Effects of Different Modes of Upper Limb Training in Individuals With Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
- Affiliations
-
- 1Department of Physical Therapy, Faculty of Allied Health Sciences, Chulalongkorn University, Bangkok, Thailand. anong.ta@chula.ac.th
- 2Department of Preventive and Social Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
- 3Department of Physical Therapy, California State University, Northridge, CA, USA.
- KMID: 2463707
- DOI: http://doi.org/10.5535/arm.2019.43.5.592
Abstract
OBJECTIVE
To determine effects of different modes of upper limb training on dyspnea and quality of life of individuals with chronic obstructive pulmonary disease (COPD) having different disease severity.
METHODS
Randomized clinical trials were retrieved from five electronic databases. Risk of bias and quality of evidence were assessed using the Cochrane Collaboration's tool and the GRADE approach, respectively. Effects of upper limb training compared to control were identified using standardized mean difference and 95% confidence interval.
RESULTS
Fifteen studies with 514 subjects were included. When compared to control, upper limb endurance and strength training with moderate quality of evidence resulted in significant improvement in dyspnea. However, quality of life was not significantly different between upper limb training of all modes of and the control. The upper limb training was more effective in reducing dyspnea in patients with severe COPD than in those with mild to moderate levels of COPD. Although quality of life was slightly improved by upper limb training for those with moderate or severe level of COPD, such improvement did not reach a significant level when compared to the control.
