Cancer Res Treat.
2016 Apr;48(2):491-498. 10.4143/crt.2015.088.
Objective Measurement of Cosmetic Outcomes of Breast Conserving Therapy Using BCCT.core
- Affiliations
-
- 1Department of Radiation Oncology, Seoul National University Bundang Hospital, Seongnam, Korea. inah228@snu.ac.kr
- 2Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2454325
- DOI: http://doi.org/10.4143/crt.2015.088
Abstract
- PURPOSE
The purpose of this study is to evaluate objective cosmetic outcomes and factors related to breast-conserving therapy (BCT) using the BCCT.core software.
MATERIALS AND METHODS
Fifty-one patients who received BCT with informed consent were evaluated using the BCCT.core software. Patients were divided into two groups based on the BCCT score: excellent or good (n=42) vs. fair or poor (n=9). Analysis of clinical factors was performed to determine factors affecting cosmetic outcomes.
RESULTS
The objective cosmetic outcome of BCT measured using the BCCT.core software was excellent in 10% of patients, good in 72%, and fair in 18%. None of the patients were classified as poor outcome. Tumor characteristics, systemic adjuvant therapy (chemotherapy and hormonal therapy), and radiation dose or energy of electron boost did not show correlation with the score measured by the BCCT.core program (p > 0.05). In univariate analysis, maximum dose within the breast (Dmax), width of tangential field, and excised tumor volume were smaller in patients with excellent or good by the BCCT.core compared to those with fair or poor (Dmax, 110.2±1.5% vs. 111.6±1.7%, p=0.019; width of tangential field, 8.0±1.1 cm vs. 8.6±0.7 cm, p=0.034; excised tumor volume, 64.0±35.8 cm3 vs. 95.3±54.4 cm3, p=0.067). In multivariate analysis, only Dmax was a significant factor for breast cosmetic outcome with a risk ratio of 1.697 (95% confidence interval, 1.006 to 2.863; p=0.047).
CONCLUSION
Objective measurement of cosmetic outcome of BCT using the BCCT.core software was feasible. The cosmetic outcome of BCT may be affected by the maximum dose within the breast.
MeSH Terms
Figure
-
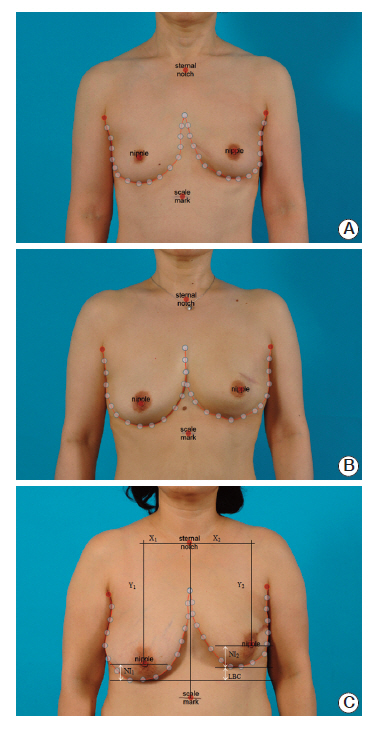
Fig. 1. Cosmetic results by BCCT.core. Representative examples of excellent outcome (A), good outcome (B), and fair outcome (C) are shown.
Reference
-
References
1. van Dongen JA, Bartelink H, Fentiman IS, Lerut T, Mignolet F, Olthuis G, et al. Randomized clinical trial to assess the value of breast-conserving therapy in stage I and II breast cancer, EORTC 10801 trial. J Natl Cancer Inst Monogr. 1992; (11):15–8.2. Harris JR, Levene MB, Svensson G, Hellman S. Analysis of cosmetic results following primary radiation therapy for stages I and II carcinoma of the breast. Int J Radiat Oncol Biol Phys. 1979; 5:257–61.
Article3. Cardoso MJ, Santos AC, Cardoso J, Barros H, Cardoso De Oliveira M. Choosing observers for evaluation of aesthetic results in breast cancer conservative treatment. Int J Radiat Oncol Biol Phys. 2005; 61:879–81.
Article4. Pezner RD, Patterson MP, Hill LR, Vora N, Desai KR, Archambeau JO, et al. Breast retraction assessment: an objective evaluation of cosmetic results of patients treated conservatively for breast cancer. Int J Radiat Oncol Biol Phys. 1985; 11:575–8.
Article5. Vrieling C, Collette L, Bartelink E, Borger JH, Brenninkmeyer SJ, Horiot JC, et al. Validation of the methods of cosmetic assessment after breast-conserving therapy in the EORTC "boost versus no boost" trial. EORTC Radiotherapy and Breast Cancer Cooperative Groups. European Organization for Research and Treatment of Cancer. Int J Radiat Oncol Biol Phys. 1999; 45:667–76.6. Heil J, Carolus A, Dahlkamp J, Golatta M, Domschke C, Schuetz F, et al. Objective assessment of aesthetic outcome after breast conserving therapy: subjective third party panel rating and objective BCCT.core software evaluation. Breast. 2012; 21:61–5.
