Successful Mechanical Thrombectomy Using Solumbra Technique In a 35-year-old Man With Achondroplasia: a case report
- Affiliations
-
- 1Department of Neurosurgery, Deajeon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Daejeon, Republic of Korea. kope95@hanmail.net
- 2Department of Radiology, Deajeon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Daejeon, Republic of Korea.
- KMID: 2465013
- DOI: http://doi.org/10.7461/jcen.2019.21.1.33
Abstract
- BACKGROUND
Achondroplasia is one of the most common types of dwarfism and is inherited as an autosomal dominant disease. The patients with achondroplasia suffer from various complications such as craniofacial, central nervous system, spinal, respiratory and cardiac anomalies. CASE DESCRIPTION: We report a case of a 35-year-old man with achondroplasia who visited the emergency room with right hemiplegia and aphasia within 6 hours after onset. An Initial CT angiography showed the total occlusion of a left internal cerebral artery due to the thrombus. We treated the patient with endovascular thrombectomy using "Solumbra technique" with balloon guiding catheter. The procedure was successful and result was completely recanalized with Thrombolysis in Cerebral Infarction (TICI) scale 3 and the weakness also improved from grade II to grade IV.
CONCLUSION
Acute ischemic stroke patients with achondroplasia could be treated with mechanical thrombectomy.
Keyword
MeSH Terms
Figure
-
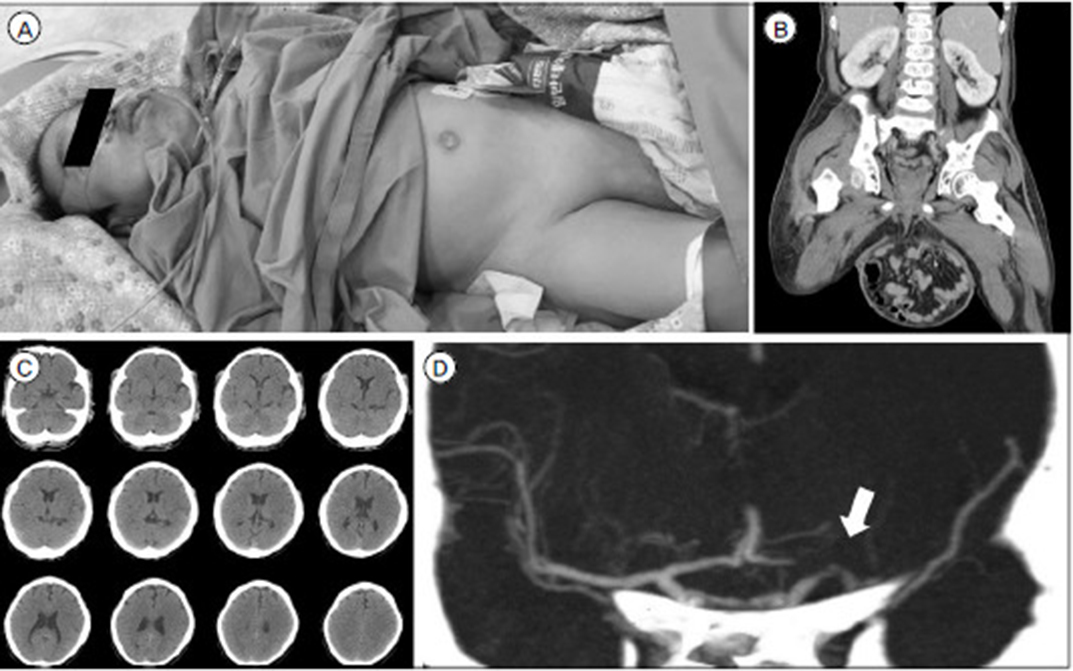
Fig. 1 (A) A 35-year-old man with achondroplasia measuring 130 cm in height visited ER with aphasia and right hemiplegia (photograph in the intervention room for the procedure). (B) Abdominal CT showed severe inguinal hernia that intestines migrated into the scrotum. (C) Initial non-enhanced CT demonstrated no evidence of hemorrhage or definite low density. (D) CT angiogram (coronal view) showed left distal ICA occlusion due to a thrombus (white arrow) and only a slight anterotemporal flow was observed, whereas ipsilateral proximal A1 and MCA distal blood flow were not detected.
