Usefulness of Myocardial Longitudinal Strain in Prediction of Heart Failure in Patients with Successfully Reperfused Anterior Wall ST-segment Elevation Myocardial Infarction
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Korea. shleemd@jbnu.ac.kr
- 2Research Institute of Clinical Medicine of Chonbuk National University, Jeonju, Korea.
- 3Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2458004
- DOI: http://doi.org/10.4070/kcj.2018.0421
Abstract
- BACKGROUND AND OBJECTIVES
Acute myocardial infarction-related heart failure (HF) is associated with poor outcome. This study was designed to investigate the usefulness of global longitudinal strain (GLS), global circumferential strain (GCS) and mean longitudinal strain of left anterior descending artery territory (LSant) measured by 2-dimensional speckle tracking echocardiography (2D STE) in prediction of acute anterior wall ST-segment elevation myocardial infarction (ant-STEMI)-related HF.
METHODS
A total of 171 patients with ant-STEMI who underwent successful primary coronary intervention and had available 2D STE data were enrolled. Patients were divided into 3 groups: in-hospital HF, post-discharge HF, and no-HF groups.
RESULTS
In-hospital and post-discharge HF developed in 39 (22.8%) and 13 (7.6%) of patients, respectively and 113 patients (69.6%) remained without HF. Multivariate analysis showed that GLS was the only factor significantly associated with the development of in-hospital HF. For post-discharge HF, LSant was the only independent predictor. Other echocardiographic or laboratory parameters did not show independent association with the development of ant-STEMI-related HF.
CONCLUSIONS
GLS is a powerful echocardiographic parameter related to development of in-hospital HF and LSant was significantly associated with post-discharge HF in patients with successfully reperfused ant-STEMI.
MeSH Terms
Figure
-

Figure 1 A flow chart showing the number of patients excluded, the reasons for exclusion and 3 groups in this study. HF = heart failure; LAD = left anterior descending artery; PCI = percutaneous coronary intervention; RWMA = regional wall motion abnormalities; STEMI = ST-segment elevation myocardial infarction.
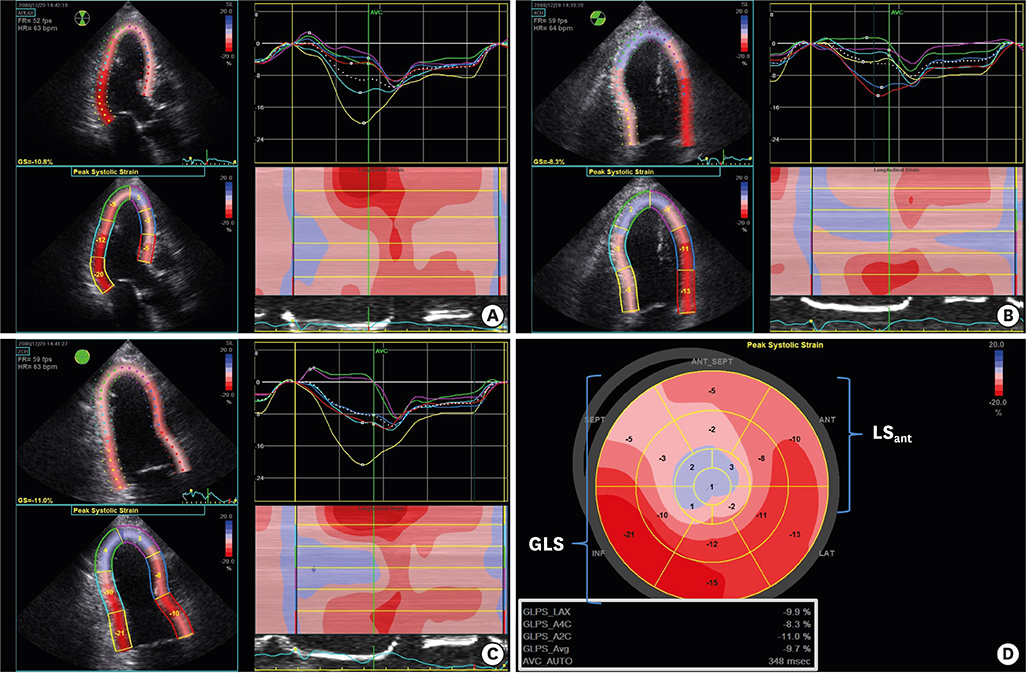
Figure 2 Measurement of GLS and LSant using two-dimensional speckle tracking echocardiography. (A-C) A region of interest is semiautomatically tracked in each of 3 apical images and software generates longitudinal strain curves for each 17 segments. (D) Note a bull's eye plot image and GLS. GLS = global longitudinal strain; LAD = left anterior descending artery; LSant = mean longitudinal strain of left anterior descending artery territory.

