Massive cerebral venous sinus thrombosis secondary to Graves' disease
- Affiliations
-
- 1Department of Radiology, Keimyung University Dongsan Hospital, Daegu, Korea. shmm11111@gmail.com
- KMID: 2460199
- DOI: http://doi.org/10.12701/yujm.2019.00339
Abstract
- Cerebral venous sinus thrombosis (CVT) is a rare cerebrovascular condition accounting for 0.5-1% of all types of strokes in the general population. Hyperthyroidism is associated with procoagulant and antifibrinolytic activity, thereby precipitating a hypercoagulable state that predisposes to CVT. We report the case of a 31-year-old Korean man with massive CVT and diagnosis of concomitant Graves' disease at admission. Early diagnosis and prompt treatment of CVT are important to improve prognosis; therefore, CVT should be considered in the differential diagnosis in all patients with hyperthyroidism presenting with neurological symptoms.
MeSH Terms
Figure
-
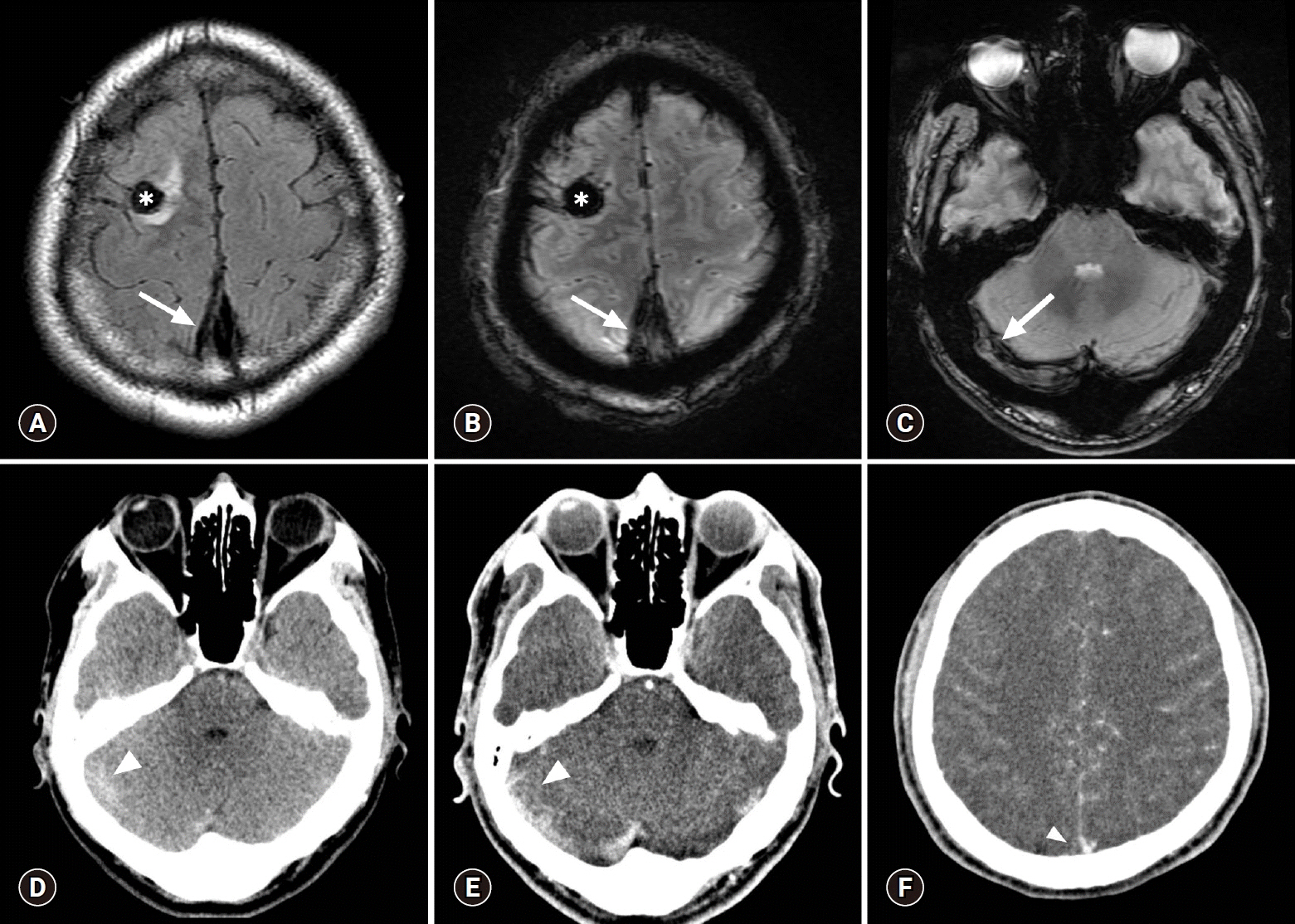
Fig. 1. Initial contrast-enhanced brain CT and MR scans. Focal hemorrhagic infarction is present in the right frontal lobe (asterisk) and a dark signal intensity representing a thrombus (blooming artifact) is present in the