Multidetector CT in Blunt Abdominal Trauma: Imaging Findings and Pitfalls
- Affiliations
-
- 1Department of Radiology, Yonsei University Wonju College of Medicine, Wonju Severance Christian Hospital, Wonju, Korea. radajh@yonsei.ac.kr
- KMID: 2454025
- DOI: http://doi.org/10.3348/jksr.2019.80.3.445
Abstract
- Owing to the developments in imaging modalities, imaging has become an essential element in the early evaluation of and decision-making algorithm for patients with trauma. In particular, CT technology has developed over the past decades, resulting in faster image acquisition and higher image quality. Currently, CT is the key imaging modality for triaging surgical and non-surgical treatment in patients with abdominal trauma and plays an important role in increasing the frequency and success rate of non-surgical treatment. Because rapid and accurate diagnosis of injury in patients with trauma can improve the patients' prognosis, radiologists should be familiar with the imaging findings, especially the CT findings, in patients with trauma. In this article, the authors reviewed the considerations when performing CT for evaluating abdominal trauma. In addition, they described the important imaging findings and pitfalls when diagnosing blunt trauma in various intra-abdominal organs.
MeSH Terms
Figure
-
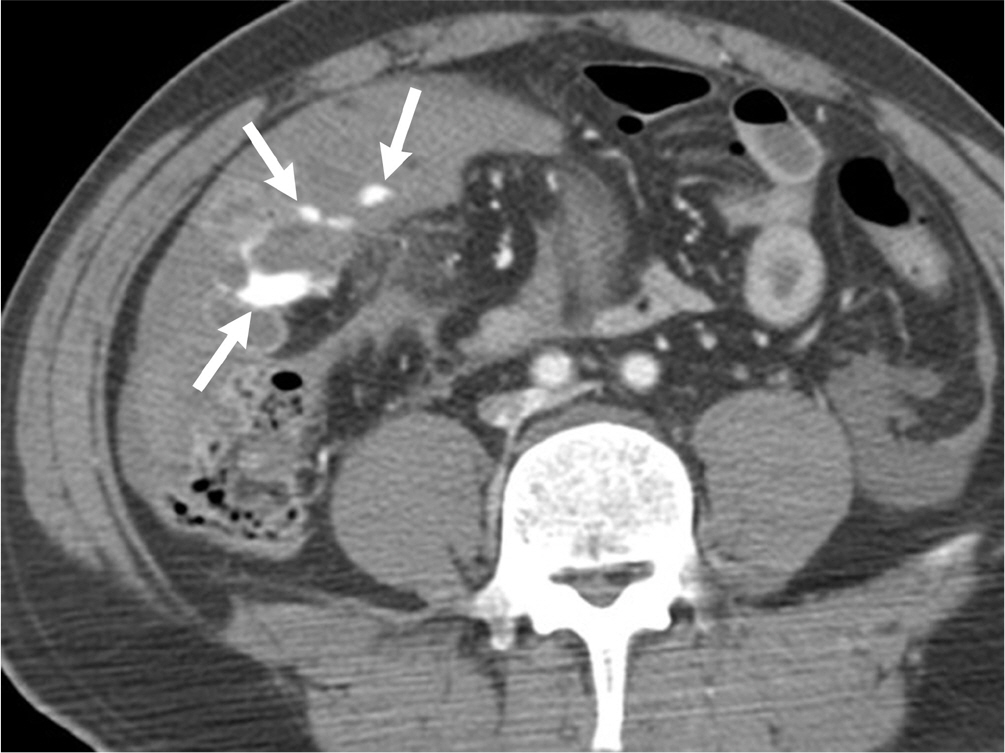
Fig. 1. Active bleeding in a 49-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows contrast extravasation (arrows) at the mesentery.

Fig. 2. The sentinel clot sign in a 59-year-old man after a motor vehicle accident. A. The non-enhanced axial CT image demonstrates the difference in density between the hemoperitoneum (32 HU, black asterisk) around the liver and the clot (69 HU, white asterisk) around the spleen. B. The contrast-enhanced CT image shows the lacerations (arrows) in the spleen. HU = Hounsfield unit

Fig. 3. Liver laceration in an 18-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows irregular and linear low-attenuation areas (arrows) in the liver, consistent with a laceration.

