Pearls and Tips in Shoulder Arthroplasty
- Affiliations
-
- 1Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA. sperling.john@mayo.edu
- KMID: 2462552
- DOI: http://doi.org/10.4055/cios.2019.11.3.258
Abstract
- There has been rapid evolution in new techniques and technology in shoulder arthroplasty. This has improved the efficiency of the procedures as well as expanded our ability to manage some of the most challenging cases. This article will review key aspects of patient evaluation, discuss key technical steps in primary anatomic and reverse arthroplasty, and lastly provide tips to facilitate revision surgery.
Keyword
MeSH Terms
Figure
-
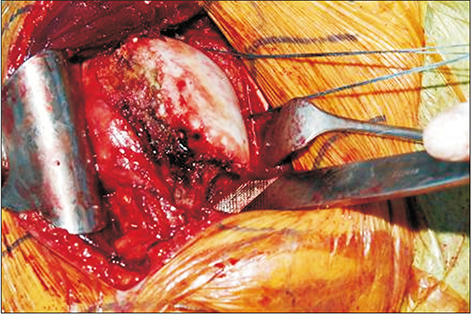
Fig. 1 Inferior capsular release along the anterior and inferior portion of the proximal humerus.
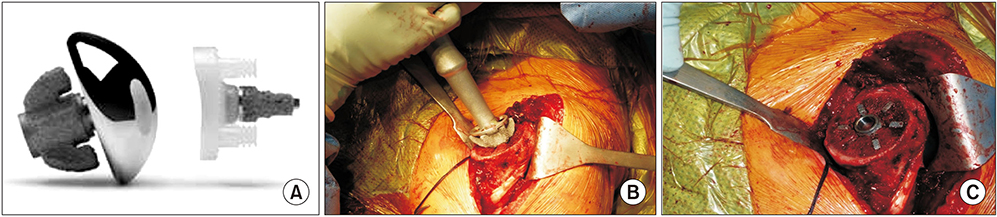
Fig. 2 Stemless shoulder replacement with porous ingrowth metal and a hybrid glenoid component. (A) Nano stemless implant. (B) Implanation of stemless humeral component. (C) Seating of the implant.
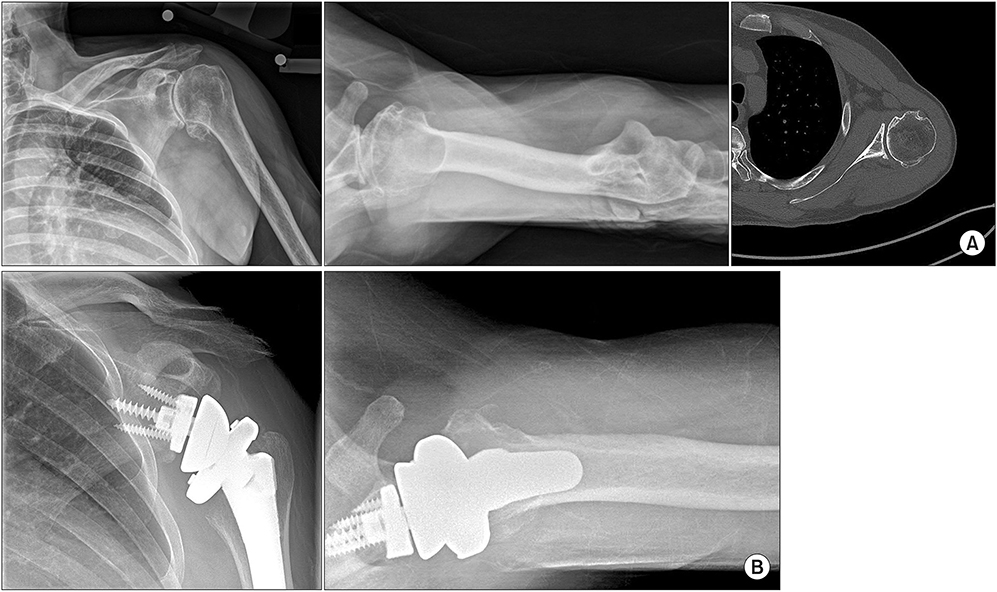
Fig. 3 (A) Significant posterior glenoid erosion. (B) An augmented baseplate is used posteriorly to help make up for the missing bone.

Fig. 4 (A) A router bit and a square tip impactor. (B) The router bit is used circumferentially around the proximal humerus. (C) The square tip impactor is then used against the collar of the implant.
