A Comprehensive Review of Percutaneous Nephrostomy and Suprapubic Cystostomy
- Affiliations
-
- 1Department of Radiology, Gyeongsang National University School of Medicine, Gyeonsang National University Hospital, Jinju, Korea. lsmd10@naver.com
- 2Department of Radiology, Soonchunhyang University College of Medicine, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- 3Department of Radiology, Ewha Womans University School of Medicine, Ewha Womans University Hospital, Seoul, Korea.
- 4Department of Radiology, Gyeongsang National University School of Medicine, Gyeonsang National University Changwon Hospital, Changwon, Korea.
- KMID: 2457442
- DOI: http://doi.org/10.3348/jksr.2019.80.4.613
Abstract
- Percutaneous nephrostomy is widely used for the diagnosis and treatment of various urinary tract diseases, such as ureteral fistula, stenosis, and percutaneous nephrolithotomy, and the relief of urinary obstruction. Suprapubic cystostomy is also known as a good method for bladder drainage in patients with lower urinary tract obstruction or injury and neurogenic bladder. Despite the frequent use of these procedures, reports in the literature are insufficient for an interventional radiologist to understand the procedures easily and thoroughly. In this article, the indication, anatomy, placement, and postoperative management of percutaneous nephrostomy and suprapubic cystostomy have been described, explaining that the procedures are safe and effective.
MeSH Terms
Figure
-
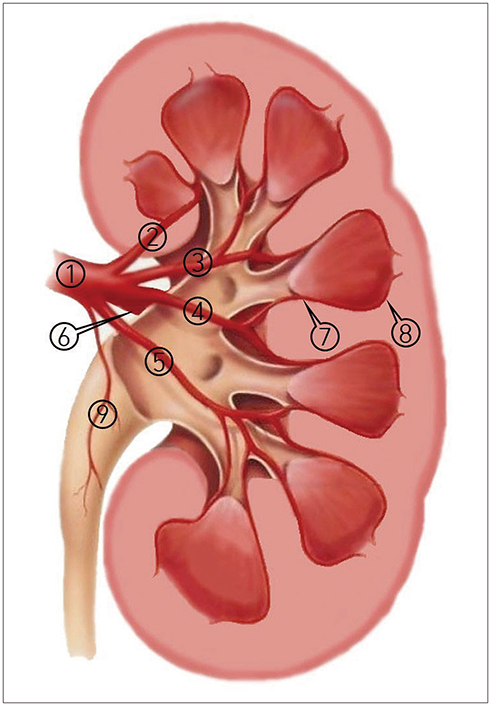
Fig. 1 Vascular anatomy of the kidney in the coronal plane. 1 = renal artery, 2 = superior segmental artery, 3 = anterior superior segmental artery, 4 = anterior inferior segmental artery, 5 = inferior segmental artery, 6 = posterior branch of the renal artery, 7 = interlobar arteries, 8 = arcuate artery, 9 = ureteric branch of the renal artery
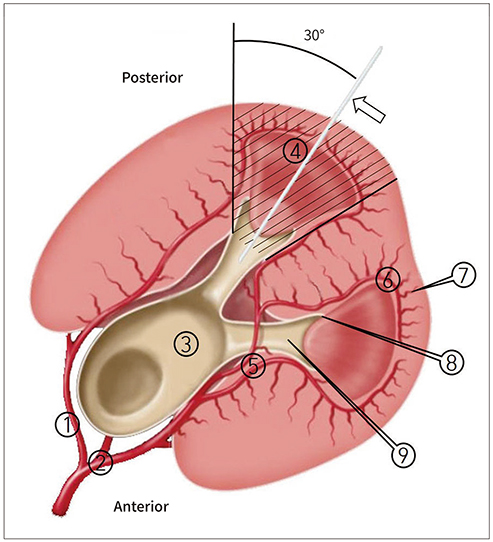
Fig. 2 Schematic anatomy of the kidney in the axial plane. The arrow indicates a needle within the posterior calyx along the plane of the Brodel's bloodless line. 1 = posterior division of the renal artery, 2 = anterior division of the renal artery, 3 = renal pelvis, 4 = Brodel's bloodless line, 5 = interlobar arteries, 6 = arcuate artery, 7 = interlobular arteries, 8 = fornix, 9 = minor calyx

