Symptomatic Sinus Pericranii with Adult Onset Headache: A Case Report with Pathologic Perspective
- Affiliations
-
- 1Department of Neurosurgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. kypark78.md@gmail.com
- 2Department of Neurosurgery, Ewha Womans University Seoul Hospital, Ewha Womans University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2465247
- DOI: http://doi.org/10.7461/jcen.2019.21.3.163
Abstract
- Sinus pericranii (SP) is a rare vascular anomaly of the scalp that consists of an abnormal pericranial venous channel connected to adjacent dural venous sinuses. Most SP are asymptomatic and are found in the pediatric age group. We aim to report a case of symptomatic SP in adult and describe the clinical, radiological, and pathohistological findings to help understand and differentiate this lesion from other scalp lesions. A 40-year-old man with a scalp mass was admitted to our hospital complaining of headache. The lesion enlarged when the patient was in a recumbent position or during Valsalva maneuver. The radiologic imaging suggested its diagnosis as an accessory type of SP with bone erosion. Surgical resection and cranioplasty were successfully performed, and the related headache also gradually subsided. At the 3-year follow-up, there was no recurrence on magnetic resonance imaging.
Keyword
MeSH Terms
Figure
-
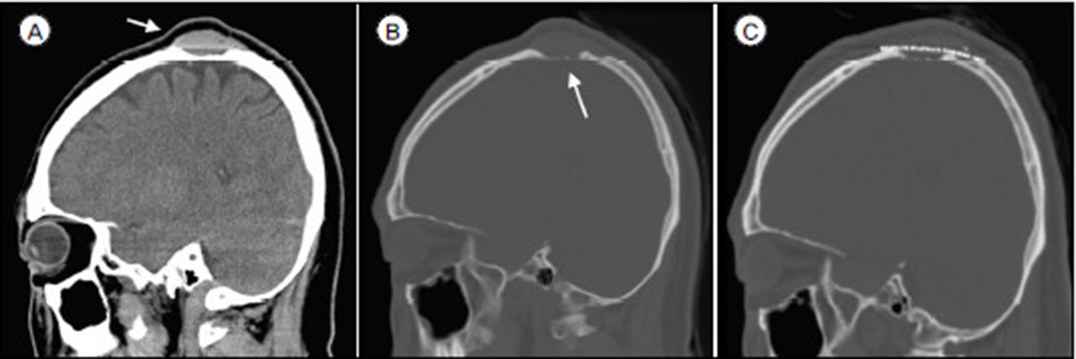
Fig. 1 Computed tomography (CT) scan. (A) Sagittal view, isodense round-shaped mass (arrow) located above the skull. (B) Sagittal view of bone window setting, the related calvarial erosion (arrow) was noted. (C) Complete removal of sinus pericranii and well-formed cranial vault with mesh plate was noted in postoperative CT scan.
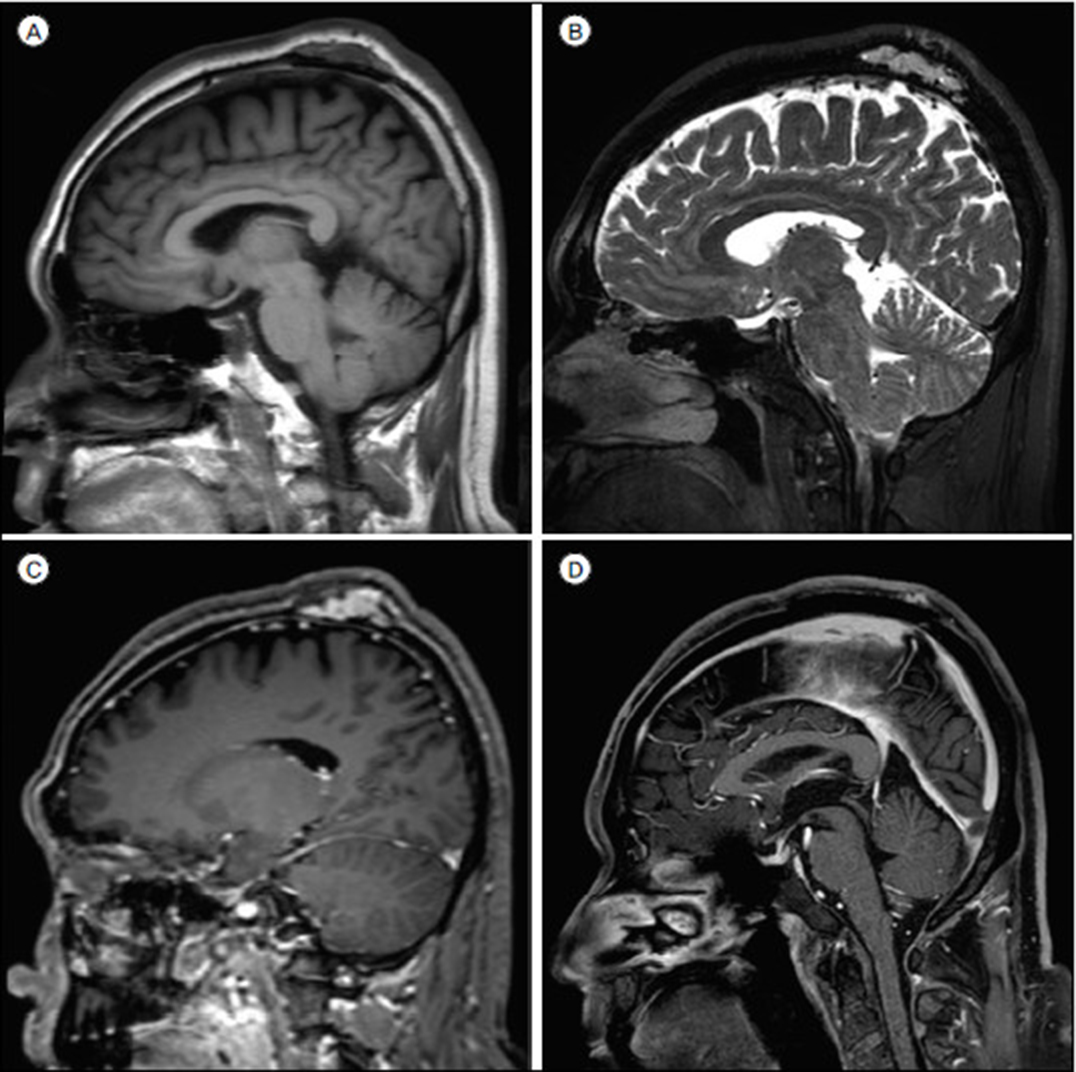
Fig. 2 Preoperative magnetic resonance (MR) imaging showed heterogenous signals and flow voids within the mass in both T1 (A) and T2 (B) weighted images. Gadolinium-enhanced T1-weighted MR imaging (C) showed a contrast-enhancing mass between galea aponeurotica and skull. Three year's follow-up gadolinium-enhanced T1-weighted MR imaging (D) showed a complete obliteration of mass without any recurrence.

