Anesth Pain Med.
2019 Oct;14(4):489-493. 10.17085/apm.2019.14.4.489.
Laryngeal granulomas in patients after two-jaw surgery: Four cases report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Dankook University Hospital, Dankook University College of Medicine, Cheonan, Korea. skkim@dankook.ac.kr
- KMID: 2465350
- DOI: http://doi.org/10.17085/apm.2019.14.4.489
Abstract
- BACKGROUND
Endotracheal intubation can cause focal ischemia, damage or edema to the laryngeal mucosa, and may be followed by serious complications such as vocal cord paralysis, ulcers, and granulation tissue formation. Laryngeal granuloma is rare but also a significant late complication of endotracheal intubation, and anesthesiologists should be concerned about it. CASE: We experienced four cases of laryngeal granuloma that developed after two-jaw surgery January 2017-December 2018 in our hospital and would like to report these cases with brief review of literature.
CONCLUSIONS
There are frequent movements on the head and neck in maxillofacial surgery and the nasotracheal intubation should be prolonged after bimaxillary osteotomy surgery because of post-operative airway problems. This may be why two-jaw surgery may have higher occurrence of laryngeal granuloma than others.
MeSH Terms
Figure
-

Fig. 1 (A) Laryngoscopic view shows larger right-sided vocal cord granuloma (arrow) than left at three months after two-jaw surgery. (B) After laryngomicroscopic surgery the granuloma is removed.
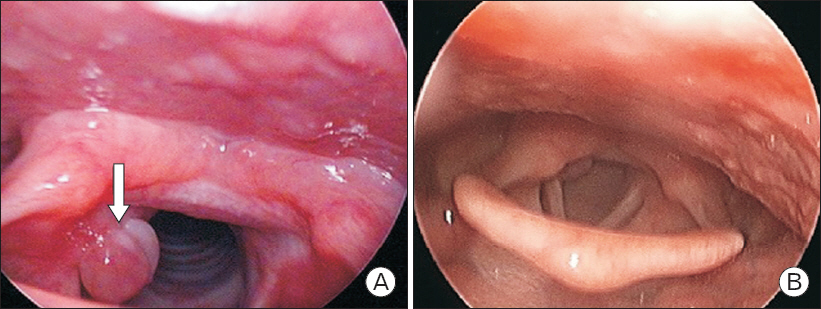
Fig. 2 (A) Laryngoscopic view shows right-sided vocal cord granuloma (arrow) one month after two-jaw surgery. (B) The granuloma decreases after conservative treatments for two weeks.
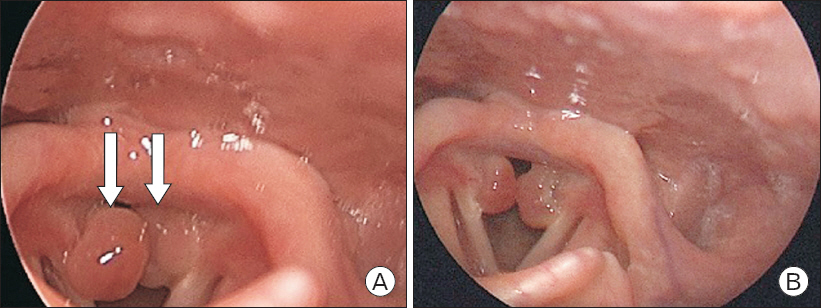
Fig. 3 (A) Laryngoscopic view shows vocal cord granuloma at both sides (arrows) four months after surgery. (B) The granuloma size decreases after conservative treatments for two months.
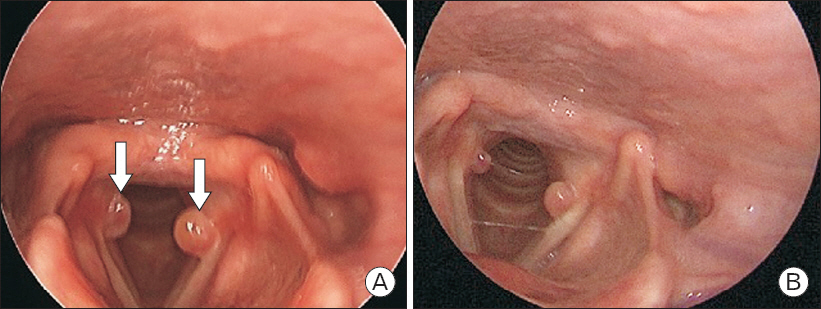
Fig. 4 (A) Laryngoscopic view shows vocal cord granuloma at both sides (arrows) five months after surgery. (B) The granuloma decreases after conservative treatment for one month.
