Neuroendocrine Tumor of the Renal Pelvis Presenting with Urinary Tract Obstruction: A Case Report
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. kyejin629@gmail.com
- KMID: 2457457
- DOI: http://doi.org/10.3348/jksr.2019.80.4.777
Abstract
- Primary renal neuroendocrine tumor (NET) is an extremely rare disease with fewer than 100 reported cases to date. Among them, only three involved the renal pelvis, to our knowledge. Here, we report another rare case of primary NET in the renal pelvis of a 33-year-old man. Initial computed tomography (CT) scanning of the abdomen and pelvis revealed a necrotic mass with peritumoral infiltration at the left renal pelvis and ureteropelvic junction causing urinary tract obstruction. A follow-up CT scan revealed an intratumoral hemorrhage. The patient then underwent nephrectomy. The results of a subsequent histopathological examination were consistent with a well-differentiated NET. No lymph nodes or paraganglia were found within the tumor, and further imaging revealed no other primary or metastatic lesions. Therefore, the patient was diagnosed with primary NET in the renal pelvis. We discuss this rare case and briefly review the current NET literature.
MeSH Terms
Figure
-
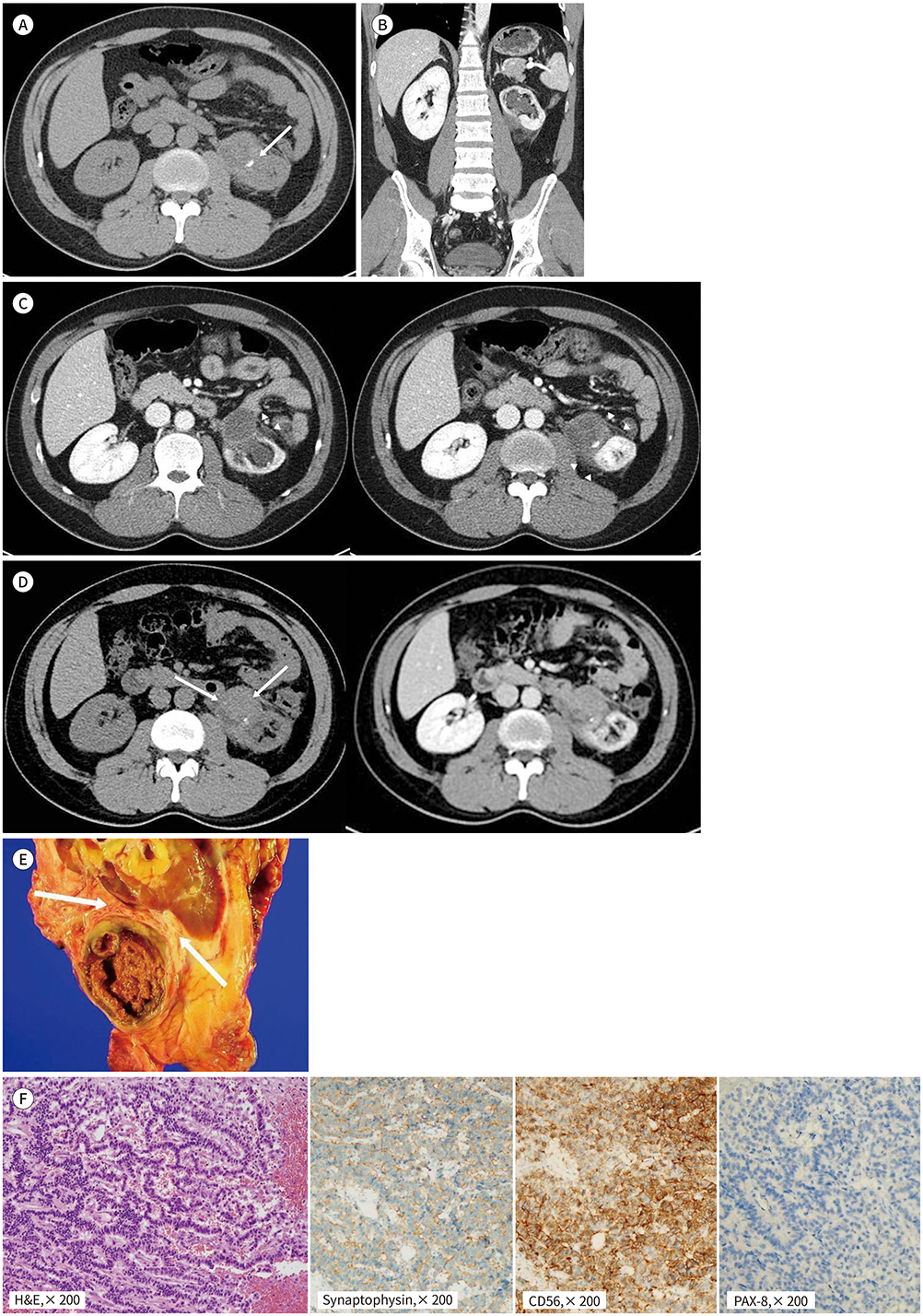
Fig. 1 A 33-year-old man with neuroendocrine tumor of the renal pelvis presenting with left flank pain. A. Precontrast CT scan reveals a hypodense mass with peripheral calcification (arrow) abutting the left renal pelvis. The center of the tumor is slightly hyperdense with a value of approximately +30 HU. B. A coronal reformatted post-contrast CT scan shows diffuse hydronephrosis and parenchymal atrophic changes in the left kidney, which are indicative of a chronic obstruction. C. On the contrast-enhanced CT scan, a thick-walled mass shows prominent peritumoral infiltration (arrow-heads) and suspicious peripheral mild enhancement (attenuation difference, approximately 30–45 HU). D. The follow-up CT scan shows high attenuation at the central portion of the mass (arrows) on precontrast (left panel) and enhanced (right panel) images. CT = computed tomography, HU = Hounsfield unit E. On gross examination, a 4.5 × 3.5 × 3.2-cm well-demarcated and grayish yellow-colored mass is found to extend to the renal sinus fat tissue but is separated from the renal parenchyma (arrows). F. The mass is composed of oval and round tumor cells arranged in a trabecular pattern on microscopic examination. Immunohistochemical staining demonstrated that neuroendocrine tumor cells have diffuse immunoreactivity to synaptophysin and CD56, without expression of PAX-8.
Reference
-
1. Lamb L, Shaban W. Primary renal carcinoid tumor: a radiologic review. Radiol Case Rep. 2015; 9:923.
Article2. Resnick ME, Unterberger H, McLoughlin PT. Renal carcinoid producing the carcinoid syndrome. Med Times. 1966; 94:895–896.3. Rudrick B, Nguyen GK, Lakey WH. Carcinoid tumor of the renal pelvis: report of a case with positive urine cytology. Diagn Cytopathol. 1995; 12:360–363.
Article4. Ji X, Li W. Primary carcinoid of the renal pelvis. J Environ Pathol Toxicol Oncol. 1994; 13:269–271.5. Kuroda N, Katto K, Tamura M, Shiotsu T, Hes O, Michal M, et al. Carcinoid tumor of the renal pelvis: consideration on the histogenesis. Pathol Int. 2008; 58:51–54.
Article6. Kruljac I, Pape U. The classification of neuroendocrine neoplasms: “neuroendocrine carcinomas” revisited—a 2017 update and future perspectives. Endocr Oncol Metab. 2017; 3:37–42.7. Lewis RB, Lattin GE Jr, Paal E. Pancreatic endocrine tumors: radiologic-clinicopathologic correlation. Radiographics. 2010; 30:1445–1464.
Article8. Bordeianou L, Vagefi PA, Sahani D, Deshpande V, Rakhlin E, Warshaw AL, et al. Cystic pancreatic endocrine neoplasms: a distinct tumor type? J Am Coll Surg. 2008; 206:1154–1158.
Article9. Takumi K, Fukukura Y, Higashi M, Ideue J, Umanodan T, Hakamada H, et al. Pancreatic neuroendocrine tumors: correlation between the contrast-enhanced computed tomography features and the pathological tumor grade. Eur J Radiol. 2015; 84:1436–1443.
Article10. Duan K, Mete O. Algorithmic approach to neuroendocrine tumors in targeted biopsies: practical applications of immunohistochemical markers. Cancer Cytopathol. 2016; 124:871–884.
Article