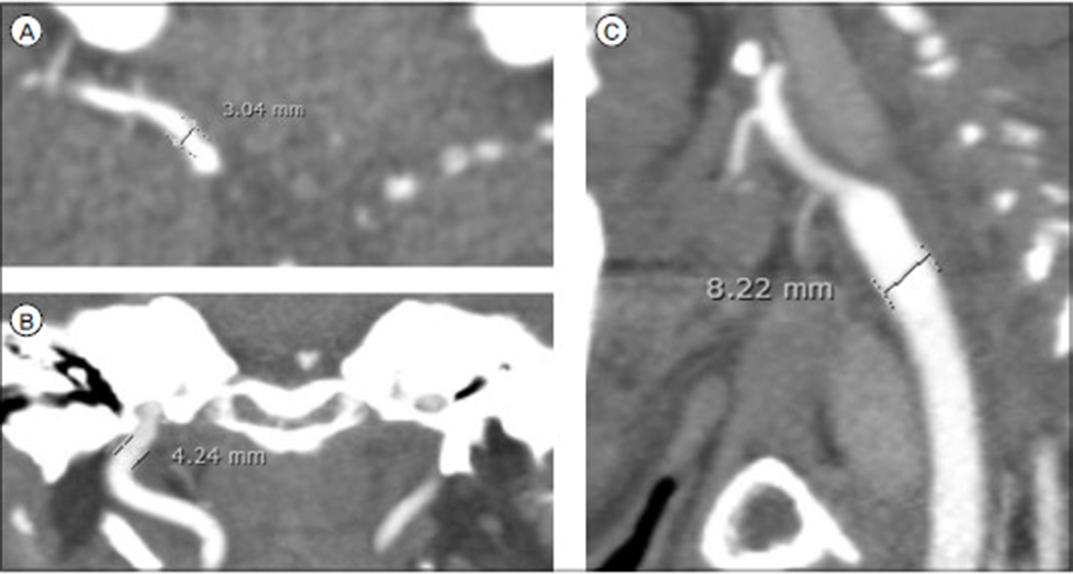
Fig. 2 To determine the use and sizes of thrombectomy devices, the initial CT angiogram was checked the normal diameters of contralateral MCA (A), ICA (B), and CCA (C), and we measured as 3.0mm, 4.2mm, and 8.2mm, respectively.
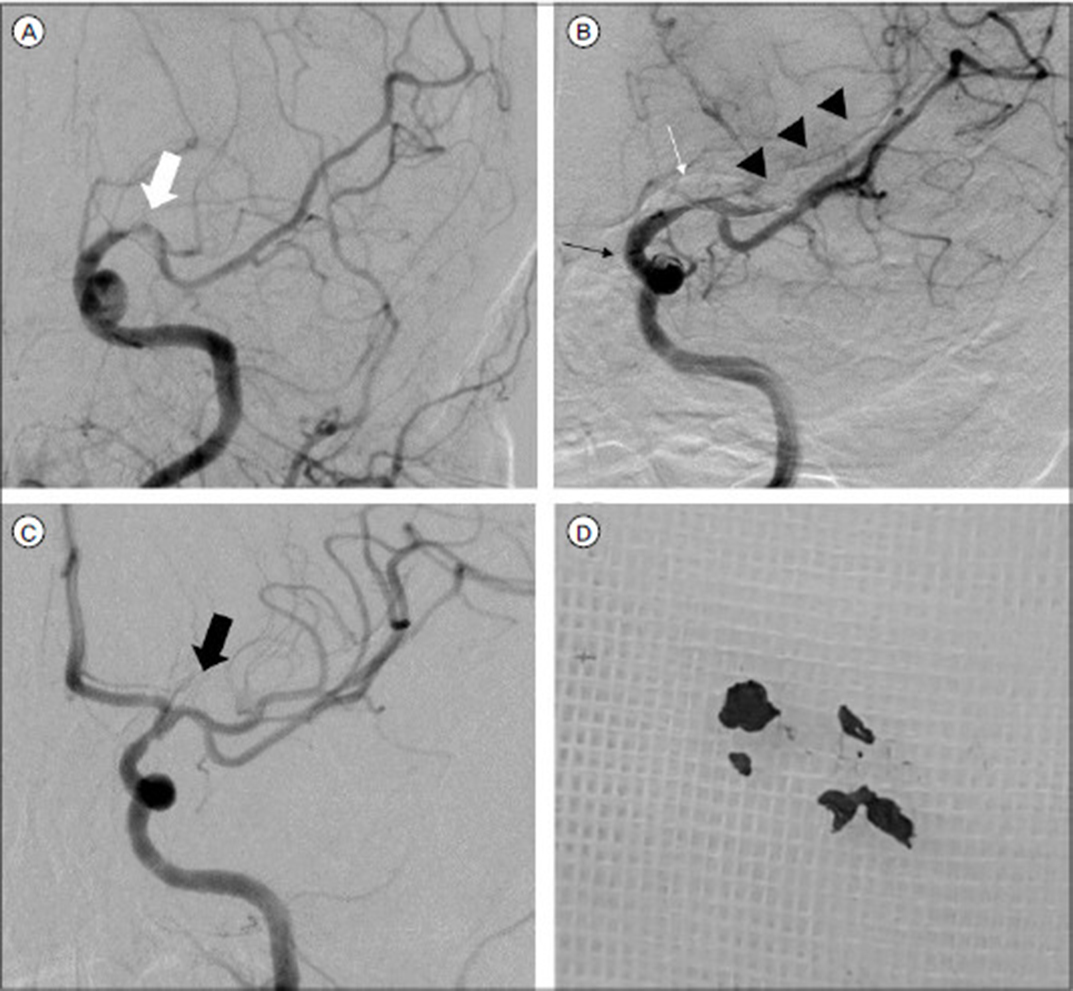
Fig. 3 (A) Diagnostic ICA angiogram showed anterotemporal artery flow but ACA and MCA flow was not detected because of thrombus (white arrow). (B) During waiting 3 min after deploying the Trevo XP 6 × 25 mm (white arrow) with AXS Catalyst ™6 (blackarrow) at the first trial, distal MCA flow was weakly observed, (arrow heads) but no ACA flow was detected due to thrombus in the stent. (C) After second thrombectomy trial, both ACA and MCA flow was completely reperfused with TICI 3. (black arrow) (D) Some thrombi were obtained from aspirating the AXS Catalyst ™6, but no clots were found in retriever stent and balloon guiding catheter.
