CT-Guided Radiofrequency Ablation of T1a Renal Cell Carcinoma in Korea: Mid-Term Outcomes
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea. rapark@skku.edu
- KMID: 2458069
- DOI: http://doi.org/10.3348/kjr.2016.17.5.763
Abstract
OBJECTIVE
To evaluate the mid-term outcomes of percutaneous radiofrequency ablation (RFA) treatment in patients with small (< 4 cm) renal cell carcinoma (RCC) in Korea.
MATERIALS AND METHODS
Between 2010 and 2015, 51 patients (40 men and 11 women; median age, 57 years) with biopsyproven 51 RCC were treated using CT-guided RFA. All patients were clinically staged T1aN0M0 prior to RFA. The median tumor size and follow-up period were 2.1 cm (range, 1.0-3.9 cm) and 26 months (4-60 months), respectively. Local tumor progression, distant metastasis, primary and secondary effectiveness rates, and major complication rates were recorded. Estimated glomerular filtration rates (GFRs) between pre-RFA and last follow-up were compared using paired t tests. The 2-year recurrence-free survival rate was calculated using Kaplan-Meier survival analysis.
RESULTS
Of the 51 patients, 2 (3.9%) experienced local tumor progression, and 1 (2.0%) had lymph node metastasis after the first RFA session. Primary and secondary effectiveness rates were 96.1% (49/51) and 100% (1/1), respectively. Only 1 patient experienced a major complication (uretero-pelvic stricture) after the second RFA session for treating a local tumor progression, and the major complication rate was 1.9% (1/52). The median pre-RFA and last follow-up GFRs were 87.1 mL/ min/1.73 m2 (14.2-142.7 mL/min/1.73 m2) and 72.0 mL/min/1.73 m2 (7.2-112.6 mL/min/1.73 m2), respectively (p < 0.0001). The 2-year recurrence-free survival rate was 96.0%.
CONCLUSION
CT-guided RFA is a safe and effective treatment in Korean patients with T1a RCC because of excellent mid-term outcomes.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Carcinoma, Renal Cell/diagnostic imaging/pathology/*surgery
Catheter Ablation/adverse effects/*methods
Female
Glomerular Filtration Rate
Humans
Kaplan-Meier Estimate
Kidney Neoplasms/diagnostic imaging/pathology/*surgery
Male
Middle Aged
Radiography, Interventional/methods
Retrospective Studies
Time Factors
Tomography, X-Ray Computed/methods
Treatment Outcome
Ureteral Obstruction/etiology
Figure
-
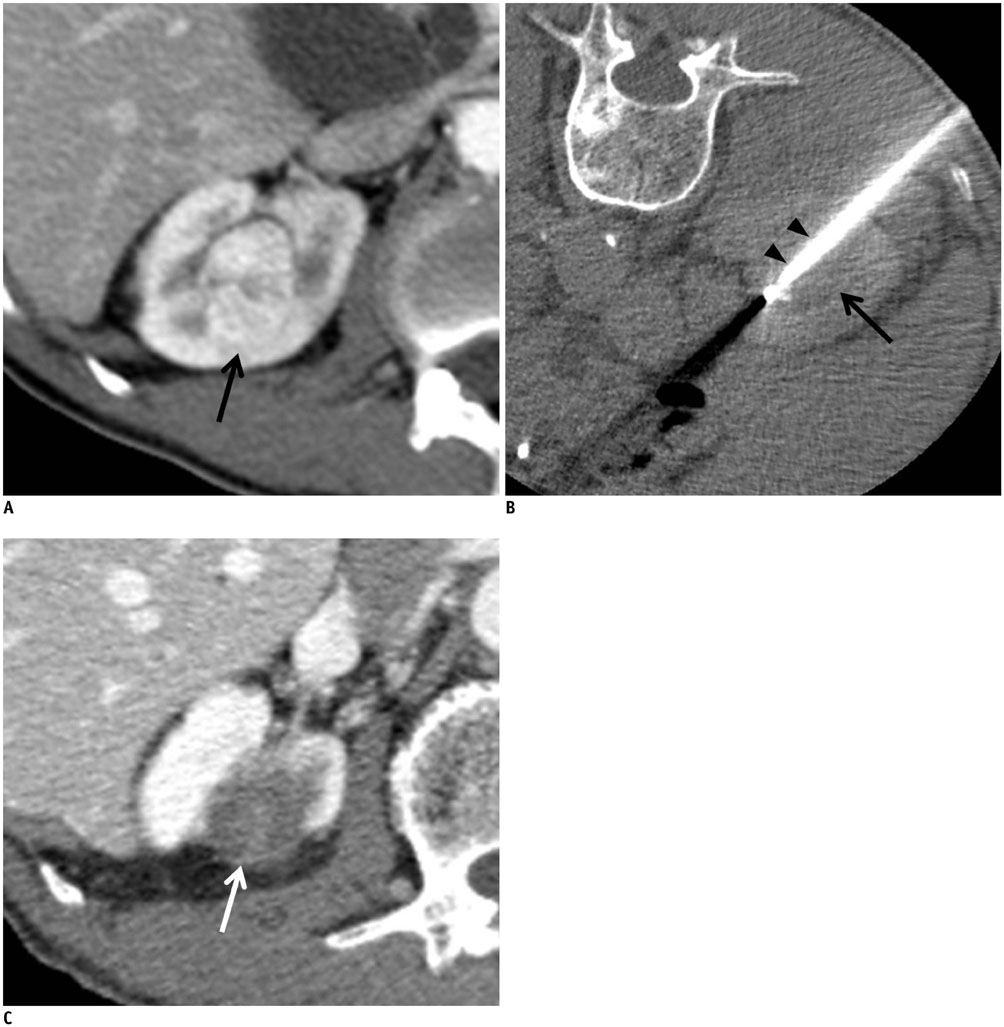
Fig. 1 67-year-old man with clear cell RCC. A. Pre-RFA contrast-enhanced CT image shows 3.1 cm endophytic RCC (arrow) in right kidney. Histologic diagnosis was confirmed clear cell RCC by US-guided biopsy. Pre-RFA creatinine and GFR were 0.98 mg/dL and 76.3 mL/min/1.73 m2, respectively. B. CT-guided RFA was performed with patient prone on CT table. CT image shows electrode (arrowheads) placed within tumor (arrow). C. 33-month post-RFA contrast-enhanced CT image shows complete tumor ablation (arrow) and no local tumor progression. Patient's creatinine increased to 1.0 mg/dL, and GFR decreased to 74.1 mL/min/1.73 m2. GFR = glomerular filtration rate, RCC = renal cell carcinoma, RFA = radiofrequency ablation, US = ultrasonography