Reference
-
1. Lemos EM, Sennes LU, Imamura R, Tsuji DH. Vocal process granuloma:clinical characterization, treatment and evolution. Braz J Otorhinolaryngol. 2005; 71:494–8. DOI: 10.1016/S1808-8694(15)31205-2. PMID: 16446966.2. Hamdan AL, Sabra O, Rameh C, El-Khatib M. Persistant dysphonia following endotracheal intubation. Middle East J Anaesthesiol. 2007; 19:5–13. PMID: 17511179.3. de Lima Pontes PA, De Biase NG, Gadelha EC. Clinical evolution of laryngeal granulomas:treatment and prognosis. Laryngoscope. 1999; 109(2 Pt 1):289–94. DOI: 10.1097/00005537-199902000-00021. PMID: 10890781.4. Clausen RJ. Unusual sequela of tracheal intubation. Proc R Soc Med. 1932; 25:1507. DOI: 10.1177/003591573202501011. PMID: 19988911. PMCID: PMC2183893.5. Blanc VF, Tremblay NA. The complications of tracheal intubation:a new classification with a review of the literature. Anesth Analg. 1974; 53:202–13. DOI: 10.1213/00000539-197403000-00005. PMID: 4593090.6. Jang M, Basa K, Levi J. Risk factors for laryngeal trauma and granuloma formation in pediatric intubations. Int J Pediatr Otorhinolaryngol. 2018; 107:45–52. DOI: 10.1016/j.ijporl.2018.01.008. PMID: 29501310.7. Kim HK, Woo NS, Jeong SM, Kwon WK. Incidentally detected laryngeal granuloma during orotracheal intubation under direct laryngoscope:a case report. Anesth Pain Med. 2010; 5:92–4.8. Park SY, Choi HS, Yoon JY, Kim EJ, Yoon JU, Kim HY, et al. Fatal vocal cord granuloma after orthognathic surgery. J Dent Anesth Pain Med. 2018; 18:375–8. DOI: 10.17245/jdapm.2018.18.6.375. PMID: 30637348. PMCID: PMC6323036.9. Rimoli CF, Martins RHG, Catâneo DC, Imamura R, Catâneo AJM. Treatment of post-intubation laryngeal granulomas:systematic review and proportional meta-analysis. Braz J Otorhinolaryngol. 2018; 84:781–9. DOI: 10.1016/j.bjorl.2018.03.003. PMID: 29699879.10. Karkos PD, George M, Van Der Veen J, Atkinson H, Dwivedi RC, Kim D, et al. Vocal process granulomas:a systematic review of treatment. Ann Otol Rhinol Laryngol. 2014; 123:314–20. DOI: 10.1177/0003489414525921. PMID: 24642585.11. Dubick MN, Wright BD. Comparison of laryngeal pathology following long-term oral and nasal endotracheal intubations. Anesth Analg. 1978; 57:663–8. DOI: 10.1213/00000539-197811000-00013. PMID: 569990.12. Kim YK. Complications associated with orthognathic surgery. J Korean Assoc Oral Maxillofac Surg. 2017; 43:3–15. DOI: 10.5125/jkaoms.2017.43.1.3. PMID: 28280704. PMCID: PMC5342970.13. Kim T, Kim JY, Woo YC, Park SG, Baek CW, Kang H. Pneumomediastinum and pneumothorax after orthognathic surgery -a case report-. Korean J Anesthesiol. 2010; 59(Suppl):242–5. DOI: 10.4097/kjae.2010.59.S.S242. PMID: 21286451. PMCID: PMC3030047.14. Choi SK, Yoon JE, Cho JW, Kim JW, Kim SJ, Kim MR. Changes of the Airway space and the position of hyoid bone after mandibular set back surgery using bilateral sagittal split ramus osteotomy technique. Maxillofac Plast Reconstr Surg. 2014; 36:185–91. DOI: 10.14402/jkamprs.2014.36.5.185. PMID: 27489832. PMCID: PMC4283530.15. Kim BY, Kong MH, Lim HJ, Chang SH, Chae BK. Clinical observation in 20 cases with intubation granuloma. Korean J Anesthesiol. 1994; 27:251–4. DOI: 10.4097/kjae.1994.27.3.251.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Synchronous Central Giant Cell Granulomas of the Maxillofacial Region: A Case Report
- Postoperative Radiation Therapy in Ameloblastoma of the Jaw: Report of Two Cases
- Jaw-thrust induces sympathetic responses during induction of general anesthesia
- Comparison of the trapezius squeezing test and jaw thrust as indicators for laryngeal mask airway insertion in adults
- A comparative study on the degree of relapse following one jaw surgery and two jaw surgery in skeletal Class III patients