Fig. 4. Intraparenchymal hematoma in a 22-year-old man after beating. The contrast-enhanced CT image demonstrates an ill-defined, round, low-attenuation area (arrows) in the right posterior section of the liver.
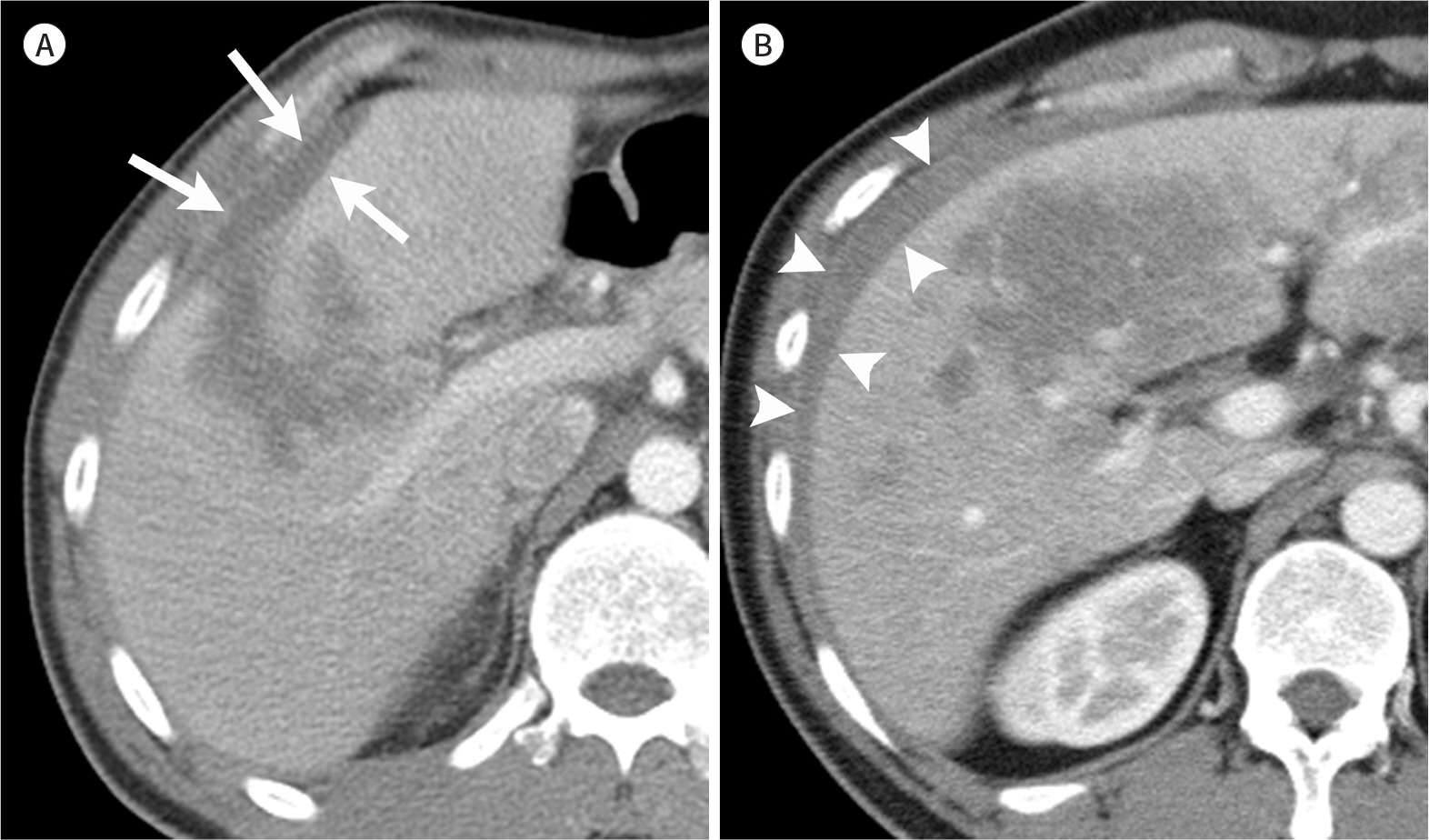
Fig. 5. Subcapsular hematoma versus perihepatic hematoma. A. Subcapsular hematoma in a 35-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows the elliptic collection of a low-attenuation area (arrows) between the liver capsule and the parenchyma, which caused indentation of the liver margin. B. However, such a finding is not seen in perihepatic hematoma (arrowheads) in a 24-year-old man after a motor vehicle accident.