superior sagittal sinus (arrows) on the MR scan obtained the following day (A, FLAIR; B, T2* GRE sequences). A similar dark signal intensity representing a thrombus (arrow) is also present in the right transverse sinus (C, T2* GRE). These findings were neglected on the previous CT scan. The right transverse sinus shows a subtle hyperdensity (arrowhead) on a non-enhanced axial CT scan (D). Contrast-enhanced axial CT scans (E, F) show corresponding filling defect (arrowhead) at the same location and a partial empty delta sign (arrowhead) in the superior sagittal sinus, which were missed during evaluation of the initial brain CT scan. CT, computed tomography; MR, magnetic resonance; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo.
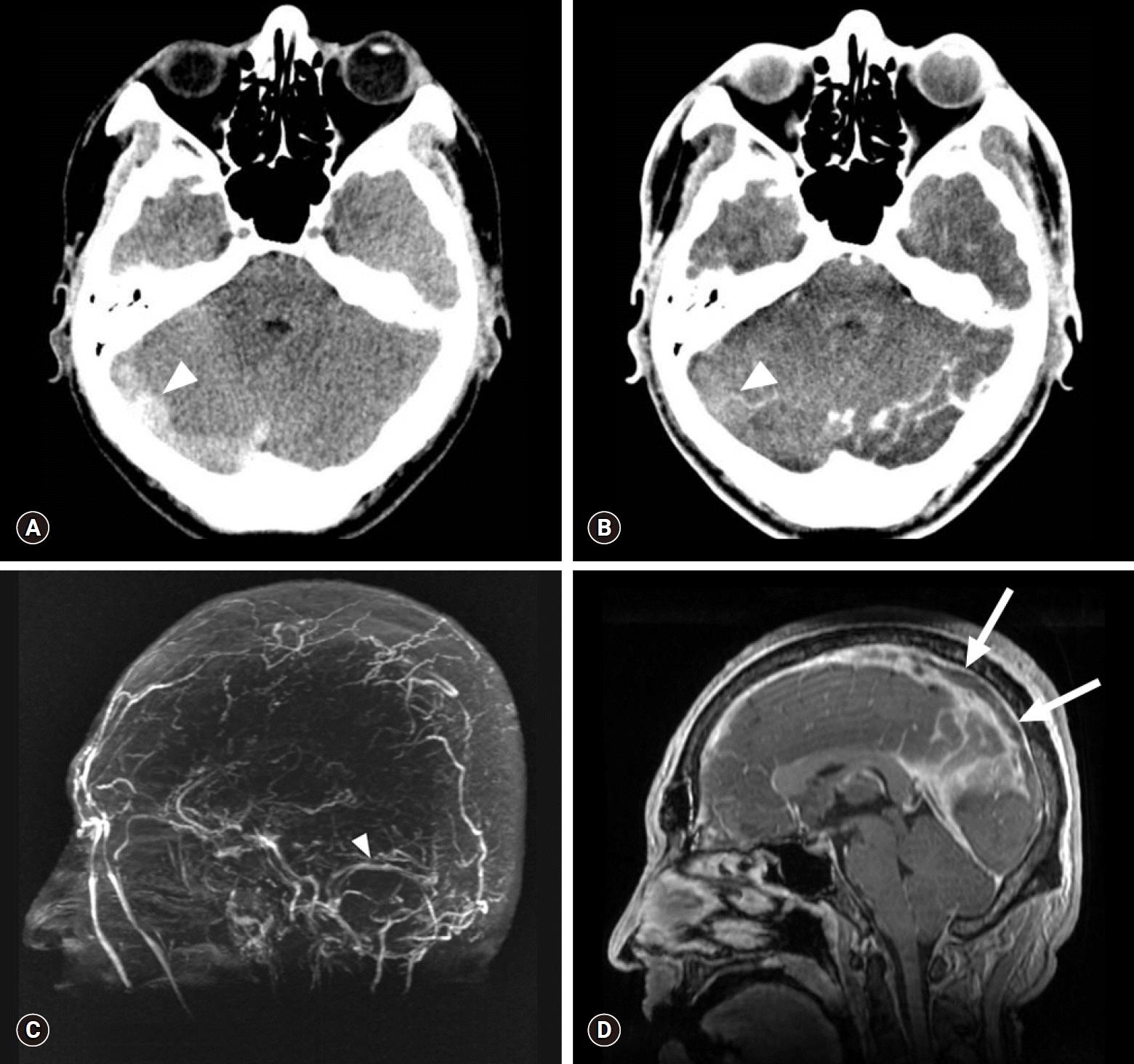
Fig. 2. Brain CT and MR venography scans obtained on admission (3 days after the initial brain CT). Axial non-enhanced CT scan (A) shows a more prominent hyperdensity (HU 70) in the right transverse sinus (arrowhead), which shows the same density (HU 70) on contrast-enhanced brain CT scan (B). Absence of flow-related enhancement is present in the superior sagittal and right transverse to sigmoid