J Gynecol Oncol.
2019 Nov;30(6):e95. 10.3802/jgo.2019.30.e95.
Accuracy of frozen section diagnosis and factors associated with final pathological diagnosis upgrade of mucinous ovarian tumors
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. catgut1-0@hanmail.net
- 2Department of Obstetrics and Gynecology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 3Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2458900
- DOI: http://doi.org/10.3802/jgo.2019.30.e95
Abstract
OBJECTIVE
To determine the accuracy of frozen section diagnosis and factors associated with final pathological diagnosis upgrade in patients with mucinous ovarian tumors.
METHODS
This study included 1,032 patients with mucinous ovarian tumors who underwent frozen section diagnosis during surgery. Sensitivity, specificity, and diagnostic accuracy of frozen section diagnosis was calculated. Univariate and multivariate regression analyses were performed to determine factors associated with diagnosis upgrade in the final pathology report.
RESULTS
The sensitivity and specificity of frozen section diagnosis were 99.1% (95% confidence interval [CI]=98%-99.6%) and 82.2% (95% CI=77.9%-85.7%), respectively, for benign mucinous tumors; 74.6% (95% CI=69.1%-79.4%) and 96.7% (95% CI=95.2%-97.8%), respectively, for mucinous borderline ovarian tumors; and 72.5% (95% CI=62.9%-80.3%) and 98.8% (95% CI=97.9%-99.3%), respectively, for invasive mucinous carcinomas. The multivariate analysis revealed that mixed tumor histology (odds ratio [OR]=2.8; 95% CI=1.3-6.3; p=0.012), tumor size >12 cm (OR=2.5; 95% CI=1.5-4.3; p=0.001), multilocular tumor (OR=2.9; 95% CI=1.4-6.0; p=0.006), and presence of a solid component in the tumor (OR=3.1; 95% CI=1.8-5.1; p<0.001) were independent risk factors for final pathological diagnosis upgrade.
CONCLUSIONS
Mixed tumor histology, tumor size >12 cm, multilocular tumor, and presence of a solid component in the tumor were independent risk factors for final pathological diagnosis upgrade based on frozen section diagnosis.
Keyword