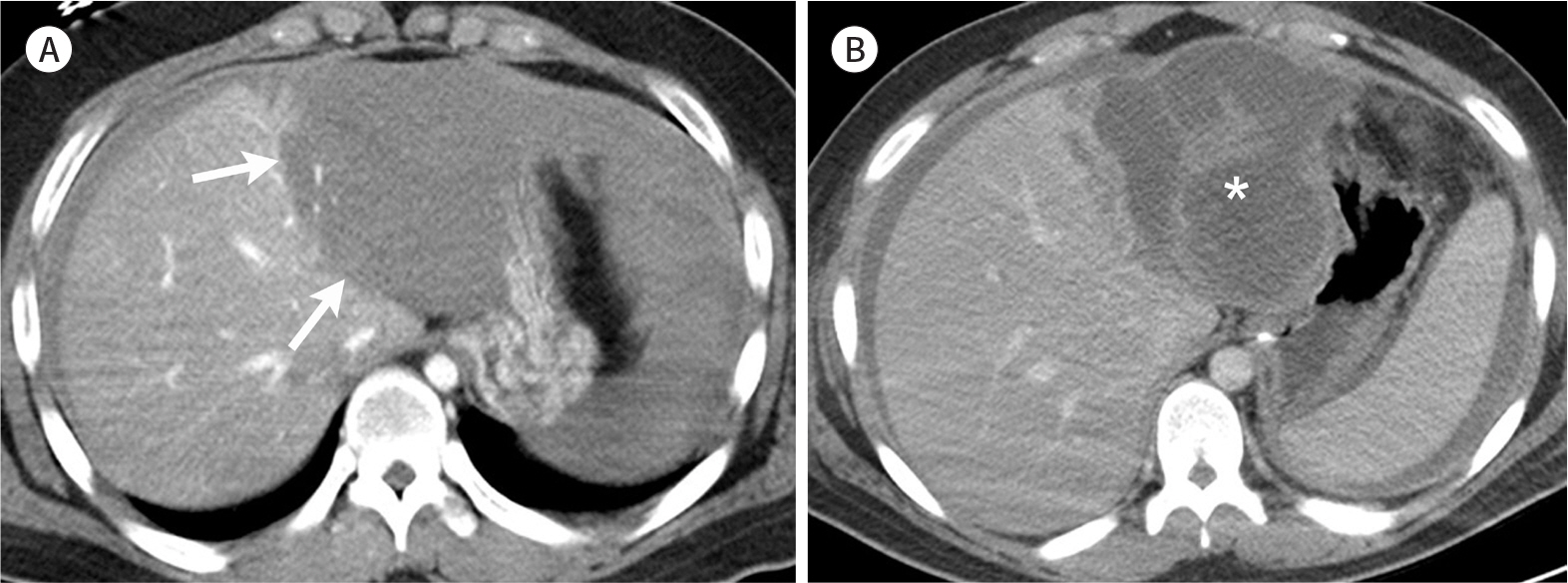
Fig. 6. Hepatic infarction in a 17-year-old man after a motor vehicle accident. A. The contrast-enhanced CT image shows a lack of perfusion (arrows) to the left lateral section of the liver. B. The follow-up contrast-enhanced CT image acquired 7 days later shows total necrosis (asterisk) of the left lateral section of the liver.

Fig. 7. Periportal low attenuation in an 18-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows low-attenuation areas around the portal vein and its branch (arrows). Note the laceration that extends to the portal vein branch (arrowheads).