sinuses, as opposed to normal flow-related enhancement observed in the left transverse sinus (arrowhead) on an MIP image (C). Sagittal reconstructed MR venography scan (D) shows the propagation of the filling defect along the superior sagittal sinus (arrows). CT, computed tomography; MR, magnetic resonance; HU, Hounsfield units; MIP, maximum intensity projection.
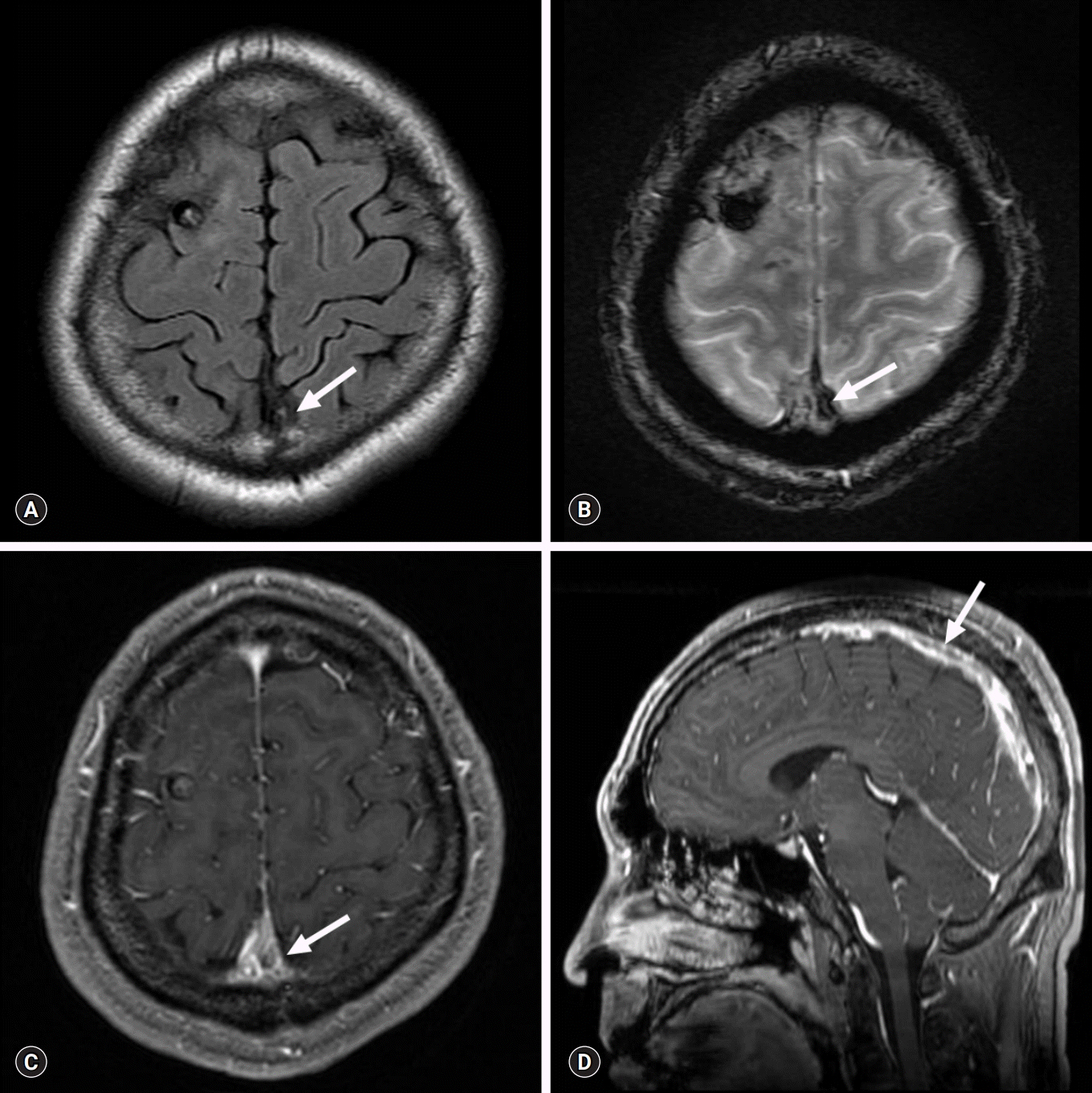
Fig. 3. Conventional and sagittal reformatted MR venography scans obtained at 1-month follow-up. Reduced thrombus burden in the superior sagittal sinus (arrows) is present on axial FLAIR sequence (A), T2* GRE sequence (B), contrast-enhanced T1WI (C), and sagittal reformatted MR venography scan (D). MR, magnetic resonance; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo; T1WI, T1-weighted image.
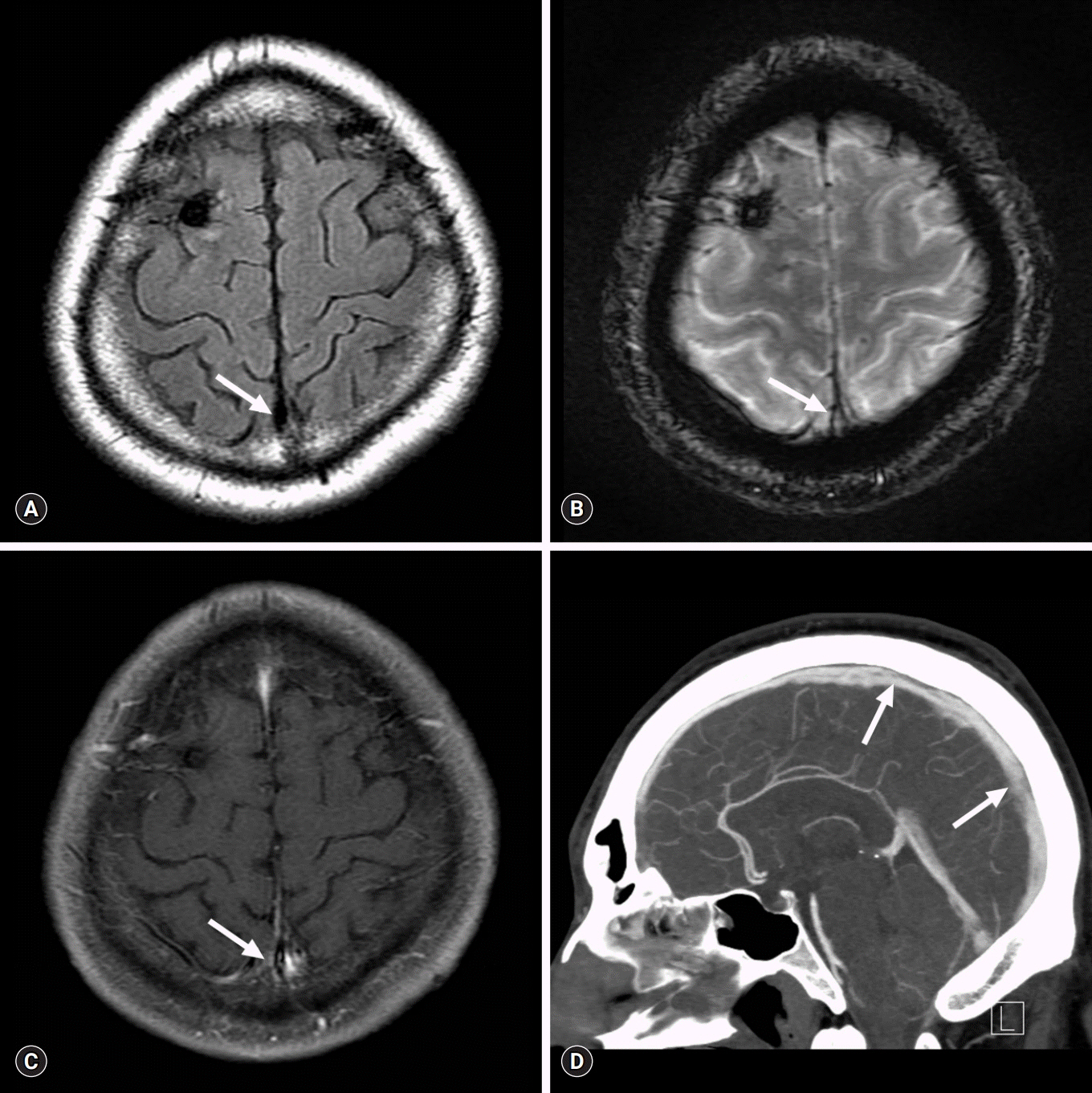
Fig. 4. Conventional MR and delayed-phase CT angiography scans obtained at the last follow-up showing near-complete recanalization of the cerebral venous sinuses. Conventional MR venography scan (A, FLAIR; B, T2* GRE; and C, contrast-enhanced T1WI) and delayed-phase CT angiography scan (D) obtained at 1-year follow-up shows near-complete