Fig. 3 Comparison of PCN performed through the inferior calyx and middle calyx. A. A needle was percutaneously introduced in the inferior calyx (arrowheads). Under fluorosopy, PCN performed through the inferior calyx placing the catheter at a sharp angle to the urete. B. If a subsequent ureteral stent is needed, it is better to puncture the middle calyx (arrowheads). In the PCN performed through the middle calyx, an obtuse angle is formed between the catheter and the ureter, reducing resistance during the ureteral stent placement. PCN = percutaneous nephrostomy
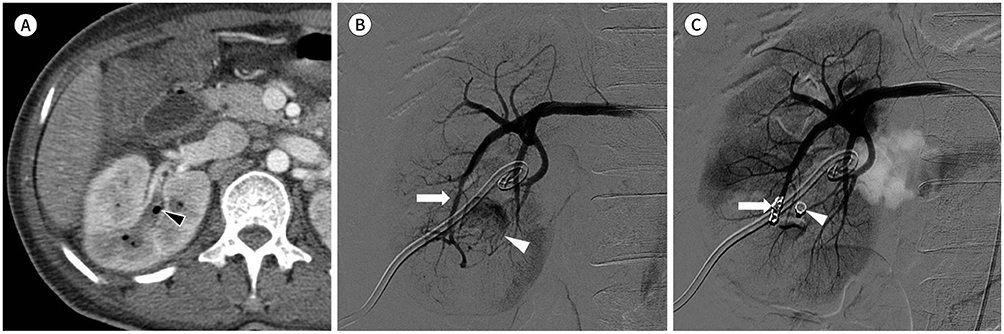
Fig. 4 A 41-year-old woman presenting with fever and flank pain. A. Contrast-enhanced CT shows pelvocalyceal dilatation with an internal air bubble (arrowhead), which suggests emphysematous pyelonephritis in the right kidney. Percutaneous nephrostomy was performed (not shown). B. Massive hematuria occurred immediately after the procedure. Right renal arteriogram shows a direct fistula between the inferior segmental artery (arrow) and inferior renal calyx (arrowhead). C. After embolization using microcoils (arrow), no further bleeding is seen on the right renal arteriogram. During the procedure, the microcoil migrated into the calyx (arrowhead).
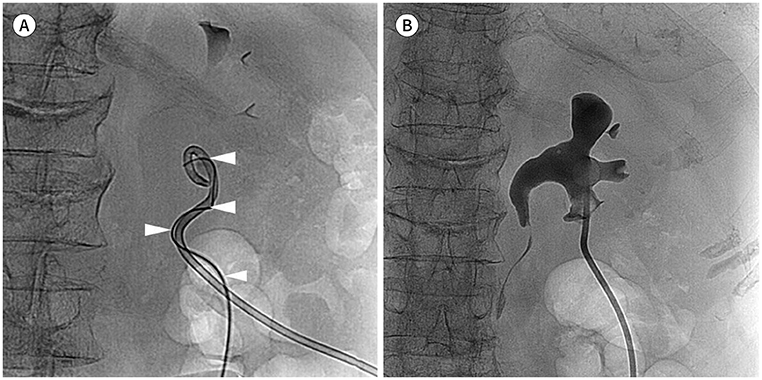
Fig. 5 An 80-year-old woman with bladder cancer replacing the drain catheter due to marked decrease of urination. A. Fluoroscopic image of the prone patient. A small amount of contrast media was injected through the catheter, but the 0.035-inch guidewire could not pass, as the catheter was clogged. Therefore, after inserting the guidewire (arrowheads) to the side of catheter, it could be advanced along the outer surface of the catheter. B. The existing catheter was removed, and a new catheter was inserted over the guidewire.

Fig. 6 A 53-year-old man with a double-J stent for ureteral stricture after kidney transplantation. At the follow-up, the patient presented with elevated serum creatinine. A. Percutaneous nephrostomy was performed for the transplanted kidney in the left lower abdomen. Under fluoroscopy, the catheter (arrow) was inserted via the anterosuperior calyx of the transplanted kidney. Arrowheads indicate a double-J ureteral stent. B. Two days after the procedure, the patient complained of abdominal pain, and free air was noted on the abdominal plain film (not shown). Contrast-enhanced CT shows that the catheter (arrowhead) penetrates the descending colon (arrow). Subsequently, the patient underwent primary repair for colon perforation.