Figure 3 Bull's eye image plots in 2 contrastive cases of with ant-STEMI, the same LVEF of 48%, and single vessel disease on coronary angiography. Note the differences between (A) a 73-year-old man with GLS of −9.7% (LSant, −2.5%) who experienced in-hospital HF and (B) a 46-year-old man with GLS of −16.1% (LSant, −10.5%) without signs of HF. ant-STEMI = anterior wall ST-segment elevation myocardial infarction; GLS = global longitudinal strain; HF = congestive heart failure; LSant = mean longitudinal strain of left anterior descending artery territory; LVEF = left ventricular ejection fraction.

Figure 4 ROC curves testing and comparing values of GLS and LSant versus LVEF and NT-proBNP in predicting in-hospital and post-discharge HF in patients with ant-STEMI. (A) The AUC of GLS was 0.753 (95% CI, 0.682–0.816; p<0.001) which was comparable (p=0.532) with LVEF (AUC, 0.735; 95% CI, 0.662–0.800; p<0.001) and significantly higher (p=0.012) than that of NT-proBNP (AUC, 0.600; 95% CI, 0.516-0.679; p=0.072) to predict in-hospital HF. (B) In prediction of post-discharge HF, LSant (AUC, 0.715; 95% CI, 0.630–0.790; p=0.010) and NT-proBNP (AUC, 0.720; 95% CI, 0.628-0.801; p=0.005) were comparable (p=0.585), but LVEF showed poor discriminatory power (AUC, 0.643; 95% CI, 0.555–0.725; p=0.055). ant-STEMI = anterior wall ST-segment elevation myocardial infarction; AUC = area under the curve; CI = confidence interval; GLS = global longitudinal strain; HF = heart failure; LSant = mean longitudinal strain of left anterior descending artery territory; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-brain natriuretic peptide; ROC = receiver operating characteristic.
Cited by 2 articles
-
Two-dimensional Echocardiographic Assessment of Myocardial Strain: Important Echocardiographic Parameter Readily Useful in Clinical Field
Jae-Hyeong Park
Korean Circ J. 2019;49(10):908-931. doi: 10.4070/kcj.2019.0200.Myocardial Longitudinal Strain in Prediction of Heart Failure after Acute Myocardial Infarction
Hyemoon Chung
Korean Circ J. 2019;49(10):973-974. doi: 10.4070/kcj.2019.0132.
Reference
-
1. Hellermann JP, Goraya TY, Jacobsen SJ, et al. Incidence of heart failure after myocardial infarction: is it changing over time? Am J Epidemiol. 2003; 157:1101–1107.
Article2. Kelly DJ, Gershlick T, Witzenbichler B, et al. Incidence and predictors of heart failure following percutaneous coronary intervention in ST-segment elevation myocardial infarction: the HORIZONS-AMI trial. Am Heart J. 2011; 162:663–670.
Article3. Antoni ML, Mollema SA, Atary JZ, et al. Time course of global left ventricular strain after acute myocardial infarction. Eur Heart J. 2010; 31:2006–2013.
Article4. Farsalinos KE, Daraban AM, Ünlü S, Thomas JD, Badano LP, Voigt JU. Head-to-head comparison of global longitudinal strain measurements among nine different vendors: the EACVI/ASE Inter-Vendor Comparison Study. J Am Soc Echocardiogr. 2015; 28:1171–1181. e25. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015; 16:233–270.
Article6. Santoro GM, Carrabba N, Migliorini A, Parodi G, Valenti R. Acute heart failure in patients with acute myocardial infarction treated with primary percutaneous coronary intervention. Eur J Heart Fail. 2008; 10:780–785.
Article7. Velazquez EJ, Francis GS, Armstrong PW, et al. An international perspective on heart failure and left ventricular systolic dysfunction complicating myocardial infarction: the VALIANT registry. Eur Heart J. 2004; 25:1911–1919.
Article8. Antoni ML, Mollema SA, Delgado V, et al. Prognostic importance of strain and strain rate after acute myocardial infarction. Eur Heart J. 2010; 31:1640–1647.
Article9. Park YH, Kang SJ, Song JK, et al. Prognostic value of longitudinal strain after primary reperfusion therapy in patients with anterior-wall acute myocardial infarction. J Am Soc Echocardiogr. 2008; 21:262–267.
Article10. Antoni ML, Hoogslag GE, Boden H, et al. Cardiovascular mortality and heart failure risk score for patients after ST-segment elevation acute myocardial infarction treated with primary percutaneous coronary intervention (data from the Leiden MISSION! Infarct Registry). Am J Cardiol. 2012; 109:187–194.
Article11. Ersbøll M, Valeur N, Mogensen UM, et al. Relationship between left ventricular longitudinal deformation and clinical heart failure during admission for acute myocardial infarction: a two-dimensional speckle-tracking study. J Am Soc Echocardiogr. 2012; 25:1280–1289.12. Lewis EF, Velazquez EJ, Solomon SD, et al. Predictors of the first heart failure hospitalization in patients who are stable survivors of myocardial infarction complicated by pulmonary congestion and/or left ventricular dysfunction: a VALIANT study. Eur Heart J. 2008; 29:748–756.