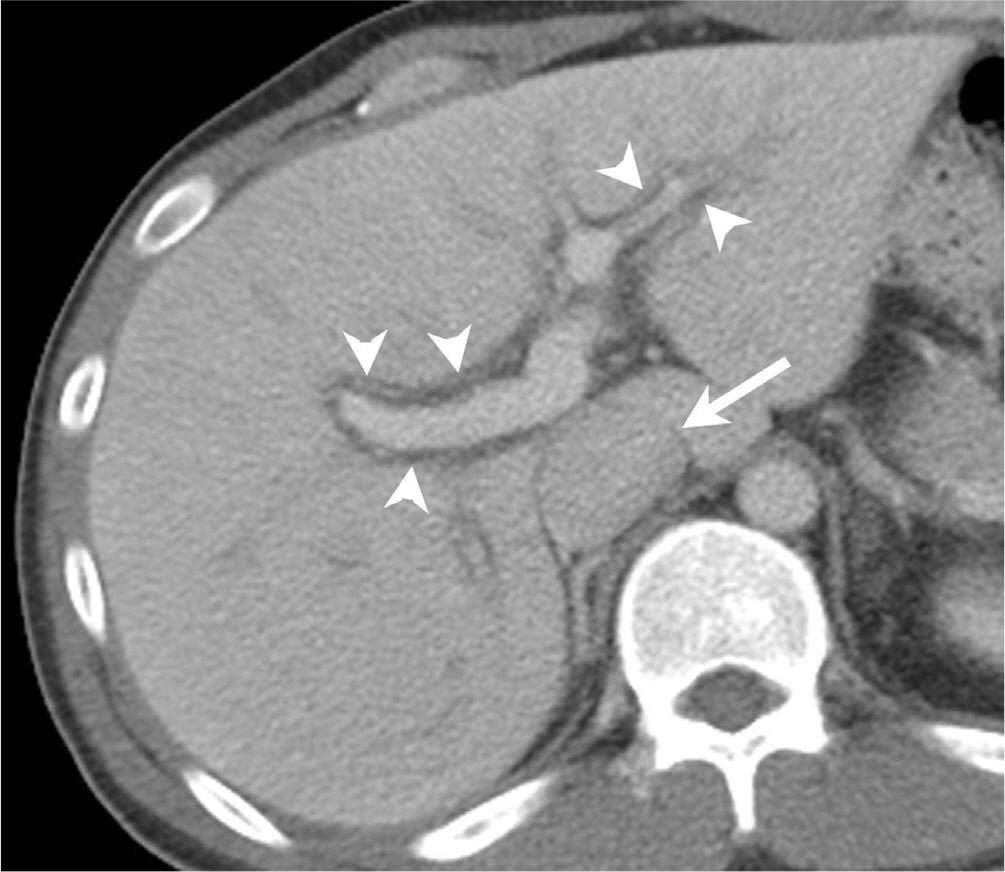
Fig. 8. Periportal low attenuation in a 31-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows low-attenuation areas around the portal vein and its branches (arrowheads). A finding of marked distention of the inferior vena cava (arrow) may indicate vigorous fluid replacement.

Fig. 9. Hepatic hemangioma initially diagnosed as hematoma in a 68-year-old man after a motor vehicle accident. A. The initial contrast-enhanced CT image demonstrates a low-attenuation lesion (arrow) in the left hemiliver, simulating a liver hematoma. B. The contrast-enhanced CT image acquired 3 days later shows peripheral-enhancing portions (arrowheads) within the low-attenuation lesion (arrow), which are most consistent with a hemangioma. Note the hepatic hematoma in the right hemiliver (black arrow).