Fig. 3 Digital subtraction angiography (DSA) findings of sinus pericranii (SP). (A) Internal carotid angiography lateral view; in late venous phase, a majority of the cerebral venous outflow occurred through the superior sagittal sinus (SSS, arrow). Small contrast filling of extracranial–intracranial venous channel was also identified (arrowhead). (B) External carotid angiography AP view; in late venous phase, the SP (arrowhead) was connected with SSS (arrow). (C) External carotid angiography lateral view; in late venous phase, only a part of the extracranial venous outflow was draining through the SP (arrowhead). These findings indicated an accessory type SP.

Fig. 4 Pathologic findings of sinus pericranii (SP). (A) H&E staining (× 100); it showed a single-layer flattened endothelium (arrow) with thick venous stroma (asterisk), which suggested a congenital type of SP. (B) CD-31 staining (× 100); thin brownish endothelial layers showed the vascular nature. (C) D2–40 staining (× 40); it showed the absence of lymphatic wall.
Reference
-
1. Akram H, Prezerakos G, Haliasos N, O'Donovan D, Low H. Sinus pericranii: an overview and literature review of a rare cranial venous anomaly (a review of the existing literature with case examples). Neurosurg Rev. 2012; 01. 35(1):15–26. discussion 26.
Article2. Arita K, Uozumi T, Kuwabara S, Kiya K, Sumida M, Iida K. A case of scalp cavernous hemangioma simulating sinus pericranii. Hiroshima J Med Sci. 1992; 03. 41(1):19–23.3. Bick DS, Brockland JJ, Scott AR. A scalp lesion with intracranial extension. Atretic cephalocele. JAMA Otolaryngol Head Neck Surg. 2015; 03. 141(3):289–290.4. Gandolfo C, Krings T, Alvarez H, Ozanne A, Schaaf M, Baccin CE. Sinus pericranii: diagnostic and therapeutic considerations in 15 patients. Neuroradiology. 2007; 06. 49(6):505–514.
Article5. Guler S, Tatli B. Rare vascular pathology sinus pericranii; becomes symptomatic with pseudotumor cerebri. Turk J Pediatr. 2015; Nov-Dec. 57(6):618–620.6. Kaido T, Kim YK, Ueda K. Diagnostic and therapeutic considerations for sinus pericranii. J Clin Neurosci. 2006; 08. 13(7):788–792.
Article7. Khachatrian VA, Khodorovskaia AM, Sebelev KI, Zabrodskaia IuM. Pericranial sinus. Definition, diagnosis, surgical treatment. Zh Vopr Neirokhir Im N N Burdenko. 2014; 78(3):30–37.8. Lee CH, Lee YS, Lee JH, Lee HG, Ryu KY, Kang DG. Sinus pericranii: A case report and the literature review. Korean J Cerebrovasc Surg. 2009; 12. 11(4):174–178.9. Nomura S, Kato S, Ishihara H, Yoneda H, Ideguchi M, Suzuki M. Association of intra- and extradural developmental venous anomalies, so-called venous angioma and sinus pericranii. Childs Nerv Syst. 2006; 04. 22(4):428–431.
Article10. Ota T, Waga S, Handa H, Nishimura S, Mitani T. Sinus pericranii. J Neurosurg. 1975; 06. 42(6):704–712.11. Pavanello M, Melloni I, Antichi E, Severino M, Ravegnani M, Piatelli G. Sinus pericranii: diagnosis and management in 21 pediatric patients. J Neurosurg Pediatr. 2015; 01. 15(1):60–70.
Article12. Rangel-Castilla L, Krishna C, Klucznik R, Diaz O. Endovascular embolization with Onyx in the management of sinus pericranii: a case report. Neurosurg Focus. 2009; 11. 27(5):E13.
Article13. Saba R, Senussi MH, Alwakkaf A, Brown H. Sinus pericranii in a young adult with chronic headache. BMJ Case Rep. 2013; 07. 2013:bcr2013010165.
Article14. Sadler LR, Tarr RW, Jungreis CA, Sekhar L. Sinus pericranii: CT and MR findings. J Comput Assist Tomogr. 1990; Jan-Feb. 14(1):124–127.
