Invasive Breast Cancer Presenting as a Mass Replaced by Calcification on Mammography: A Report of Two Cases
- Affiliations
-
- 1Department of Radiology, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea. jhrad@dau.ac.kr
- 2Pathology Reference Lab, Seegene Medical Foundation, Busan, Korea.
- 3Department of Surgery, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea.
- KMID: 2454041
- DOI: http://doi.org/10.3348/jksr.2019.80.3.591
Abstract
- A distinct calcification pattern is one of the criteria for determining the malignancy of breast cancer according to the Breast Imaging Reporting and Data System. A mass almost entirely replaced by calcification, however, is difficult to categorize and likely to be misdiagnosed. We present the report of two patients with invasive carcinoma of the breast that presented as a mass replaced by calcification on mammography. In the first case, the mass was confirmed as a mixed carcinoma comprising mucinous and micropapillary carcinoma, and in the second case, the mass was a mucinous carcinoma. Diagnosis of cancer in the latter case was missed as the mass had been assessed as a category 2 typically benign calcification at the first screening mammography 2 years ago. This report merits publication because it shows that a mass replaced by calcification on mammography can be misdiagnosed as a benign finding.
MeSH Terms
Figure
-

Fig. 1 A 50-year-old woman with a mixed-type mucinous carcinoma. A. Right mediolateral oblique mammogram shows a calcified mass, measuring 24 mm, with an oval shape and circumscribed margins in the clinically palpable upper inner area (arrow). B. Breast ultrasound image shows an irregular, indistinctly marginated, markedly hypoechoic mass with posterior shadowing. C. Subtraction image of dynamic contrast-enhanced breast MRI shows a heterogeneously enhancing mass (arrow) and a satellite enhancing nodule (open arrow). The kinetic curve shows initial fast and delayed plateau enhancement pattern (inset). D, E. In the surgical specimen, the mass shows collisional features with two histologically different types of carcinoma. The area on the right comprises a mucinous carcinoma with an abundant extracellular mucin pool, floating tumor cells, and multifocal microcalcifications (D, hematoxylin & eosin stain, × 10, arrow: microcalcification). The area on the left comprises a micropapillary carcinoma with central dense calcification and diffuse microcalcifications within micropapillary tumor cells (E, hematoxylin & eosin stain, × 200, arrows: microcalcification).
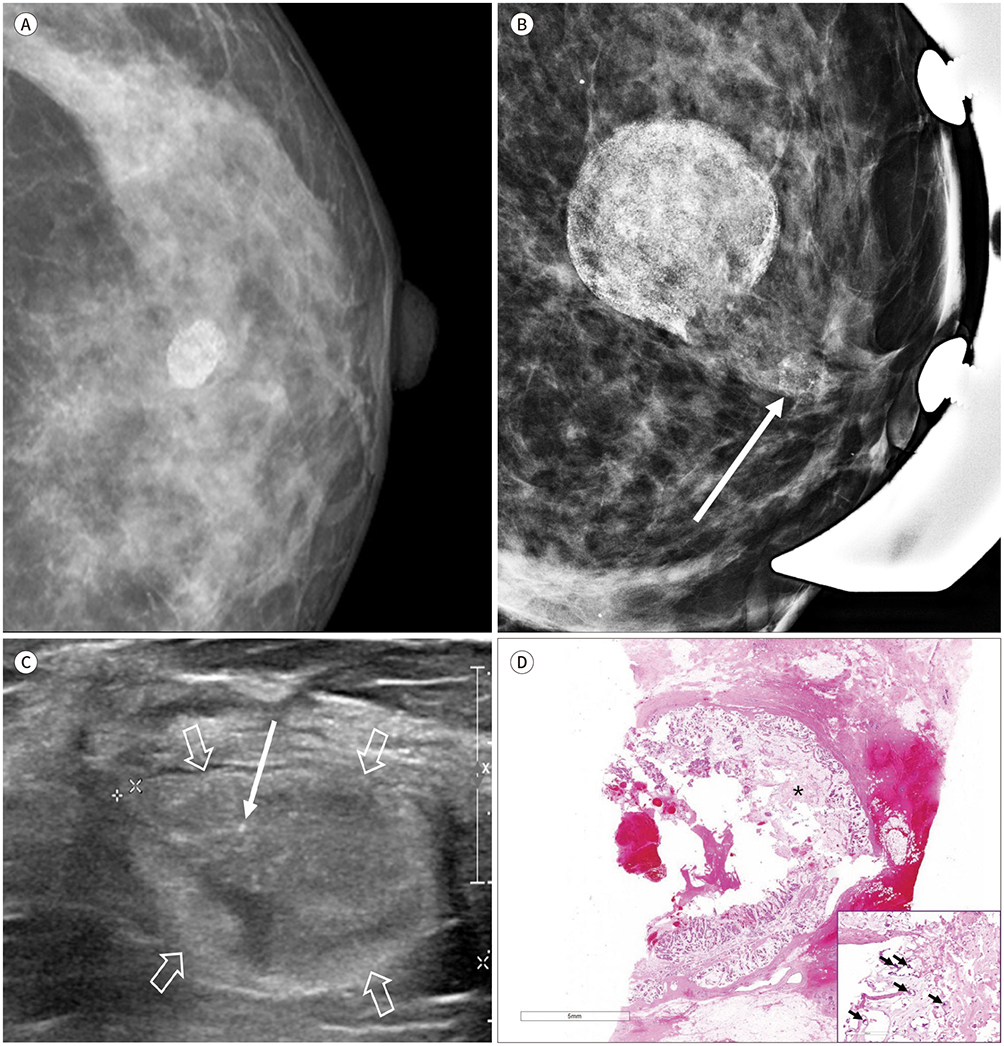
