetic testing