MeSH Terms
Figure
-
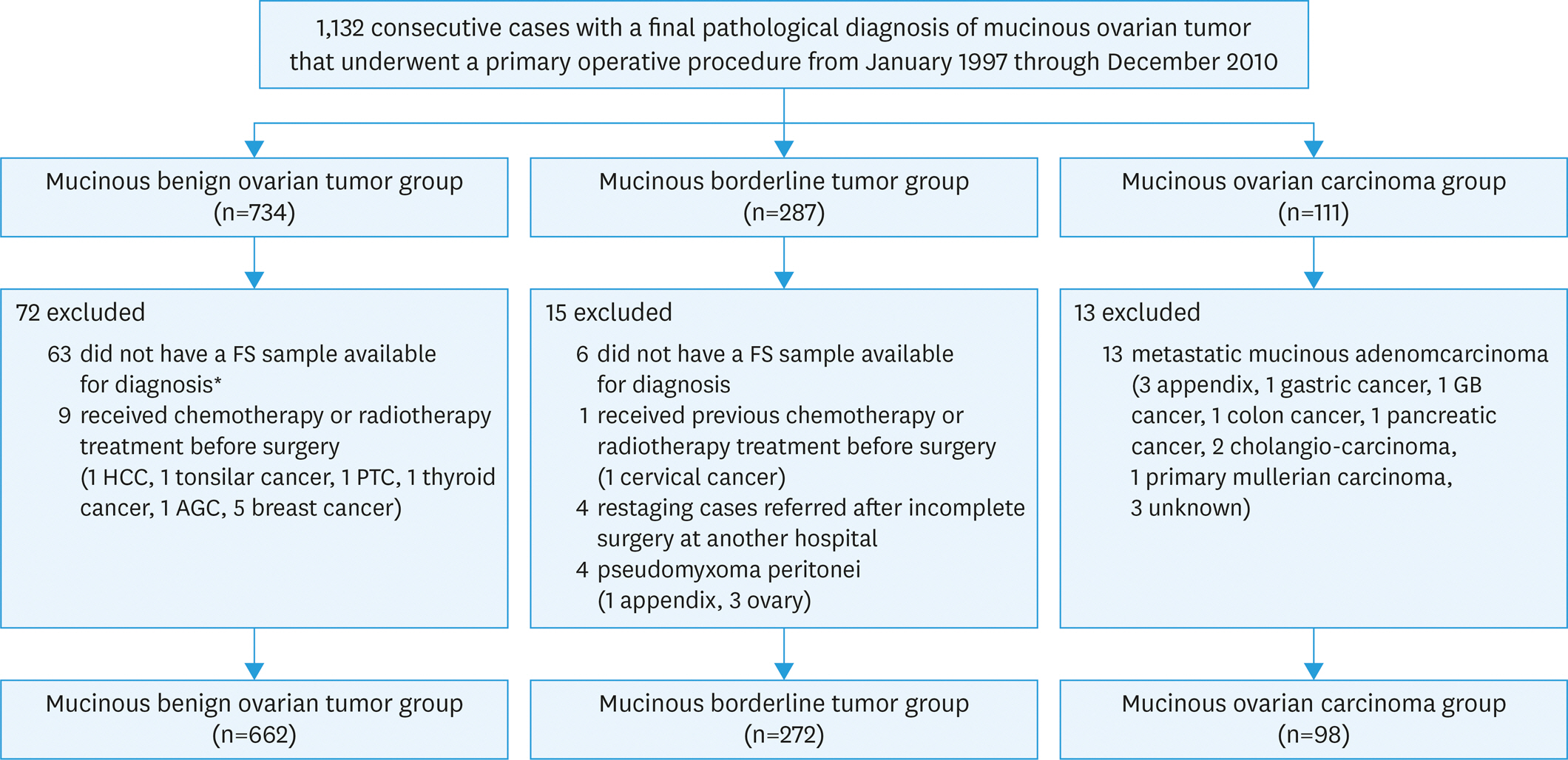
Fig. 1. Study flow chart. AGC, advanced gastric cancer; GB, gallbladder; HCC, hepatocelluar carcinoma; PTC, parathyroid cancer. * Samples were not available for frozen section diagnosis; these cases included 52 patients with unilateral and two patients with bilateral mucinous benign ovarian tumors. In addition, nine patients with bilateral benign mucinous tumors had frozen sections available for only one ovarian tumor.
Reference
-
References
1. Jayson GC, Kohn EC, Kitchener HC, Ledermann JA. Ovarian cancer. Lancet. 2014; 384:1376–88.
Article2. Hata K, Hata T, Manabe A, Kitao M. Ovarian tumors of low malignant potential: transvaginal Doppler ultrasound features. Gynecol Oncol. 1992; 45:259–64.
Article3. Gotlieb WH, Soriano D, Achiron R, Zalel Y, Davidson B, Kopolovic J, et al. CA 125 measurement and ultrasonography in borderline tumors of the ovary. Am J Obstet Gynecol. 2000; 183:541–6.
Article4. Ratnavelu ND, Brown AP, Mallett S, Scholten RJ, Patel A, Founta C, et al. Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses. Cochrane Database Syst Rev. 2016; 3:CD010360.
Article5. Twaalfhoven FC, Peters AA, Trimbos JB, Hermans J, Fleuren GJ. The accuracy of frozen section diagnosis of ovarian tumors. Gynecol Oncol. 1991; 41:189–92.
Article6. Rose PG, Rubin RB, Nelson BE, Hunter RE, Reale FR. Accuracy of frozen-section (intraoperative consultation) diagnosis of ovarian tumors. Am J Obstet Gynecol. 1994; 171:823–6.
Article7. Pinto PB, Andrade LA, Derchain SF. Accuracy of intraoperative frozen section diagnosis of ovarian tumors. Gynecol Oncol. 2001; 81:230–2.
Article8. Gol M, Baloglu A, Yigit S, Dogan M, Aydin C, Yensel U. Accuracy of frozen section diagnosis in ovarian tumors: is there a change in the course of time? Int J Gynecol Cancer. 2003; 13:593–7.
Article9. Ilvan S, Ramazanoglu R, Ulker Akyildiz E, Calay Z, Bese T, Oruc N. The accuracy of frozen section (intraoperative consultation) in the diagnosis of ovarian masses. Gynecol Oncol. 2005; 97:395–9.