Article13. Mega JL, Morrow DA, De Lemos JA, et al. B-type natriuretic peptide at presentation and prognosis in patients with ST-segment elevation myocardial infarction: an ENTIRE-TIMI-23 substudy. J Am Coll Cardiol. 2004; 44:335–339.
Article14. Kalam K, Otahal P, Marwick TH. Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart. 2014; 100:1673–1680.
Article15. Ersbøll M, Valeur N, Mogensen UM, et al. Prediction of all-cause mortality and heart failure admissions from global left ventricular longitudinal strain in patients with acute myocardial infarction and preserved left ventricular ejection fraction. J Am Coll Cardiol. 2013; 61:2365–2373.
Article16. Stanton T, Leano R, Marwick TH. Prediction of all-cause mortality from global longitudinal speckle strain: comparison with ejection fraction and wall motion scoring. Circ Cardiovasc Imaging. 2009; 2:356–364.17. Mignot A, Donal E, Zaroui A, et al. Global longitudinal strain as a major predictor of cardiac events in patients with depressed left ventricular function: a multicenter study. J Am Soc Echocardiogr. 2010; 23:1019–1024.
Article18. Munk K, Andersen NH, Nielsen SS, et al. Global longitudinal strain by speckle tracking for infarct size estimation. Eur J Echocardiogr. 2011; 12:156–165.
Article19. Bière L, Donal E, Terrien G, et al. Longitudinal strain is a marker of microvascular obstruction and infarct size in patients with acute ST-segment elevation myocardial infarction. PLoS One. 2014; 9:e86959.
Article20. Grabka M, Wita K, Tabor Z, et al. Prediction of infarct size by speckle tracking echocardiography in patients with anterior myocardial infarction. Coron Artery Dis. 2013; 24:127–134.
Article21. Ersbøll M, Valeur N, Mogensen UM, et al. Global left ventricular longitudinal strain is closely associated with increased neurohormonal activation after acute myocardial infarction in patients with both reduced and preserved ejection fraction: a two-dimensional speckle tracking study. Eur J Heart Fail. 2012; 14:1121–1129.
Article22. Shehata M. Value of two-dimensional strain imaging in prediction of myocardial function recovery after percutaneous revascularization of infarct-related artery. Echocardiography. 2015; 32:630–637.
Article23. Meimoun P, Abouth S, Clerc J, et al. Usefulness of two-dimensional longitudinal strain pattern to predict left ventricular recovery and in-hospital complications after acute anterior myocardial infarction treated successfully by primary angioplasty. J Am Soc Echocardiogr. 2015; 28:1366–1375.24. Park SM, Hong SJ, Kim YH, Ahn CM, Lim DS, Shim WJ. Predicting myocardial functional recovery after acute myocardial infarction: relationship between myocardial strain and coronary flow reserve. Korean Circ J. 2010; 40:639–644.
Article25. Zaliaduonyte-Peksiene D, Vaskelyte JJ, Mizariene V, Jurkevicius R, Zaliunas R. Does longitudinal strain predict left ventricular remodeling after myocardial infarction? Echocardiography. 2012; 29:419–427.26. Bochenek T, Wita K, Tabor Z, et al. Value of speckle-tracking echocardiography for prediction of left ventricular remodeling in patients with ST-elevation myocardial infarction treated by primary percutaneous intervention. J Am Soc Echocardiogr. 2011; 24:1342–1348.
Article27. Bonios MJ, Kaladaridou A, Tasoulis A, et al. Value of apical circumferential strain in the early post-myocardial infarction period for prediction of left ventricular remodeling. Hellenic J Cardiol. 2014; 55:305–312.28. Choi SW, Park JH, Sun BJ, et al. Impaired two-dimensional global longitudinal strain of left ventricle predicts adverse long-term clinical outcomes in patients with acute myocardial infarction. Int J Cardiol. 2015; 196:165–167.
Article29. Lewis EF, Moye LA, Rouleau JL, CARE Study, et al. Predictors of late development of heart failure in stable survivors of myocardial infarction: the CARE study. J Am Coll Cardiol. 2003; 42:1446–1453.
Article30. Jang SY, Yang DH, Kim NK, et al. Difference in the prognostic impact of left ventricular global longitudinal strain between anterior and nonanterior myocardial infarction. Echocardiography. 2016; 33:984–990.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Myocardial Longitudinal Strain in Prediction of Heart Failure after Acute Myocardial Infarction
- Coronary Slow Flow Phenomenon Leads to ST Elevation Myocardial Infarction
- Acute Myocardial Infarction by Right Coronary Artery Occlusion Presenting as Precordial ST Elevation on Electrocardiography
- The Prognostic Significance of Maximal Precordial ST-Segment Depression in Patients with Acute Inferior Myocardial Infarction
- Correlation of ST Segment Elevation in Lead V1 and the Conal Branch of Right Coronary Artery in Patients with Acute Anterior Wall Myocardial Infarction