CONCLUSION
Upper limb endurance and strength training could significantly improve dyspnea in individuals with chronic obstructive pulmonary disease. Thus, incorporating the upper limb training into pulmonary rehabilitation is recommended to reduce dyspnea, especially for those with severe patients. Further studies with larger sample size and standardized training protocol are needed to confirm these finding (Registration No. CRD42018102805).
Keyword
MeSH Terms
Figure
-
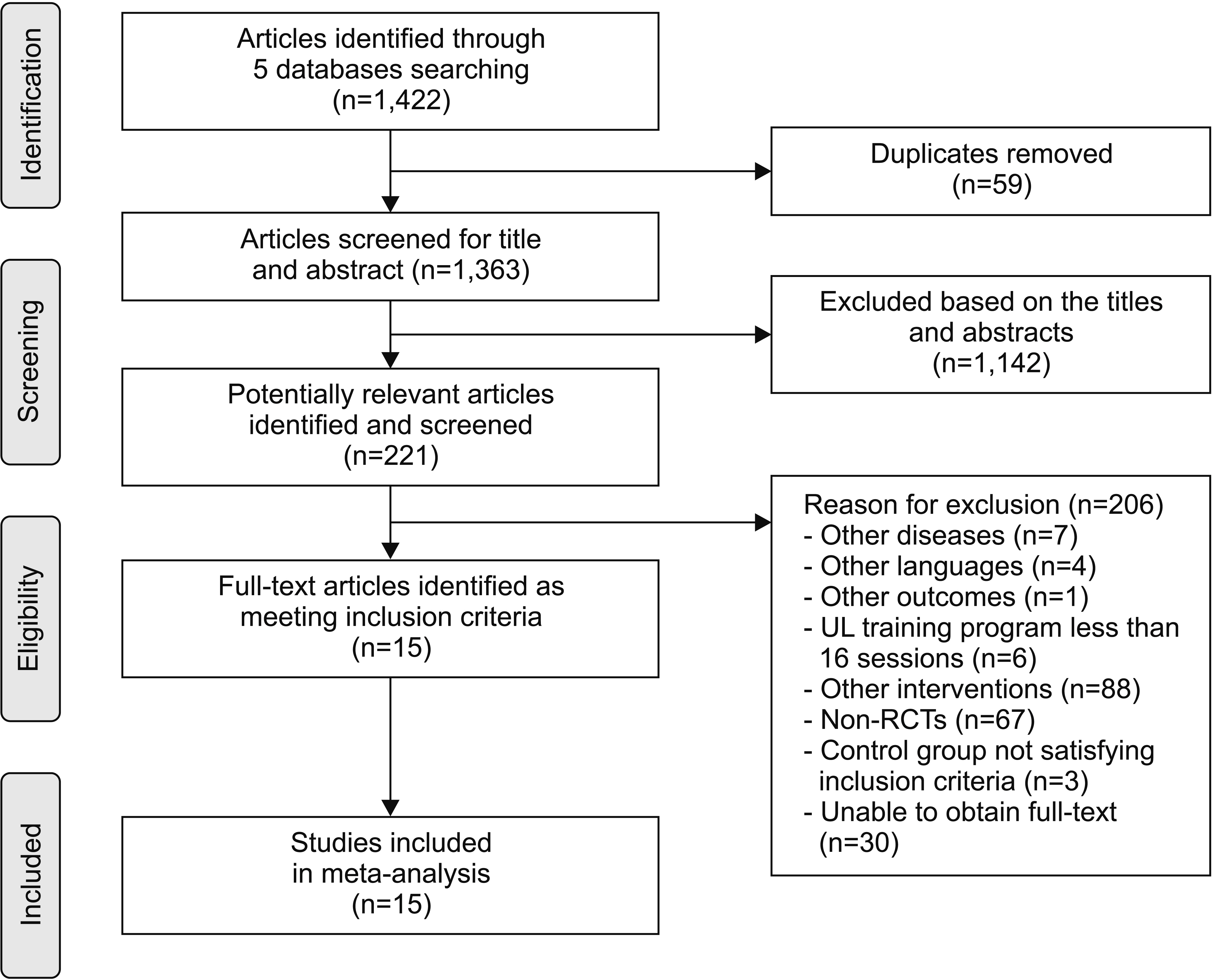
Fig. 1. Search strategy and flow diagram of article screening process.

Fig. 2. The risk of bias assessment of included studies by the Cochrane Collaboration’s tool.