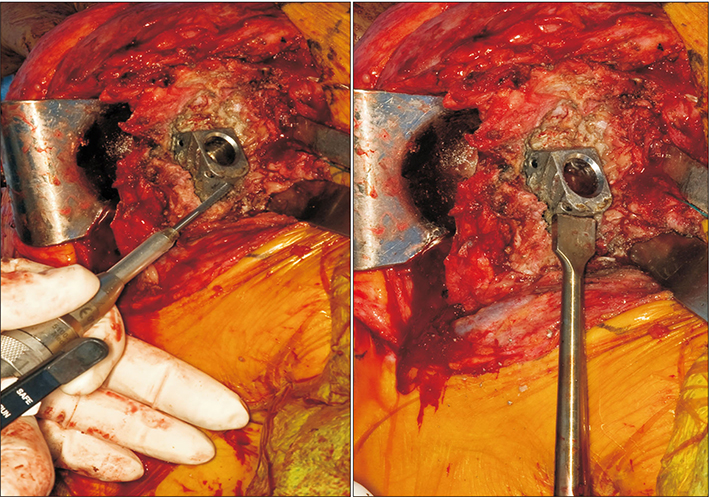
Fig. 5 Helicoidal bur is used to create a ledge in an implant without a collar. The square tip impactor is then used to remove the stem.

Fig. 6 (A) A hemiarthroplasty for fracture with tuberosity resorption and proximal humeral bone deficiency. (B) A metal implant is used to recreate tension on the deltoid.
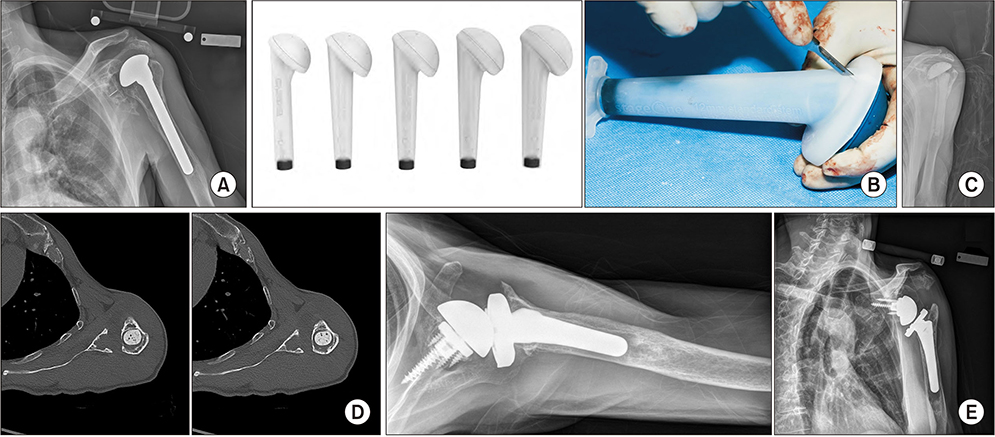
Fig. 7 (A) An infected shoulder arthroplasty with a loose humeral component that has shifted in position. (B) An antibiotic spacer can be templated ahead of the case. This facilitates the flow of surgery and allows the surgeon to titrate the antibiotics for the individual patient. (C) Radiograph with the cement spacer in place. (D) A computed tomography scan shows the bone remaining medially. This is ideally suited for central screw fixation. (E) A baseplate with a modular central screw engages the far cortex and provides compression. The glenoid baseplate is placed in the best bone and then the glenosphere is “dialed” for glenoid coverage. Additionally, a shorter humeral stem is used and the old pedestal is not bypassed.
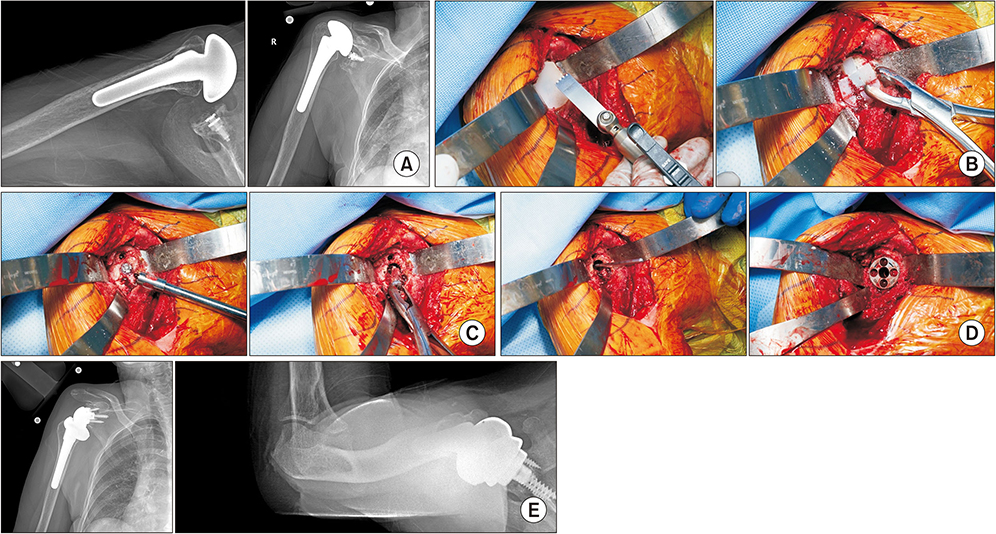
Fig. 8 (A) A patient who underwent repair of a large rotator cuff tear at the time of anatomic shoulder arthroplasty at an outside institution. She has a large rotator cuff tear, anterior subluxation of the humeral head, and the inability to raise her arm. (B) The glenoid component is split with a saw and removed with two horizontal cuts and two vertical cuts. (C) The central ingrowth post is removed. (D) An augmented baseplate is used to create tilt rather than reaming away a large amount of central and inferior bone. (E) Postoperative imaging revealing the convertible stem and augmented baseplate used to create the tilt.