Fig. 7 Percutaneous nephrostomy using the double-stick technique in a patient with a non-dilated renal collecting system. A. Fluoroscopic image after ultrasound-guided needle (22G) placement in the dilated pelvis of the right kidney. A small volume of urine was aspirated and an equivalent amount of diluted contrast was gently injected in the left renal collecting system. B. After opacifying the renal calyces and identifying the posterior calyx (arrowhead), a 21G second needle (arrow) was inserted toward the posterior calyx under fluoroscopic guidance. C. A 0.018-inch guidewire is inserted through the second needle. Once the wire was in the appropriate position, the first puncture needle was removed. D. After inserting a percutaneous access system (Neff, Cook, Bloomington, IN, USA) over the 0.018-inch guidewire, a 0.035-inch guidewire, dilators (arrow), and an 8.5-Fr pigtail catheter were subsequently inserted. Small hematomas are seen in the renal pelvis and calyces (arrowheads).

Fig. 8 Caudal view of the pelvis and anterior abdominal wall. Circle indicates the preferred puncture site. 1 = inferior epigastric artery, 2 = rectus abdominis muscle, 3 = bladder, 4 = space of Retzius, 5 = external iliac artery, 6 = reflected peritoneum
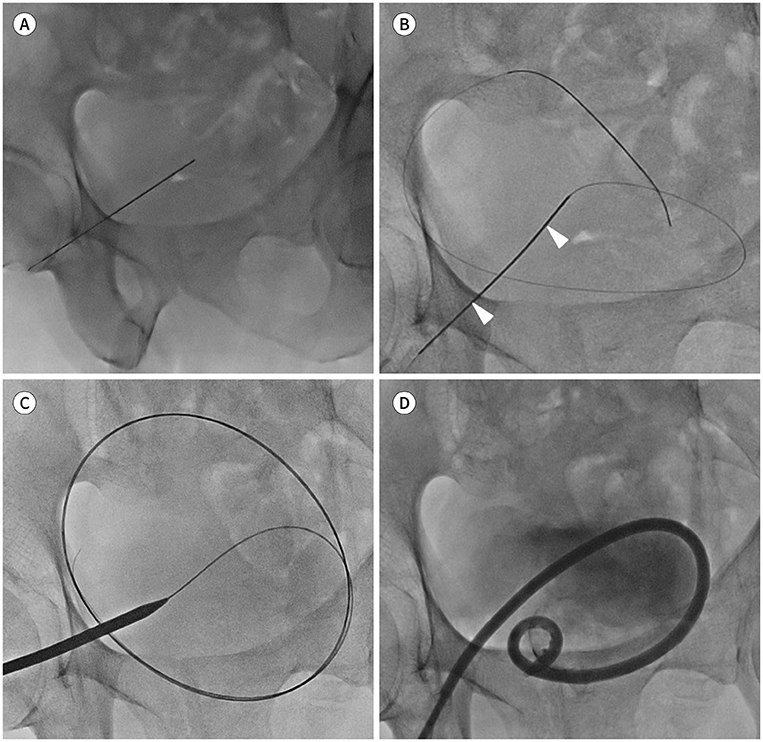
Fig. 9 A 59-year-old man presenting with urinary retention due to neurogenic bladder. A. Fluoroscopic image in a supine patient. A 21G needle was percutaneously inserted 2–3 cm above the pubic symphysis under ultrasound guidance. If bladder is not fully inflated, diluted contrast media should be injected through the indwelling transurethral catheter or a puncture needle. B. A 0.018-inch guidewire was inserted through the access needle (arrowheads). The needle was exchanged over the wire for the percutaneous access system (Neff, Cook, Bloomington, IN, USA), and the inner metal cannula was removed (not shown). C. A 0.035-inch guidewire was advanced into the bladder, and serial dilatation of the tract was performed over the wire. D. A 8.5-Fr pigtail catheter was subsequently inserted over the wire, and a small amount of contrast media was injected to confirm that the catheter was in an appropriate position.