Fig. 3. Forest plot showing difference in dyspnea by comparing modes of upper limb (UL) training with control condition (A) and by patient severity (B).
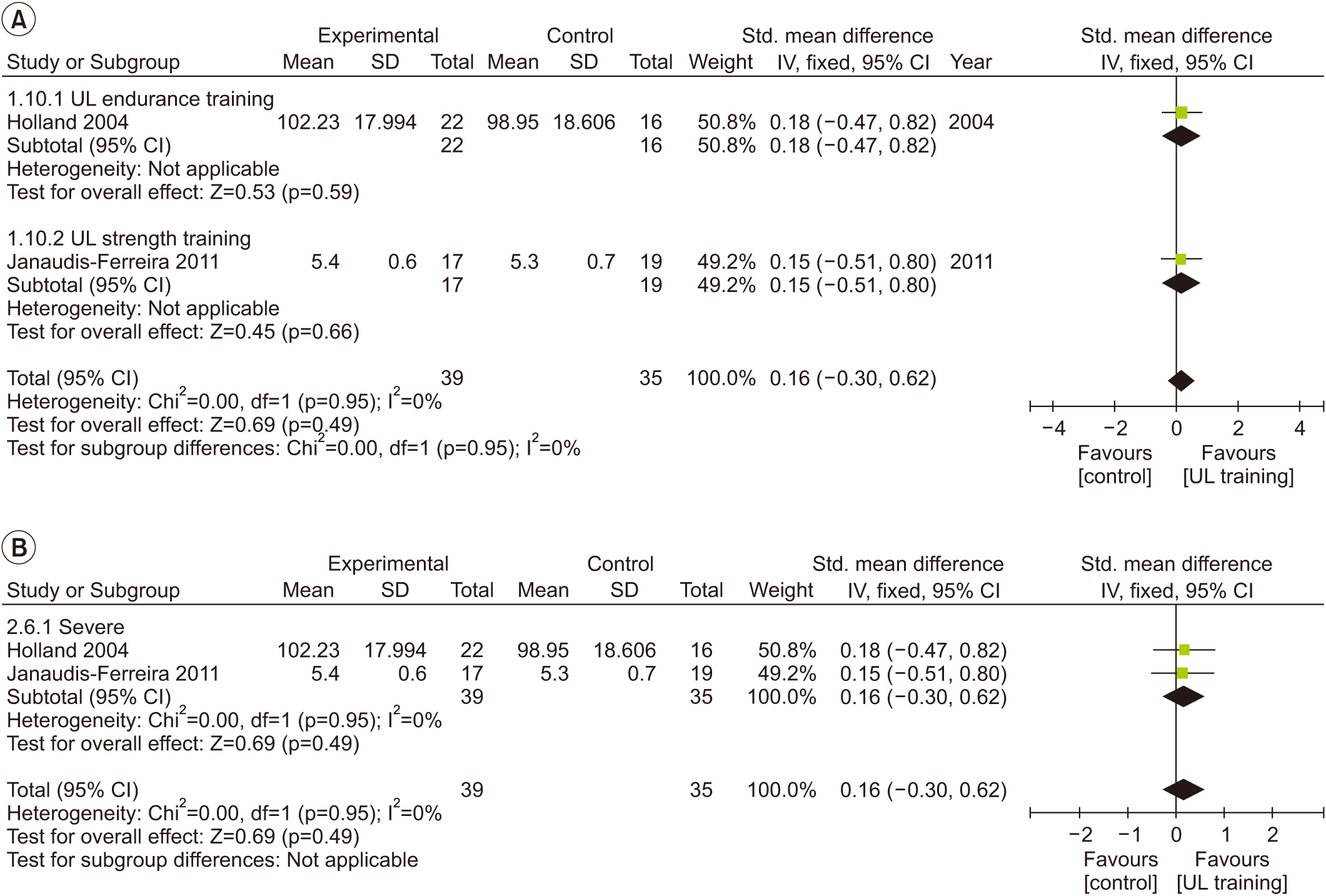
Fig. 4. Forest plot showing difference in quality of life from Chronic Respiratory Disease Questionnaire (CRQ) score by comparing modes of upper limb (UL) training with control condition (A) and by patient severity (B).
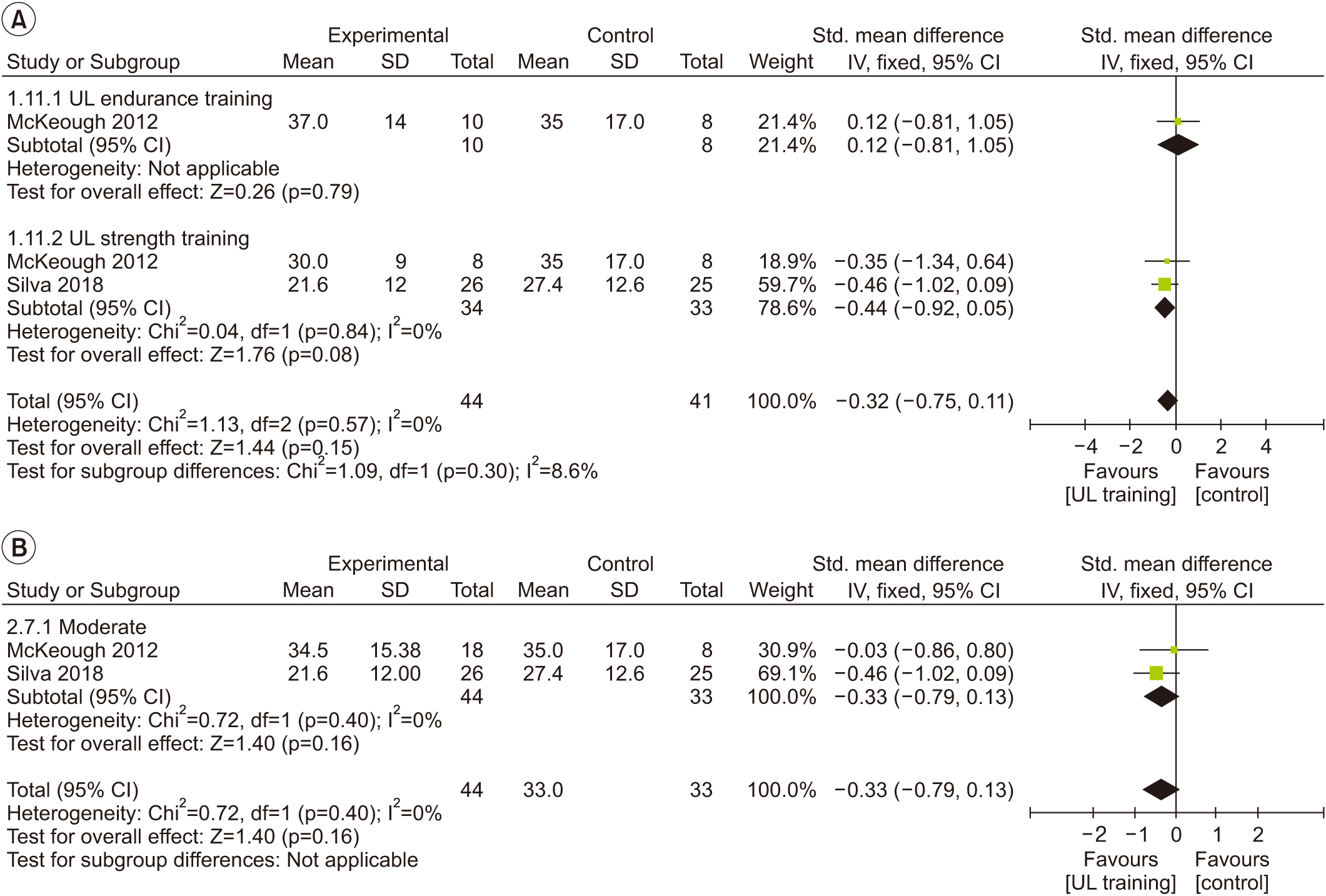
Fig. 5. Forest plot showing difference in quality of life from St. George’s Respiratory Questionnaire (SGRQ) by comparing modes of upper limb (UL) training with control condition (A) and by patient severity (B).
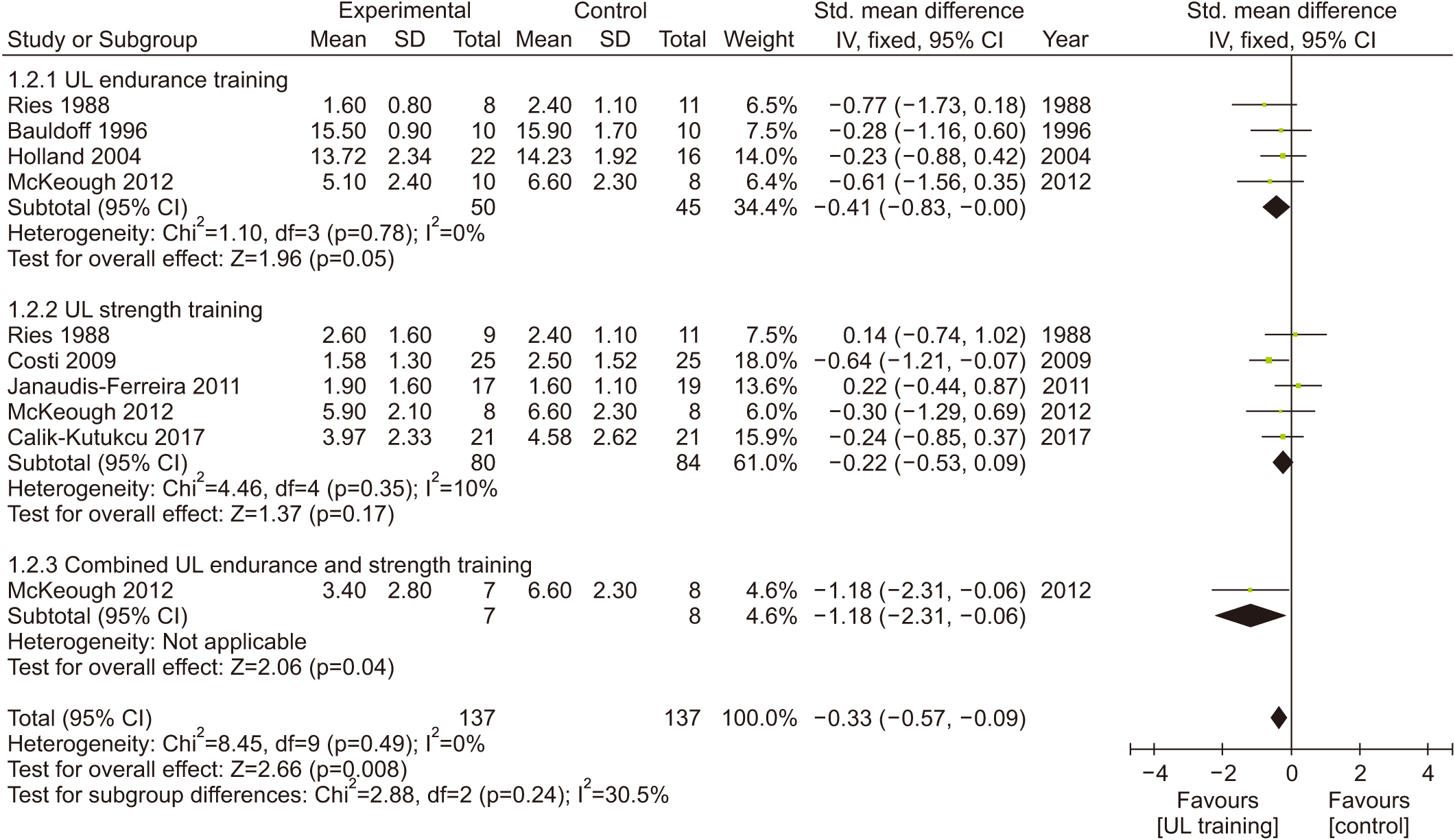
Fig. 6. Forest plot showing difference in upper limb (UL) fatigue by comparing modes of UL training with control condition.