Article10. Taskiran C, Erdem O, Onan A, Bozkurt N, Yaman-Tunc S, Ataoglu O, et al. The role of frozen section evaluation in the diagnosis of adnexal mass. Int J Gynecol Cancer. 2008; 18:235–40.
Article11. Rakhshan A, Zham H, Kazempour M. Accuracy of frozen section diagnosis in ovarian masses: experience at a tertiary oncology center. Arch Gynecol Obstet. 2009; 280:223–8.
Article12. Stewart CJ, Brennan BA, Hammond IG, Leung YC, McCartney AJ. Intraoperative assessment of ovarian tumors: a 5-year review with assessment of discrepant diagnostic cases. Int J Gynecol Pathol. 2006; 25:216–22.13. Brun JL, Cortez A, Rouzier R, et al. Factors influencing the use and accuracy of frozen section diagnosis of epithelial ovarian tumors. Am J Obstet Gynecol. 2008; 199:244. e1–7.
Article14. Puls L, Heidtman E, Hunter JE, Crane M, Stafford J. The accuracy of frozen section by tumor weight for ovarian epithelial neoplasms. Gynecol Oncol. 1997; 67:16–9.
Article15. Tangjitgamol S, Jesadapatrakul S, Manusirivithaya S, Sheanakul C. Accuracy of frozen section in diagnosis of ovarian mass. Int J Gynecol Cancer. 2004; 14:212–9.
Article16. FIGO (International Federation of Gynecology and Obstetrics) annual report on the results of treatment in gynecological cancer. Int J Gynaecol Obstet. 2003; 83(Suppl 1):ix–xxii. 1–229.17. Meinhold-Heerlein I, Fotopoulou C, Harter P, Kurzeder C, Mustea A, Wimberger P, et al. The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications. Arch Gynecol Obstet. 2016; 293:695–700.
Article18. Fauvet R, Boccara J, Dufournet C, Poncelet C, Daraï E. Laparoscopic management of borderline ovarian tumors: results of a French multicenter study. Ann Oncol. 2005; 16:403–10.
Article19. Ronnett BM, Kajdacsy-Balla A, Gilks CB, Merino MJ, Silva E, Werness BA, et al. Mucinous borderline ovarian tumors: points of general agreement and persistent controversies regarding nomenclature, diagnostic criteria, and behavior. Hum Pathol. 2004; 35:949–60.
Article20. Storms AA, Sukumvanich P, Monaco SE, Beriwal S, Krivak TC, Olawaiye AB, et al. Mucinous tumors of the ovary: diagnostic challenges at frozen section and clinical implications. Gynecol Oncol. 2012; 125:75–9.
Article21. Pongsuvareeyakul T, Khunamornpong S, Settakorn J, Sukpan K, Suprasert P, Siriaunkgul S. Accuracy of frozen-section diagnosis of ovarian mucinous tumors. Int J Gynecol Cancer. 2012; 22:400–6.
Article22. Bige O, Demir A, Saygili U, Gode F, Uslu T, Koyuncuoglu M. Frozen section diagnoses of 578 ovarian tumors made by pathologists with and without expertise on gynecologic pathology. Gynecol Oncol. 2011; 123:43–6.
Article23. Lehner R, Wenzl R, Heinzl H, Husslein P, Sevelda P. Influence of delayed staging laparotomy after laparoscopic removal of ovarian masses later found malignant. Obstet Gynecol. 1998; 92:967–71.
Article24. Houck K, Nikrui N, Duska L, Chang Y, Fuller AF, Bell D, et al. Borderline tumors of the ovary: correlation of frozen and permanent histopathologic diagnosis. Obstet Gynecol. 2000; 95:839–43.
Article25. Kim JH, Kim TJ, Park YG, Lee SH, Lee CW, Song MJ, et al. Clinical analysis of intraoperative frozen section proven borderline tumors of the ovary. J Gynecol Oncol. 2009; 20:176–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Accuracy of Frozen Section in the Diagnosis of Ovarian Tumors
- The accuracy of frozen section in the diagnosis of ovarian tumors
- The Accuracy of Frozen section Diagnosis of ovarian Tumors
- Accuracy of frozen section diagnosis for ovarian tumors according to histologic type and malignant potential
- The Accuracy of Frozen Section Diagnosis of Gynecologic Tumors