Reference
-
1. Goodwin WE, Casey WC, Woolf W. Percutaneous trocar (needle) nephrostomy in hydronephrosis. J Am Med Assoc. 1955; 157:891–894.2. Zagoria RJ, Dyer RB. Do's and don't's of percutaneous nephrostomy. Acad Radiol. 1999; 6:370–377.3. Khan AA, Mathur S, Feneley R, Timoney AG. Developing a strategy to reduce the high morbidity of patients with long-term urinary catheters: the BioMed catheter research clinic. BJU Int. 2007; 100:1298–1301.4. Mohammed A, Khan A, Shergill IS, Gujral SS. A new model for suprapubic catheterization: the MediPlus Seldinger suprapubic catheter. Expert Rev Med Devices. 2008; 5:705–707.5. Pabon-Ramos WM, Dariushnia SR, Walker TG, D'Othée BJ, Ganguli S, Midia M, et al. Quality improvement guidelines for percutaneous nephrostomy. J Vasc Interv Radiol. 2016; 27:410–414.6. Dyer RB, Regan JD, Kavanagh PV, Khatod EG, Chen MY, Zagoria RJ. Percutaneous nephrostomy with extensions of the technique: step by step. Radiographics. 2002; 22:503–525.7. Funaki B, Tepper JA. Percutaneous nephrostomy. Semin Intervent Radiol. 2006; 23:205–208.8. Regalado SP. Emergency percutaneous nephrostomy. Semin Intervent Radiol. 2006; 23:287–294.9. Payne CS. A primer on patient management problems in interventional radiology. AJR Am J Roentgenol. 1998; 170:1169–1176.10. Moon E, Tam MD, Kikano RN, Karuppasamy K. Prophylactic antibiotic guidelines in modern interventional radiology practice. Semin Intervent Radiol. 2010; 27:327–337.11. Sampaio FJ, Aragão AH. Anatomical relationship between the renal venous arrangement and the kidney collecting system. J Urol. 1990; 144:1089–1093.12. Hopper KD, Yakes WF. The posterior intercostal approach for percutaneous renal procedures: risk of puncturing the lung, spleen, and liver as determined by CT. AJR Am J Roentgenol. 1990; 154:115–117.13. Graves FT. The anatomy of the intrarenal arteries and its application to segmental resection of the kidney. Br J Surg. 1954; 42:132–139.14. Munver R, Delvecchio FC, Newman GE, Preminger GM. Critical analysis of supracostal access for percutaneous renal surgery. J Urol. 2001; 166:1242–1246.15. Paul EM, Marcovich R, Lee BR, Smith AD. Choosing the ideal nephrostomy tube. BJU Int. 2003; 92:672–677.16. Degirmenci T, Gunlusoy B, Kozacioglu Z, Arslan M, Ceylan Y, Ors B, et al. Utilization of a modified Clavien Classification System in reporting complications after ultrasound-guided percutaneous nephrostomy tube placement: comparison to standard Society of Interventional Radiology practice guidelines. Urology. 2013; 81:1161–1167.17. Patel U, Hussain FF. Percutaneous nephrostomy of nondilated renal collecting systems with fluoroscopic guidance: technique and results. Radiology. 2004; 233:226–233.18. Montvilas P, Solvig J, Johansen TE. Single-centre review of radiologically guided percutaneous nephrostomy using “mixed” technique: success and complication rates. Eur J Radiol. 2011; 80:553–558.19. Sommer CM, Huber J, Radeleff BA, Hosch W, Stampfl U, Loenard BM, et al. Combined CT- and fluoroscopy-guided nephrostomy in patients with non-obstructive uropathy due to urine leaks in cases of failed ultrasound-guided procedures. Eur J Radiol. 2011; 80:686–691.20. Gupta S, Gulati M, Uday Shankar K, Rungta U, Suri S. Percutaneous nephrostomy with real-time sonographic guidance. Acta Radiol. 1997; 38:454–457.21. Lee WJ, Mond DJ, Patel M, Pillari GP. Emergency percutaneous nephrostomy: technical success based on level of operator experience. J Vasc Interv Radiol. 1994; 5:327–330.22. Patel RD, Newland C, Rees Y. Major complications after percutaneous nephrostomy-lessons from a department audit. Clin Radiol. 