Fig. 7. Forest plot showing difference in upper limb (UL) function by comparing modes of UL training with control condition.
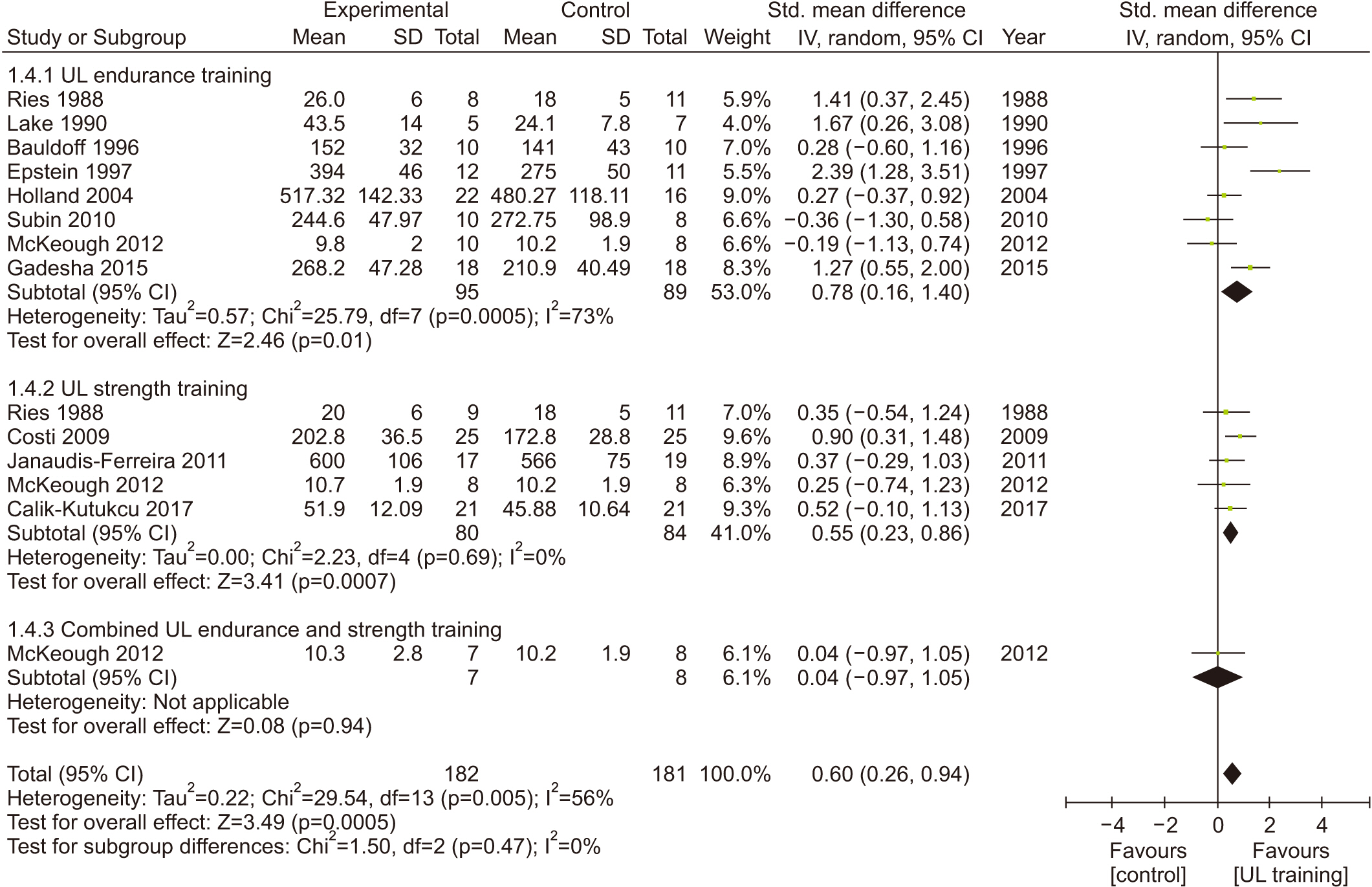
Fig. 8. Forest plot showing difference in upper limb (UL) exercise tolerance by comparing modes of UL training with control condition.