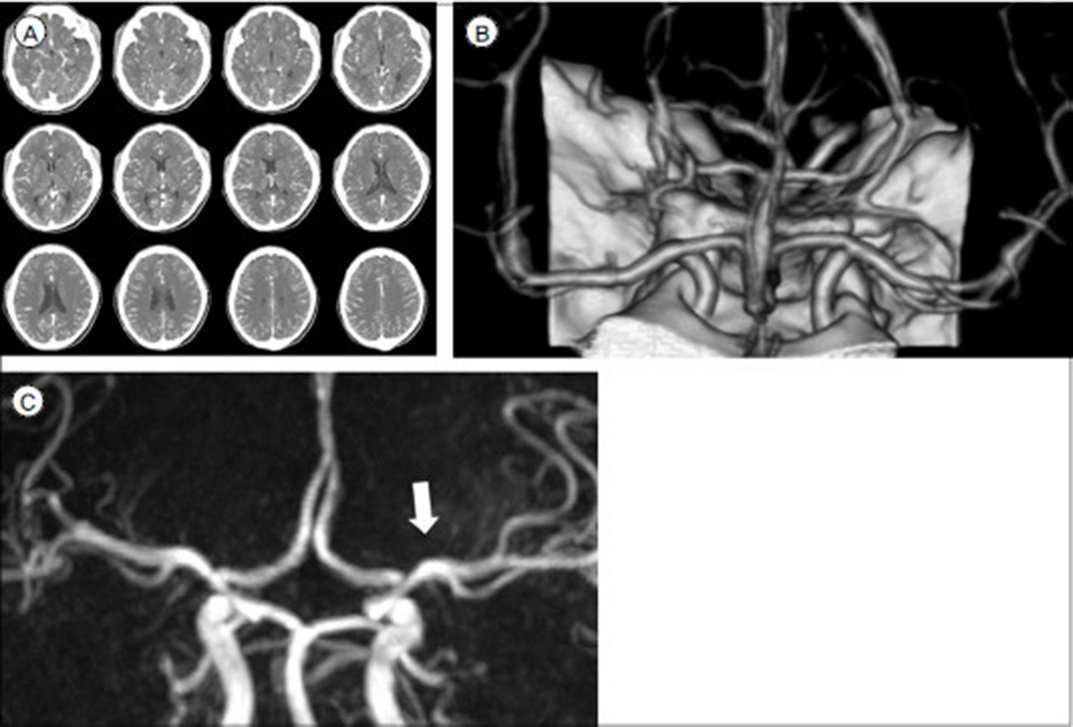
Fig. 4 After 3 days post procedure, there was no definite hemorrhage or low density in left MCA territory on enhanced brain CT (A) and the volume rendered reconstruction also showed intact left MCA (B). Three months later, follow-up MR angiography revealed well maintained completely reperfused MCA (white arrow) (C).
Reference
-
1. Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015; 01. 01. 372(1):11–20.2. Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015; 03. 12. 372(11):1009–1018.
Article3. Chueh JY, Puri AS, Wakhloo AK, Gounis MJ. Risk of distal embolization with stent retriever thrombectomy and ADAPT. J Neurointerv Surg. 2016; 02. 8(2):197–202.
Article4. Daugherty A. Achondroplasia: Etiology, Clinical Presentation, and Management. Neonatal Netw. 2017; 11. 01. 36(6):337–342.
Article5. Deshaies EM. Tri-axial system using the Solitaire-FR and Penumbra Aspiration Microcatheter for acute mechanical thrombectomy. J Clin Neurosci. 2013; 09. 20(9):1303–1305.
Article6. Dubiel L, Scott GA, Agaram R, McGrady E, Duncan A, Litchfield KN. Achondroplasia: anaesthetic challenges for caesarean section. Int J Obstet Anesth. 2014; 08. 23(3):274–278.
Article7. Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015; 03. 12. 372(11):1019–1030.8. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016; 04. 23. 387(10029):1723–1731.
Article9. Hecht JT, Francomano CA, Horton WA, Annegers JF. Mortality in achondroplasia. Am J Hum Genet. 1987; 09. 41(3):454–464.10. Hoover-Fong J, McGready J, Schulze K, Alade AY, Scott CI. A height-for-age growth reference for children with achondroplasia: Expanded applications and comparison with original reference data. Am J Med Genet A. 2017; 05. 173(5):1226–1230.11. Horton WA, Hall JG, Hecht JT. Achondroplasia. Lancet. 2007; 07. 14. 370(9582):162–172.
Article12. Horton WA, Rotter JI, Rimoin DL, Scott CI, Hall JG. Standard growth curves for achondroplasia. J Pediatr. 1978; 09. 93(3):435–438.
Article13. Jain KK. SOME OBSERVATIONS ON THE ANATOMY OF THE MIDDLE CEREBRAL ARTERY. Can J Surg. 1964; 04. 7:134–139.14. Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015; 06. 11. 372(24):2296–2306.