Reference
-
1. Amini MH, Ricchetti ET, Iannotti JP. Three-dimensional templating and use of standard instrumentation in primary anatomic total shoulder arthroplasty. JBJS Essent Surg Tech. 2017; 7(3):e28.
Article2. Ricchetti ET, Jun BJ, Cain RA, et al. Sequential 3-dimensional computed tomography analysis of implant position following total shoulder arthroplasty. J Shoulder Elbow Surg. 2018; 27(6):983–992.
Article3. Iannotti JP, Weiner S, Rodriguez E, et al. Three-dimensional imaging and templating improve glenoid implant positioning. J Bone Joint Surg Am. 2015; 97(8):651–658.
Article4. Lapner PL, Wood KS, Zhang T, Athwal GS. The return of subscapularis strength after shoulder arthroplasty. J Shoulder Elbow Surg. 2015; 24(2):223–228.
Article5. Sacevich N, Athwal GS, Lapner P. Subscapularis management in total shoulder arthroplasty. J Hand Surg Am. 2015; 40(5):1009–1011.
Article6. Gutierrez S, Greiwe RM, Frankle MA, Siegal S, Lee WE 3rd. Biomechanical comparison of component position and hardware failure in the reverse shoulder prosthesis. J Shoulder Elbow Surg. 2007; 16:3 Suppl. S9–S12.7. Alentorn-Geli E, Clark NJ, Assenmacher AT, et al. What are the complications, survival, and outcomes after revision to reverse shoulder arthroplasty in patients older than 80 years? Clin Orthop Relat Res. 2017; 475(11):2744–2751.
Article8. Wagner ER, Statz JM, Houdek MT, Cofield RH, Sanchez-Sotelo J, Sperling JW. Use of a shorter humeral stem in revision reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2017; 26(8):1454–1461.
Article9. Wagner ER, Houdek MT, Hernandez NM, Cofield RH, Sanchez-Sotelo J, Sperling JW. Cement-within-cement technique in revision reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2017; 26(8):1448–1453.
Article10. Merolla G, Wagner E, Sperling JW, Paladini P, Fabbri E, Porcellini G. Revision of failed shoulder hemiarthroplasty to reverse total arthroplasty: analysis of 157 revision implants. J Shoulder Elbow Surg. 2018; 27(1):75–81.
Article11. Baghdadi YMK, Maradit-Kremers H, Dennison T, et al. The hospital cost of two-stage reimplantation for deep infection after shoulder arthroplasty. JSES Open Access. 2017; 1(1):15–18.
Article12. Assenmacher AT, Alentorn-Geli E, Dennison T, et al. Two-stage reimplantation for the treatment of deep infection after shoulder arthroplasty. J Shoulder Elbow Surg. 2017; 26(11):1978–1983.
Article13. Hernandez NM, Chalmers BP, Wagner ER, Sperling JW, Cofield RH, Sanchez-Sotelo J. Revision to reverse total shoulder arthroplasty restores stability for patients with unstable shoulder prostheses. Clin Orthop Relat Res. 2017; 475(11):2716–2722.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Musculocutaneous Nerve Palsy after the Reverse Total Shoulder Arthroplasty
- The Current State of Total Shoulder Arthroplasty
- Reverse Total Shoulder Arthroplasty: Techniques and Pitfalls
- Acromion Fracture after Reverse Total Shoulder Arthroplasty
- The Internal Rotation Deficit in Reverse Shoulder Arthroplasty: Can Humeral Rotation Make Difference?