2004; 59:766.23. Lee WJ, Smith AD, Cubelli V, Badlani GH, Lewin B, Vernace F, et al. Complications of percutaneous nephrolithotomy. AJR Am J Roentgenol. 1987; 148:177–180.24. Lessne ML, Holly B, Huang SY, Kim CY. Diagnosis and management of hemorrhagic complications of interventional radiology procedures. Semin Intervent Radiol. 2015; 32:89–97.25. Stables DP. Percutaneous nephrostomy: techniques, indications, and results. Urol Clin North Am. 1982; 9:15–29.26. Narasimham DL, Jacobsson B, Vijayan P, Bhuyan BC, Nyman U, Holmquist B. Percutaneous nephrolithotomy through an intercostal approach. Acta Radiol. 1991; 32:162–165.27. Picus D, Weyman PJ, Clayman RV, McClennan BL. Intercostal-space nephrostomy for percutaneous stone removal. AJR Am J Roentgenol. 1986; 147:393–397.28. Gerspach JM, Bellman GC, Stoller ML, Fugelso P. Conservative management of colon injury following percutaneous renal surgery. Urology. 1997; 49:831–836.29. Öztürk H. Treatment of colonic injury during percutaneous nephrolithotomy. Rev Urol. 2015; 17:194–201.30. Millward SF. Percutaneous nephrostomy: a practical approach. J Vasc Interv Radiol. 2000; 11:955–964.31. Collares FB, Faintuch S, Kim SK, Rabkin DJ. Reinsertion of accidentally dislodged catheters through the original track: what is the likelihood of success? J Vasc Interv Radiol. 2010; 21:861–864.32. Krohmer SJ, Pillai AK, Guevara CJ, Bones BL, Dickey KW. Image-guided nephrostomy interventions: how to recognize, avoid, or get out of trouble. Tech Vasc Interv Radiol. 2018; 21:261–266.33. Praz V, Leisinger HJ, Pascual M, Jichlinski P. Urological complications in renal transplantation from cadaveric donor grafts: a retrospective analysis of 20 years. Urol Int. 2005; 75:144–149.34. Lojanapiwat B, Mital D, Fallon L, Koolpe H, Raja R, Badosa F, et al. Management of ureteral stenosis after renal transplantation. J Am Coll Surg. 1994; 179:21–24.35. Juaneda B, Alcaraz A, Bujons A, Guirado L, Díaz JM, Martí J, et al. Endourological management is better in early-onset ureteral stenosis in kidney transplantation. Transplant Proc. 2005; 37:3825–3827.36. Bhayani SB, Landman J, Slotoroff C, Figenshau RS. Transplant ureter stricture: acucise endoureterotomy and balloon dilation are effective. J Endourol. 2003; 17:19–22.37. Fonio P, Appendino E, Calandri M, Faletti R, Righi D, Gandini G. Treatment of urological complications in more than 1,000 kidney transplantations: the role of interventional radiology. Radiol Med. 2015; 120:206–212.38. Saad WE, Moorthy M, Ginat D. Percutaneous nephrostomy: native and transplanted kidneys. Tech Vasc Interv Radiol. 2009; 12:172–192.39. Gupta S, Gulati M, Suri S. Ultrasound-guided percutaneous nephrostomy in non-dilated pelvicaliceal system. J Clin Ultrasound. 1998; 26:177–179.40. Thanos L, Mylona S, Stroumpouli E, Kalioras V, Pomoni M, Batakis N. Percutaneous CT-guided nephrostomy: a safe and quick alternative method in management of obstructive and nonobstructive uropathy. J Endourol. 2006; 20:486–490.41. LeMaitre L, Mestdagh P, Marecaux-Delomez J, Valtille P, Dubrulle F, Biserte J. Percutaneous nephrostomy: placement under laser guidance and real-time CT fluoroscopy. Eur Radiol. 2000; 10:892–895.42. Manohar T, Jain P, Desai M. Supine percutaneous nephrolithotomy: effective approach to high-risk and morbidly obese patients. J Endourol. 2007; 21:44–49.43. Egilmez H, Oztoprak I, Atalar M, Cetin A, Gumus C, Gultekin Y, et al. The place of computed tomography as a guidance modality in percutaneous nephrostomy: analysis of a 10-year single-center experience. Acta Radiol. 