Fig. 2 A 46-year-old woman with a pure-type mucinous carcinoma. A. Left craniocaudal screening mammogram obtained at another hospital shows a calcified mass, measuring 13 mm, with circumscribed margins in the left central area. The mass had been assessed as a category 2 typically benign finding. B. Follow-up left magnification mammogram obtained after 2 years for a palpable lump in the left breast shows a mass with an increased size and a new group of calcifications in the left subareolar area (arrow). C. Breast US image obtained at another hospital shows an oval-shaped, circumscribed, and hyperechoic mass (open arrows) with suspected echogenic calcifications (arrow). D. In the excised specimen, a well-defined mass consisting of an abundant extracellular mucin pool with some floating carcinoma cells is observed. Diffuse microcalcification is noted within the mucin pool and tumor cells [hematoxylin & eosin stain, × 10 (inset: × 200); arrows: microcalcification; asterisk: mucin pool]
Reference
-
1. American College of Radiology. ACR BI-RADS atlas: breast imaging reporting and data system. 5th ed. Reston, VA: American College of Radiology;2013.2. Erguvan-Dogan B, Yazgan C, Atasoy C, Sak SD, Tukel S, Ceyhan K, et al. Radiologic-pathologic conference of the University of Ankara Medical School: metaplastic breast carcinoma with osteochondrosarcomatous differentiation. AJR Am J Roentgenol. 2005; 185:1593–1594.3. Lee JH, Kim EK, Choi SS, Nam KJ, Kim DC, Cho SH. Metaplastic breast carcinoma with extensive osseous differentiation: a case report. Breast. 2008; 17:314–316.
Article4. Evans HA, Shaughnessy EA, Nikiforov YE. Infiltrating ductal carcinoma of the breast with osseous metaplasia: imaging findings with pathologic correlation. AJR Am J Roentgenol. 1999; 172:1420–1422.
Article5. Wilson DA, Kalisher L, Port JE, Titus JM, Kirzner HL. Breast imaging case of the day. Pure mucinous carcinoma with calcifying matrix. Radiographics. 1997; 17:800–880.
Article6. Tani H, Murakami R, Yoshida T, Kumita S, Yanagihara K, Iida S, et al. Mucinous carcinoma of the breast accompanied by coarse calcification. Open J Med Imaging. 2012; 2:125–127.
Article7. Alghofaily KA, Almushayqih MH, Alanazi MF, Salamah AAB, Benediktsson H. Primary osteosarcoma of the breast arising in an intraductal papilloma. Case Rep Radiol. 2017; 2017:5787829.
Article8. Kim JH, Woo HY, Kim EK, Kim MJ, Moon HJ, Yoon JH. Metastatic osteosarcoma to the breast presenting as a densely calcified mass on mammography. J Breast Cancer. 2016; 19:87–91.
Article9. Ozsaran AA, Dikmen Y, Terek MC, Ulukus M, Ozdemir N, Orgüc S, et al. Bilateral metastatic carcinoma of the breast from primary ovarian cancer. Arch Gynecol Obstet. 2000; 264:166–167.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mucinous Breast Carcinoma Presenting as a Coarse and Densely Calcified Mass on Mammography: A Case Report
- Mammographic findings of breast cancer: Emphasis on the tumor and microcalcifications
- Misdiagnosed Breast Cancer on Mammography Retrospective Analysis in 17 Cases
- Usefulness of Ultrasonography for Detection of Breast Cancer in Patients under 30 Years of Age
- Early screening for breast cancer