recanalization of the superior sagittal and the right transverse and sigmoid sinuses (arrows). MR, magnetic resonance; CT, computed tomography; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo; T1WI, T1-weighted image.
Reference
-
References
1. Einhäupl K, Bousser MG, de Bruijn SF, Ferro JM, Martinelli I, Masuhr F, et al. EFNS guideline on the treatment of cerebral venous and sinus thrombosis. Eur J Neurol. 2006; 13:553–9.
Article2. Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011; 42:1158–92.
Article3. Kaliebe H. Autochthone sinusthrombose bei einem falle von morbus basedow und tabes. Med Klin. 1913; 9:1929–32.4. Doyle JB. Obstruction of the longitudinal sinus. Arch Neurol Psychiatry. 1927; 18:374–82.
Article5. Hermans E, Mariën P, De Deyn PP. Sinus sigmoideus thrombosis secondary to graves' disease: a case description. Case Rep Neurol. 2011; 3:203–9.
Article6. Hwang JU, Kwon KY, Hur JW, Lee JW, Lee HK. The role of hyperthyroidism as the predisposing factor for superior sagittal sinus thrombosis. J Cerebrovasc Endovasc Neurosurg. 2012; 14:251–4.
Article7. Merino M, Guijarro MG, Iglesias P, Aladro Y, Montero P. Thyrotoxicosis and cerebral venous sinus thrombosis, causality or chance alone? Endocrinol Nutr. 2012; 59:462–3.