Reference
-
1. Wouters EF. Chronic obstructive pulmonary disease. 5: systemic effects of COPD. Thorax. 2002; 57:1067–70.2. Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005; 171:972–7.
Article3. Sclauser Pessoa IM, Parreira VF, Lorenzo VA, Reis MA, Costa D. Analysis of dynamic pulmonary hyperinflation (DH) following activities of daily living in patients with chronic obstructive pulmonary disease. Braz J Phys Ther. 2007; 11:469–74.4. Panagiotou M, Kastanakis E, Vogiatzis I. Exercise limitation in COPD. Pneumon. 2013; 26:245–56.5. Rabinovich RA, Vilaro J. Structural and functional changes of peripheral muscles in chronic obstructive pulmonary disease patients. Curr Opin Pulm Med. 2010; 16:123–33.
Article6. Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T, Mishima M. Exercise capacity deterioration in patients with COPD: longitudinal evaluation over 5 years. Chest. 2005; 128:62–9.7. Ries AL, Bauldoff GS, Carlin BW, Casaburi R, Emery CF, Mahler DA, et al. Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007; 131(5 Suppl):4S–42S.8. Langer D, Hendriks E, Burtin C, Probst V, van der Schans C, Paterson W, et al. A clinical practice guideline for physiotherapists treating patients with chronic obstructive pulmonary disease based on a systematic review of available evidence. Clin Rehabil. 2009; 23:445–62.
Article9. Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013; 188:e13–64.10. Costi S, Di Bari M, Pillastrini P, D’Amico R, Crisafulli E, Arletti C, et al. Short-term efficacy of upper-extremity exercise training in patients with chronic airway obstruction: a systematic review. Phys Ther. 2009; 89:443–55.
Article11. Janaudis-Ferreira T, Hill K, Goldstein R, Wadell K, Brooks D. Arm exercise training in patients with chronic obstructive pulmonary disease: a systematic review. J Cardiopulm Rehabil Prev. 2009; 29:277–83.12. Pan L, Guo YZ, Yan JH, Zhang WX, Sun J, Li BW. Does upper extremity exercise improve dyspnea in patients with COPD? A meta-analysis. Respir Med. 2012; 106:1517–25.
Article13. McKeough ZJ, Velloso M, Lima VP, Alison JA. Upper limb exercise training for COPD. Cochrane Database Syst Rev. 2016; 11:CD011434.
Article14. Breslin EH. Dyspnea-limited response in chronic obstructive pulmonary disease: reduced unsupported arm activities. Rehabil Nurs. 1992; 17:12–20.15. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009; 151:264–9.
Article16. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011; 343:d5928.
Article17. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008; 336:924–6.
Article18. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011; 64:401–6.
Article19. Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global Strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017; 195:557–82.
Article20. Cohen J. A power primer. Psychol Bull. 1992; 112:155–9.
Article21. Melsen WG, Bootsma MC, Rovers MM, Bonten MJ. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin Microbiol Infect. 2014; 20:123–9.
Article22. Ries AL, Ellis B, Hawkins RW. Upper extremity exercise training in chronic obstructive pulmonary disease. Chest. 1988; 93:688–92.
Article23. Lake FR, Henderson K, Briffa T, Openshaw J, Musk AW. Upper-limb and lower-limb exercise training in patients with chronic airflow obstruction. Chest. 1990; 97:1077–82.