Article15. Kang DH, Park J. Endovascular Stroke Therapy Focused on Stent Retriever Thrombectomy and Direct Clot Aspiration: Historical Review and Modern Application. J Korean Neurosurg Soc. 2017; 05. 60(3):335–347.16. Krejza J, Arkuszewski M, Kasner SE, Weigele J, Ustymowicz A, Hurst RW, et al. Carotid artery diameter in men and women and the relation to body and neck size. Stroke. 2006; 04. 37(4):1103–1105.
Article17. Melekoglu R, Celik E, Eraslan S. Successful obstetric and anaesthetic management of a pregnant woman with achondroplasia. BMJ Case Rep. 2017; 10. 25. 2017:bcr2017221238.
Article18. Miyazaki M, Kanezaki S, Notani N, Ishihara T, Tsumura H. Spondylectomy and lateral lumbar interbody fusion for thoracolumbar kyphosis in an adult with achondroplasia: A case report. Medicine (Baltimore). 2017; 12. 96(49):e8983.19. Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015; 10. 46(10):3020–3035.
Article20. Rahman N, Nabi A, Gul I. Sheathless transradial coronary angioplasty in an achondroplasic patient with ST elevation myocardial infarction. BMJ Case Rep. 2015; 10. 27. 2015:bcr2015212697.
Article21. Rousseau F, Bonaventure J, Legeai-Mallet L, Pelet A, Rozet JM, Maroteaux P, et al. Mutations in the gene encoding fibroblast growth factor receptor-3 in achondroplasia. Nature. 1994; 09. 15. 371(6494):252–254.
Article22. Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015; 06. 11. 372(24):2285–2295.
Article23. Srinivas SK, Ramalingam R, Manjunath CN. A rare case of percutaneous coronary intervention in achondroplasia. J Invasive Cardiol. 2013; 06. 25(6):E136–E138.24. Susarla SM, Mundinger GS, Kapadia H, Fisher M, Smartt J, Derderian C, et al. Subcranial and orthognathic surgery for obstructive sleep apnea in achondroplasia. J Craniomaxillofac Surg. 2017; 12. 45(12):2028–2034.
Article25. Unger S, Bonafe L, Gouze E. Current Care and Investigational Therapies in Achondroplasia. Curr Osteoporos Rep. 2017; 04. 15(2):53–60.
Article26. Waller DK, Correa A, Vo TM, Wang Y, Hobbs C, Langlois PH, et al. The population-based prevalence of achondroplasia and thanatophoric dysplasia in selected regions of the US. Am J Med Genet A. 2008; 09. 15. 146a(18):2385–2389.
Article27. Wynn J, King TM, Gambello MJ, Waller DK, Hecht JT. Mortality in achondroplasia study: a 42-year follow-up. Am J Med Genet A. 2007; 11. 01. 143a(21):2502–2511.
Article28. Yi HJ, Sung JH, Lee DH, Hong JT, Lee SW. Single-Center Experience of Mechanical Thrombectomy with the Trevo XP ProVue 6 × 25 mm Stent Retriever in Middle Cerebral Artery Occlusion: Comparison with Trevo XP ProVue 4 × 20 mm. World Neurosurg. 2017; 11. 107:649–656.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effectiveness and Technical Considerations of Solitaire Platinum 4×40 mm Stent Retriever in Mechanical Thrombectomy with Solumbra Technique
- Effectiveness of Anchoring with Balloon Guide Catheter and Stent Retriever in Difficult Mechanical Thrombectomy for Large Vessel Occlusion
- Safe Implementation of Mechanical Thrombectomy in Acute Stroke Patients with Major Arterial Occlusion and Concomitant Subdural Hematoma
- Successful Mechanical Thrombectomy in a 2-Year-Old Male Through a 4-French Guide Catheter
- Mechanical Thrombectomy for Large Vessel Occlusion via the Transbrachial Approach: Case Series