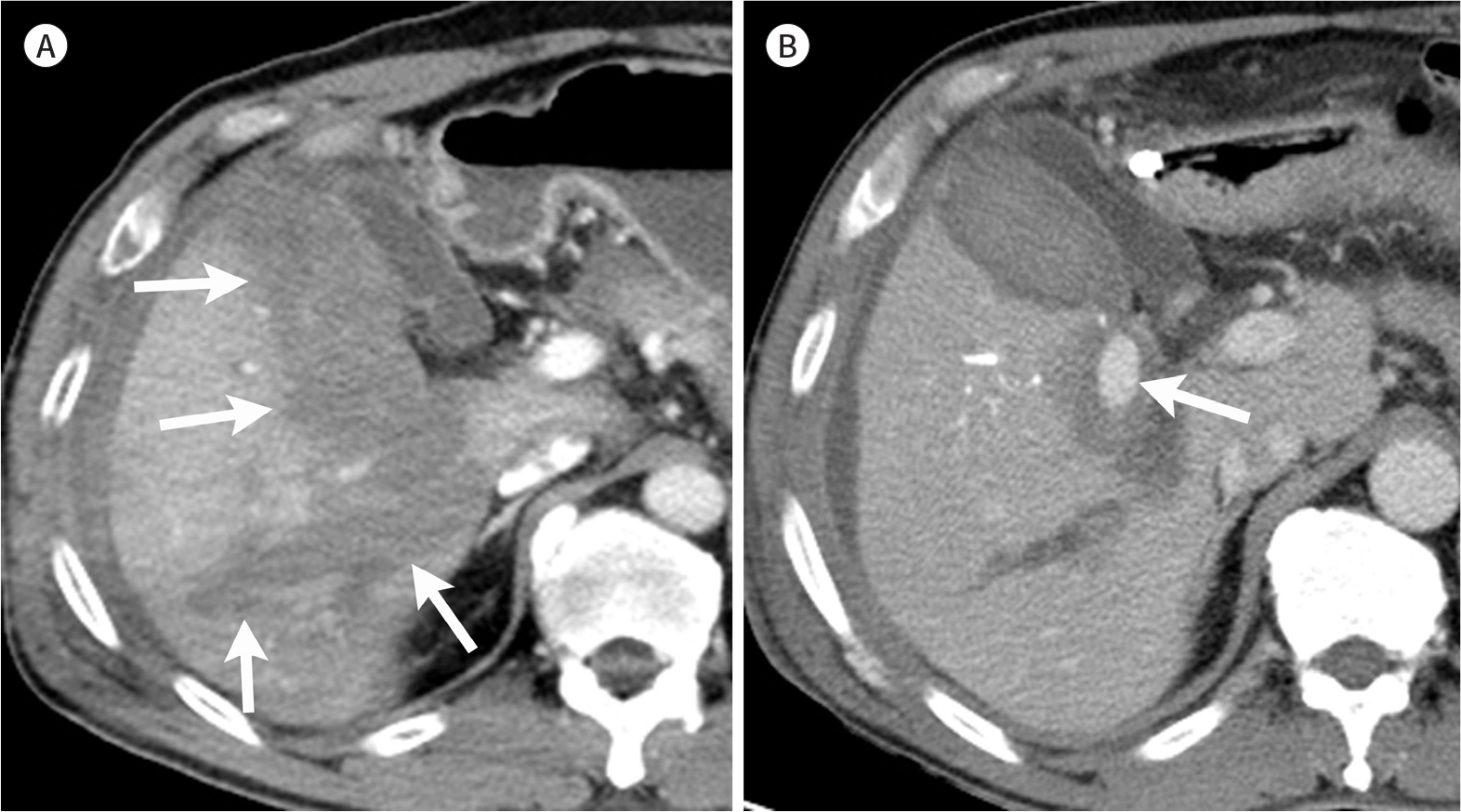
Fig. 10. Post-traumatic pseudoaneurysm in a 56-year-old man after a 2-meter fall. A. The initial contrast-enhanced CT image shows a large hematoma (arrows) in the right hemiliver. B. The contrast-enhanced CT image acquired 18 days later shows a newly developed, well-defined pseudoaneurysm (arrow) within the hepatic hematoma.