Fig. 2 48-year-old man with clear cell RCC. A. Pre-RFA contrast-enhanced CT image shows 2.7 cm endophytic RCC (arrow) in left kidney. Histologic diagnosis was confirmed clear cell RCC with US-guided biopsy. Pre-RFA creatinine and GFR were 0.65 mg/dL and 131.1 mL/min/1.73 m2, respectively. B. Twelve-month contrast-enhanced CT image after first RFA shows nodular enhancement (arrowhead) at lateral aspect of tumor, suggesting local tumor progression. Second RFA was performed to treat recurrent RCC. C. Forty-month contrast-enhanced CT image after second RFA shows complete ablation of tumor (arrow). However, left kidney becomes atrophic because of uretero-pelvic stricture (arrowhead). Patient's creatinine increased to 1.11 mg/dL, and GFR decreased to 69.6 mL/min/1.73 m2. GFR = glomerular filtration rate, RCC = renal cell carcinoma, RFA = radiofrequency ablation, US = ultrasonography

Fig. 3 Kaplan-Meier survival analysis. This Kaplan-Meier survival curve illustrates excellent recurrence-free survival rate for patients with T1a RCC undergoing percutaneous RFA. Two-year recurrence-free survival rate is 96.0%. RCC = renal cell carcinoma, RFA = radiofrequency ablation
Reference
-
1. Zagoria RJ, Pettus JA, Rogers M, Werle DM, Childs D, Leyendecker JR. Long-term outcomes after percutaneous radiofrequency ablation for renal cell carcinoma. Urology. 2011; 77:1393–1397.2. Psutka SP, Feldman AS, McDougal WS, McGovern FJ, Mueller P, Gervais DA. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur Urol. 2013; 63:486–492.3. Lorber G, Glamore M, Doshi M, Jorda M, Morillo-Burgos G, Leveillee RJ. Long-term oncologic outcomes following radiofrequency ablation with real-time temperature monitoring for T1a renal cell cancer. Urol Oncol. 2014; 32:1017–1023.4. Chang X, Liu T, Zhang F, Ji C, Zhao X, Wang W, et al. Radiofrequency ablation versus partial nephrectomy for clinical T1a renal-cell carcinoma: long-term clinical and oncologic outcomes based on a propensity score analysis. J Endourol. 2015; 29:518–525.5. Park BK, Morrison PR, Tatli S, Govindarajulu U, Tuncali K, Judy P, et al. Estimated effective dose of CT-guided percutaneous cryoablation of liver tumors. Eur J Radiol. 2012; 81:1702–1706.6. Park BK, Kim CK, Lee HM. Image-guided radiofrequency ablation of Bosniak category III or IV cystic renal tumors: initial clinical experience. Eur Radiol. 2008; 18:1519–1525.7. Park JJ, Park BK, Park SY, Kim CK. Percutaneous radiofrequency ablation of sporadic Bosniak III or IV lesions: treatment techniques and short-term outcomes. J Vasc Interv Radiol. 2015; 26:46–54.8. Goldberg SN, Grassi CJ, Cardella JF, Charboneau JW, Dodd GD 3rd, Dupuy DE, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria. J Vasc Interv Radiol. 2009; 20:7 Suppl. S377–S390.9. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999; 130:461–447.10. Huda W, Ogden KM, Khorasani MR. Converting dose-length product to effective dose at CT. Radiology. 2008; 248:995–1003.11. Cardella JF, Kundu S, Miller DL, Millward SF, Sacks D;. Society of Interventional Radiology clinical practice guidelines. J Vasc Interv Radiol. 2009; 20:7 Suppl. S189–S191.12. Chae EJ, Kim JK, Kim SH, Bae SJ, Cho KS. Renal cell carcinoma: analysis of postoperative recurrence patterns. Radiology. 2005; 234:189–196.13. Gervais DA, McGovern FJ, Arellano RS, McDougal WS, Mueller PR. Radiofrequency ablation of renal cell carcinoma: part 1, indications, results, and role in patient management over a 6-year period and ablation of 100 tumors. AJR Am J Roentgenol. 