Article7. Preuss J, Lester L, Saunders C. BCCT.core: can a computer program be used for the assessment of aesthetic outcome after breast reconstructive surgery? Breast. 2012; 21:597–600.8. Cardoso JS, Cardoso MJ. Towards an intelligent medical system for the aesthetic evaluation of breast cancer conservative treatment. Artif Intell Med. 2007; 40:115–26.
Article9. Cardoso MJ, Cardoso J, Amaral N, Azevedo I, Barreau L, Bernardo M, et al. Turning subjective into objective: the BCCT.core software for evaluation of cosmetic results in breast cancer conservative treatment. Breast. 2007; 16:456–61.
Article10. Heil J, Dahlkamp J, Golatta M, Rom J, Domschke C, Rauch G, et al. Aesthetics in breast conserving therapy: do objectively measured results match patients' evaluations? Ann Surg Oncol. 2011; 18:134–8.
Article11. Halperin EC, Wazer DE, Perez CA, Brady LW. Perez and Brady's principles and practice of radiation oncology. 6th ed. Philadelphia, PA: Lippincott Williams and Wilkins;2012. p. 1808.12. Hepel JT, Tokita M, MacAusland SG, Evans SB, Hiatt J, Price L, et al. Toxicity of 3D-CRT for accelerated partial breast irradiation. Int J Radiat Oncol Biol Phys. 2008; 72:S5.
Article13. Neal AJ, Torr M, Helyer S, Yarnold JR. Correlation of breast dose heterogeneity with breast size using 3D CT planning and dose-volume histograms. Radiother Oncol. 1995; 34:210–8.
Article14. Moody AM, Mayles WP, Bliss JM, A'Hern RP, Owen JR, Regan J, et al. The influence of breast size on late radiation effects and association with radiotherapy dose inhomogeneity. Radiother Oncol. 1994; 33:106–12.
Article15. Harsolia A, Kestin L, Grills I, Wallace M, Jolly S, Jones C, et al. Intensity-modulated radiotherapy results in significant decrease in clinical toxicities compared with conventional wedge-based breast radiotherapy. Int J Radiat Oncol Biol Phys. 2007; 68:1375–80.
Article16. Donovan E, Bleakley N, Denholm E, Evans P, Gothard L, Hanson J, et al. Randomised trial of standard 2D radiotherapy (RT) versus intensity modulated radiotherapy (IMRT) in patients prescribed breast radiotherapy. Radiother Oncol. 2007; 82:254–64.
Article17. Vrieling C, Collette L, Fourquet A, Hoogenraad WJ, Horiot JC, Jager JJ, et al. The influence of the boost in breast-conserving therapy on cosmetic outcome in the EORTC "boost versus no boost" trial. EORTC Radiotherapy and Breast Cancer Cooperative Groups. European Organization for Research and Treatment of Cancer. Int J Radiat Oncol Biol Phys. 1999; 45:677–85.18. Romestaing P, Lehingue Y, Carrie C, Coquard R, Montbarbon X, Ardiet JM, et al. Role of a 10-Gy boost in the conservative treatment of early breast cancer: results of a randomized clinical trial in Lyon, France. J Clin Oncol. 1997; 15:963–8.
Article19. Taylor ME, Perez CA, Halverson KJ, Kuske RR, Philpott GW, Garcia DM, et al. Factors influencing cosmetic results after conservation therapy for breast cancer. Int J Radiat Oncol Biol Phys. 1995; 31:753–64.
Article20. Hau E, Browne LH, Khanna S, Cail S, Cert G, Chin Y, et al. Radiotherapy breast boost with reduced whole-breast dose is associated with improved cosmesis: the results of a comprehensive assessment from the St. George and Wollongong randomized breast boost trial. Int J Radiat Oncol Biol Phys. 2012; 82:682–9.
Article21. Whelan TJ, Pignol JP, Levine MN, Julian JA, MacKenzie R, Parpia S, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010; 362:513–20.
Article22. Kim B, Shin SS, Kim SD, Noh DY, Ha SW. Cosmetic results of conservative treatment for early breast cancer. J Korean Soc Ther Radiol Oncol. 2011; 19:21–6.23. Van Limbergen E, Rijnders A, van der Schueren E, Lerut T, Christiaens R. Cosmetic evaluation of breast conserving treatment for mammary cancer. 2. A quantitative analysis of the influence of radiation dose, fractionation schedules and surgical treatment techniques on cosmetic results. Radiother Oncol. 1989; 16:253–67.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cosmetic Evaluation Methods Adapted to Asian Patients after Breast-Conserving Surgery and Examination of the Necessarily Elements for Cosmetic Evaluation
- Long-term results of oncoplastic breast surgery with latissimus dorsi flap reconstruction: a pilot study of the objective cosmetic results and patient reported outcome
- Comparison of Quality of Life and Cosmetic Outcome of Latissimus Dorsi Mini-Flap With Breast Conservation Surgery Without Reconstruction
- Long-term cosmesis following a novel schedule of accelerated partial breast radiation in selected early stage breast cancer: result of a prospective clinical trial
- Breast-Conserving Surgery With or Without Radiation Therapy for Early Breast Cancer