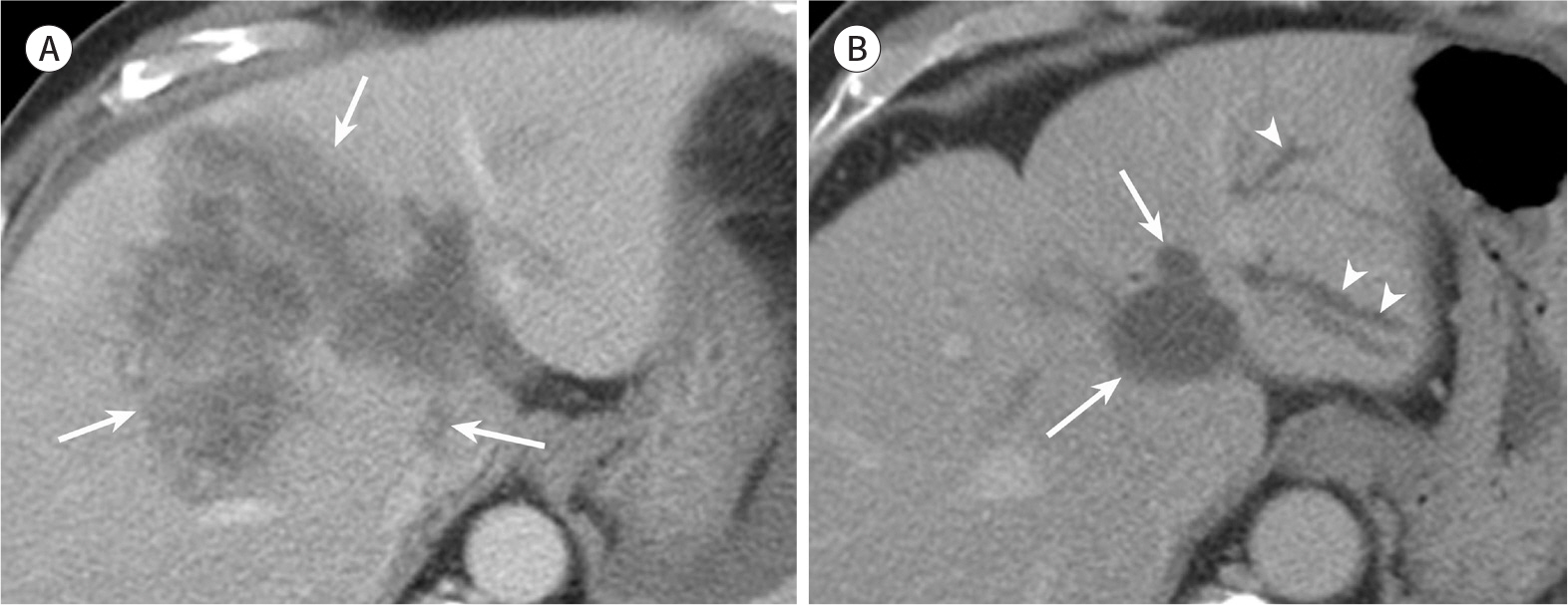
Fig. 11. Bile duct injury in a 63-year-old man after a motor vehicle accident. A. The initial contrast-enhanced CT image shows multiple lacerations and hematoma (arrows) in the medial section of the left liver and anterior section of the right liver. B. The follow-up contrast-enhanced CT image acquired 83 days later shows the development of a biloma (arrows) and left intrahepatic duct dilatation (arrowheads).

Fig. 12. Splenic laceration in a 31-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows an irregular and linear low-attenuation area (arrows) in the spleen. Hematoma in the left adrenal gland is also seen (arrowheads).

Fig. 13. Congenital cleft in a 42-year-old man after a motor vehicle accident. The contrast-enhanced CT image demonstrates a smooth low-attenuation line (arrows) in the spleen without perisplenic fluid collection. Note the lacerations of the liver (arrowheads).