Article24. Bauldoff GS, Hoffman LA, Sciurba F, Zullo TG. Homebased, upper-arm exercise training for patients with chronic obstructive pulmonary disease. Heart Lung. 1996; 25:288–94.
Article25. Holland AE, Hill CJ, Nehez E, Ntoumenopoulos G. Does unsupported upper limb exercise training improve symptoms and quality of life for patients with chronic obstructive pulmonary disease? J Cardiopulm Rehabil. 2004; 24:422–7.
Article26. Marrara KT, Marino DM, de Held PA, de Oliveira Junior AD, Jamami M, Di Lorenzo VA. Different physical therapy interventions on daily physical activities in chronic obstructive pulmonary disease. Respir Med. 2008; 102:505–11.
Article27. Costi S, Crisafulli E, Degli Antoni F, Beneventi C, Fabbri LM, Clini EM. Effects of unsupported upper extremity exercise training in patients with COPD: a randomized clinical trial. Chest. 2009; 136:387–95.28. Rao V, Prem V. Effect of upper limb, lower limb and combined training on health-related quality of life in COPD. Lung India. 2010; 27:4–7.
Article29. Janaudis-Ferreira T, Hill K, Goldstein RS, Robles-Ribeiro P, Beauchamp MK, et al. Resistance arm training in patients with COPD: a randomized controlled trial. Chest. 2011; 139:151–8.30. McKeough ZJ, Bye PT, Alison JA. Arm exercise training in chronic obstructive pulmonary disease: a randomised controlled trial. Chron Respir Dis. 2012; 9:153–62.31. Covey MK, McAuley E, Kapella MC, Collins EG, Alex CG, Berbaum ML, et al. Upper-body resistance training and self-efficacy enhancement in COPD. J Pulm Respir Med. 2012; Suppl 9:001.
Article32. Calik-Kutukcu E, Arikan H, Saglam M, Vardar-Yagli N, Oksuz C, Inal-Ince D, et al. Arm strength training improves activities of daily living and occupational performance in patients with COPD. Clin Respir J. 2017; 11:820–32.
Article33. Silva CMDSE, Gomes Neto M, Saquetto MB, Conceicao CSD, Souza-Machado A. Effects of upper limb resistance exercise on aerobic capacity, muscle strength, and quality of life in COPD patients: a randomized controlled trial. Clin Rehabil. 2018; 32:1636–44.
Article34. Epstein SK, Celli BR, Martinez FJ, Couser JI, Roa J, Pollock M, et al. Arm training reduces the VO2 and VE cost of unsupported arm exercise and elevation in chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 1997; 17:171–7.
Article35. Gadesha A, Bhise A. Effect of unsupported upper extremity exercise training on symptoms & quality of life in patients with COPD. Indian J Physiother Occup Ther. 2015; 9:146–51.36. Rekha K, Vijayalakshmi A, Samuel Sundar Doss D, Anandh V. Effects of home based upper extremity exercise in chronic obstructive pulmonary disease. Int J Pharmaceutial Clin Res. 2016; 8:1351–5.37. Bogdanis GC. Effects of physical activity and inactivity on muscle fatigue. Front Physiol. 2012; 3:142.
Article38. Fitts RH. Effects of regular exercise training on skeletal muscle contractile function. Am J Phys Med Rehabil. 2003; 82:320–31.
Article39. Maltais F, Simard AA, Simard C, Jobin J, Desgagnes P, LeBlanc P. Oxidative capacity of the skeletal muscle and lactic acid kinetics during exercise in normal subjects and in patients with COPD. Am J Respir Crit Care Med. 1996; 153:288–93.
Article40. Daabis R, Hassan M, Zidan M. Endurance and strength training in pulmonary rehabilitation for COPD patients. Egypt J Chest Dis Tuberc. 2017; 66:231–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of the Use of Beta-Blockers on Chronic Obstructive Pulmonary Disease Associated with Cardiovascular Comorbities: Systematic Review and Meta-analysis
- The Study on the Effects of a Respiratory Rehabilitation Program for COPD Patients
- Trends of Meta-analysis in Upper Gastrointestinal Diseases
- Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease
- The Effect of Respiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease: Preliminary Study