Article8. Migeot M, Rutgers MP, Gille M. Puerperal cerebral sinus venous thrombosis and acute hyperthyroidism in Graves' disease. Acta Neurol Belg. 2013; 113:331–3.
Article9. Bensalah M, Squizzato A, Ould Kablia S, Menia H, Kemali Z. Cerebral vein and sinus thrombosis and hyperthyrodism: a case report and a systematic review of the literature. Thromb Res. 2011; 128:98–100.
Article10. Squizzato A, Romualdi E, Büller HR, Gerdes VE. Thyroid dysfunction and effects on coagulation and fibrinolysis: a systematic review. J Clin Endocrinol Metab. 2007; 92:2415–20.
Article11. Rosendaal FR. Venous thrombosis: a multicausal disease. Lancet. 1999; 353:1167–73.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Leptomeningeal Metastasis Associated with Cerebral Venous Thrombosis
- A Case of Cerebral Venous Thrombosis in a Patient with Graves' Disease
- Neuro-Behcet's Disease Presented with Cerebral Venous Sinus Thrombosis: A Case Report
- Cerebral Venous Sinus Thrombosis Associated with Antithrombin III Deficiency: A Case Report
- Development of Subdural Hemorrhage in a Patient With Cerebral Venous Sinus Thrombosis