2005; 185:64–71.14. Park BK, Kim CK, Choi HY, Lee HM, Jeon SS, Seo SI, et al. Limitation for performing ultrasound-guided radiofrequency ablation of small renal masses. Eur J Radiol. 2010; 75:248–252.15. Allaf ME, Varkarakis IM, Bhayani SB, Inagaki T, Kavoussi LR, Solomon SB. Pain control requirements for percutaneous ablation of renal tumors: cryoablation versus radiofrequency ablation--initial observations. Radiology. 2005; 237:366–370.16. Sung HH, Park BK, Kim CK, Choi HY, Lee HM. Comparison of percutaneous radiofrequency ablation and open partial nephrectomy for the treatment of size- and location-matched renal masses. Int J Hyperthermia. 2012; 28:227–234.17. Park SY, Park BK, Kim CK. Thermal ablation in renal cell carcinoma: what affects renal function? Int J Hyperthermia. 2012; 28:729–734.18. Park BK, Kim CK. Percutaneous radio frequency ablation of renal tumors in patients with von Hippel-Lindau disease: preliminary results. J Urol. 2010; 183:1703–1707.19. Park SY, Park BK, Kim CK, Lee HM, Jeon SS, Seo SI, et al. Percutaneous radiofrequency ablation of renal cell carcinomas in patients with von Hippel Lindau disease previously undergoing a radical nephrectomy or repeated nephron-sparing surgery. Acta Radiol. 2011; 52:680–685.20. Park BK, Kim CK, Park SY, Shen SH. Percutaneous radiofrequency ablation of renal cell carcinomas in patients with von Hippel Lindau disease: indications, techniques, complications, and outcomes. Acta Radiol. 2013; 54:418–427.21. Park BK, Kim CK. Complications of image-guided radiofrequency ablation of renal cell carcinoma: causes, imaging features and prevention methods. Eur Radiol. 2009; 19:2180–2190.22. Meloni MF, Goldberg SN, Moser V, Piazza G, Livraghi T. Colonic perforation and abscess following radiofrequency ablation treatment of hepatoma. Eur J Ultrasound. 2002; 15:73–76.23. Park BK, Kim CK, Moo HL. Arteriovenous fistula after radiofrequency ablation of a renal tumor located within the renal sinus. J Vasc Interv Radiol. 2007; 18:1183–1185.24. Eisenberg JD, Gervais DA, Singh S, Kalra MK, Sabir SH, Paul AB, et al. Radiation exposure from CT-guided ablation of renal masses: effects on life expectancy. AJR Am J Roentgenol. 2015; 204:335–342.25. Tsalafoutas IA, Tsapaki V, Triantopoulou C, Gorantonaki A, Papailiou J. CT-guided interventional procedures without CT fluoroscopy assistance: patient effective dose and absorbed dose considerations. AJR Am J Roentgenol. 2007; 188:1479–1484.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiofrequency ablation using real-time ultrasonography–computed tomography fusion imaging improves treatment outcomes for T1a renal cell carcinoma: Comparison with laparoscopic partial nephrectomy
- Spontaneous Regression of Pulmonary and Adrenal Metastases Following Percutaneous Radiofrequency Ablation of a Recurrent Renal Cell Carcinoma
- Imaging-Guided Biopsy, Percutaneous Ablation, and Active Surveillance for Small Renal Masses
- Recent developments in endoscopic ultrasound-guided radiofrequency ablation for pancreatic lesions
- Current status and future of radiofrequency ablation for hepatocellular carcinoma