2007; 48:806–813.44. Jiao D, Zhang Z, Sun Z, Wang Y, Han X. Percutaneous nephrolithotripsy: C-arm CT with 3D virtual navigation in non-dilated renal collecting systems. Diagn Interv Radiol. 2018; 24:17–22.45. Ghani KR, Andonian S, Bultitude M, Desai M, Giusti G, Okhunov Z, et al. Percutaneous nephrolithotomy: update, trends, and future directions. Eur Urol. 2016; 70:382–396.46. Kallidonis P, Panagopoulos V, Kyriazis I, Liatsikos E. Complications of percutaneous nephrolithotomy: classification, management, and prevention. Curr Opin Urol. 2016; 26:88–94.47. Tonolini M, Villa F, Ippolito S, Pagani A, Bianco R. Cross-sectional imaging of iatrogenic complications after extracorporeal and endourological treatment of urolithiasis. Insights Imaging. 2014; 5:677–689.48. Corder CJ, LaGrange CA. Suprapubic bladder catheterization. Treasure Island: StatPearls Publishing LLC;2018.49. Lee MJ, Papanicolaou N, Nocks BN, Valdez JA, Yoder IC. Fluoroscopically guided percutaneous suprapubic cystostomy for long-term bladder drainage: an alternative to surgical cystostomy. Radiology. 1993; 188:787–789.50. Okafor HT, Nsouli IS. Percutaneous bladder catheterization (suprapubic bladder catheterization). Atlas Oral Maxillofac Surg Clin North Am. 2015; 23:177–181.51. Papanicolaou N, Pfister RC, Nocks BN. Percutaneous, large-bore, suprapubic cystostomy: technique and results. AJR Am J Roentgenol. 1989; 152:303–306.52. Johnson S, Fiscus G, Sudakoff GS, O'Connor RC, Guralnick ML. The utility of abdominal ultrasound during percutaneous suprapubic catheter placement. Can J Urol. 2013; 20:6840–6843.53. Ahluwalia RS, Johal N, Kouriefs C, Kooiman G, Montgomery BS, Plail RO. The surgical risk of suprapubic catheter insertion and long-term sequelae. Ann R Coll Surg Engl. 2006; 88:210–213.54. Aguilera PA, Choi T, Durham BA. Ultrasound-guided suprapubic cystostomy catheter placement in the emergency department. J Emerg Med. 2004; 26:319–321.55. Ahmed SJ, Mehta A, Rimington P. Delayed bowel perforation following suprapubic catheter insertion. BMC Urol. 2004; 4:16.56. Hunter KF, Bharmal A, Moore KN. Long-term bladder drainage: Suprapubic catheter versus other methods: a scoping review. Neurourol Urodyn. 2013; 32:944–951.57. Katsumi HK, Kalisvaart JF, Ronningen LD, Hovey RM. Urethral versus suprapubic catheter: choosing the best bladder management for male spinal cord injury patients with indwelling catheters. Spinal Cord. 2010; 48:325–329.58. Feifer A, Corcos J. Contemporary role of suprapubic cystostomy in treatment of neuropathic bladder dysfunction in spinal cord injured patients. Neurourol Urodyn. 2008; 27:475–479.59. Navon JD, Soliman H, Khonsari F, Ahlering T. Screening cystoscopy and survival of spinal cord injured patients with squamous cell cancer of the bladder. J Urol. 1997; 157:2109–2111.60. Rigby D. An overview of suprapubic catheter care in community practice. Br J Community Nurs. 2009; 14:278280282–284.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Squamous Cell Carcinoma of the Suprapubic Cystostomy Tract With Bladder Involvement
- Efficacy of the Preliminary Ultrasonographic Examination before Suprapubic Cystostomy by Trocar
- Clinicel Observetion of Urethroplasty after Suprapubic Cystostomy in 11 Cases Urethral Injuries
- Suprapubic Cystostomy: Risk Analysis of Possible Bowel Interposition Through the Percutaneous Tract by Computed Tomography
- Treatment of Anterior Urethral Injury with Percutaneous Cystostomy