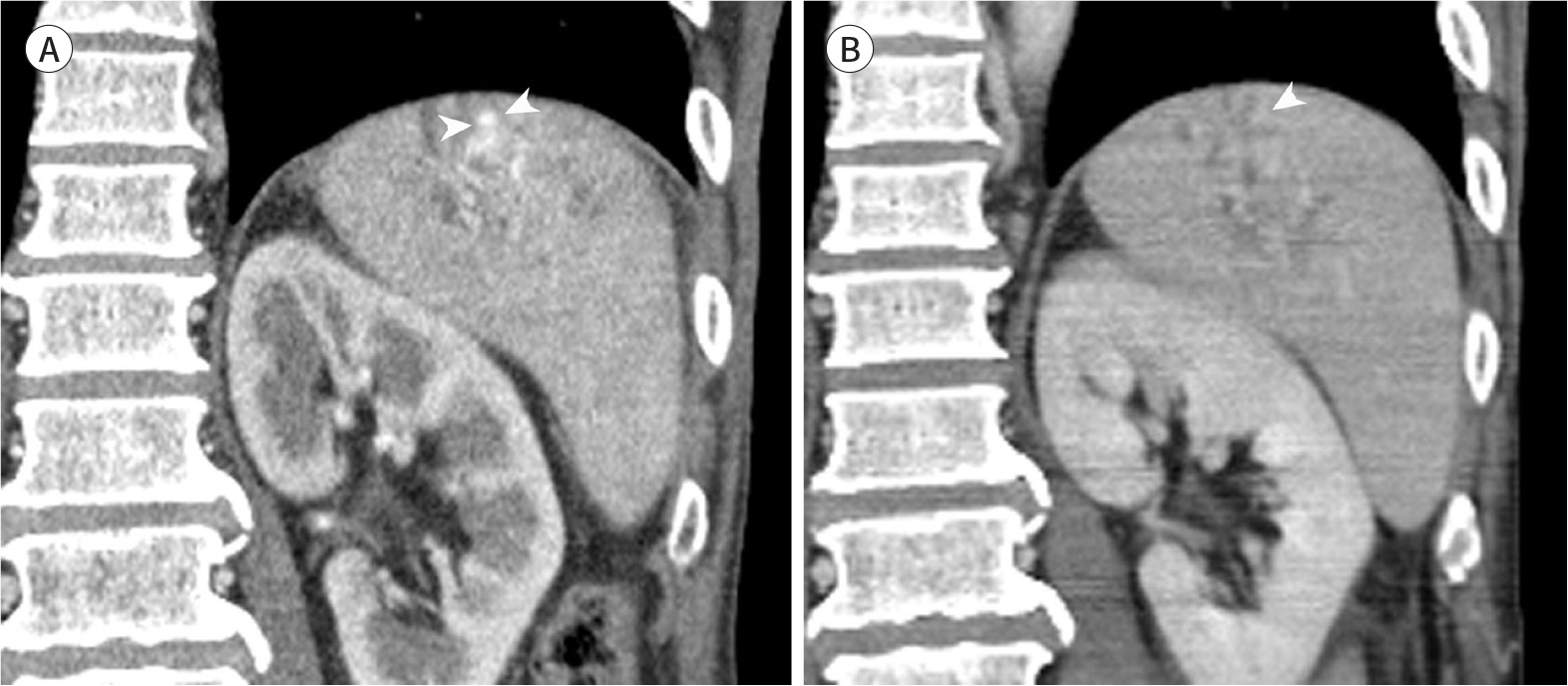
Fig. 14. Splenic pseudoaneurysm in a 54-year-old man after a motor vehicle accident. A. The contrast-enhanced CT image acquired in an early phase of enhancement during chest CT shows a high-attenuation area (arrowheads) in the spleen. B. The contrast-enhanced CT image acquired in the portal venous phase of enhancement shows that the
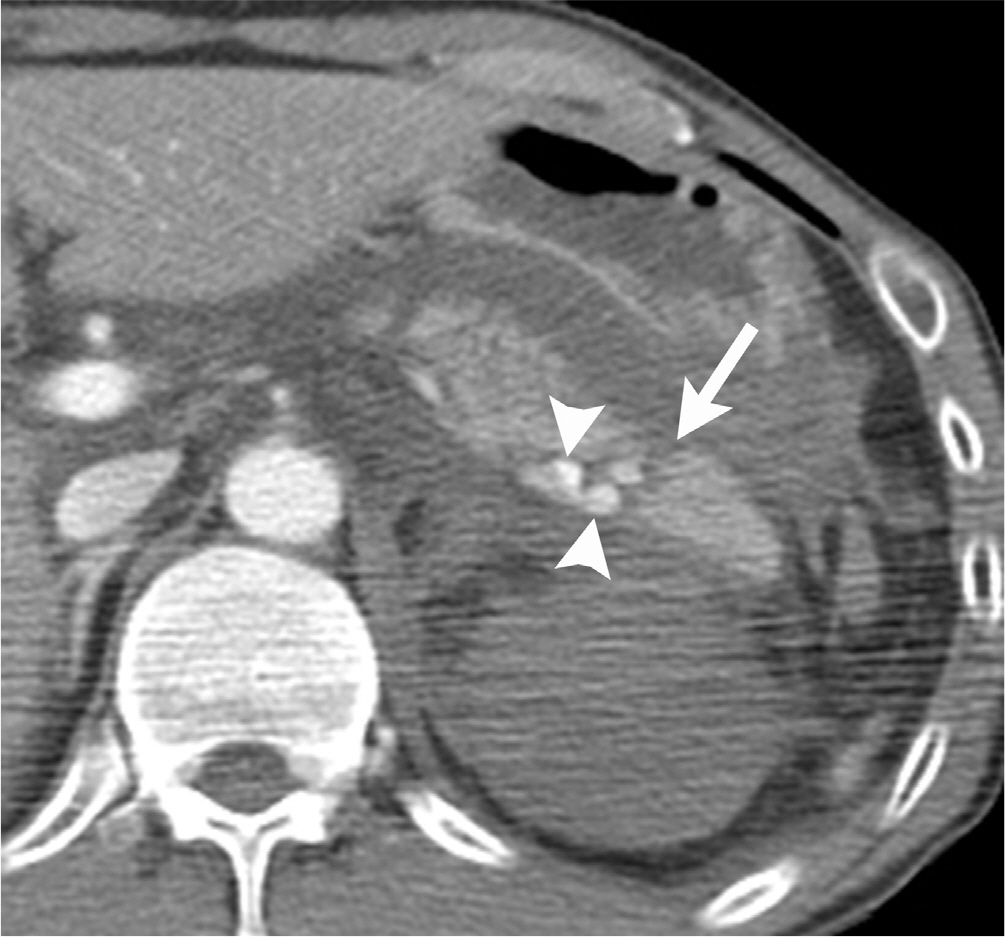
Fig. 15. Transection of the pancreas with active bleeding in a 47-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows a linear low-attenuation area (arrow) across the pancreatic tail. Note the high-attenuation contrast material extravasation (arrowheads) within the intrapancreatic hematoma.

Fig. 16. Pancreatic laceration with the disruption of the pancreatic duct in a 43-year-old man after a motor vehicle accident. A. The contrast-enhanced CT image shows a deep laceration with hematoma (arrows) in the pancreatic tail. B. The endoscopic retrograde pancreatogram shows extravasation (arrows) of contrast material from a pancreatic duct, indicating duct disruption.

Fig. 17. Sigmoid colon perforation in a 57-year-old man after a motor vehicle accident. A large mural defect is seen at the sigmoid colon (arrows) with feces (F) spilling from the lumen (L) and multifocal intraperitoneal extraluminal air (arrowheads).

Fig. 18. Large bowel transection in a 49-year-old man after a motor vehicle accident. The contrast-enhanced CT image shows abnormal dual bowel wall enhancement (both increased and decreased), as well as the Janus sign (arrowheads). The surrounding hematoma (arrows) makes it difficult to recognize the transected bowel end.

Fig. 19. Monnettsrreaanssttt–eeernnichh haaennmcceeaddt o CCmTT aiimm inaa ggaeen sa8hc7oq-ywueisra erfod-oc 2lad0l mhdaaazynisn aleafsttese rr(aasrh mroowowtsso)tr ih nvee t hrheiecs lomel uaetcsiceoinndt eeonrf ytm. esenteric haziness.
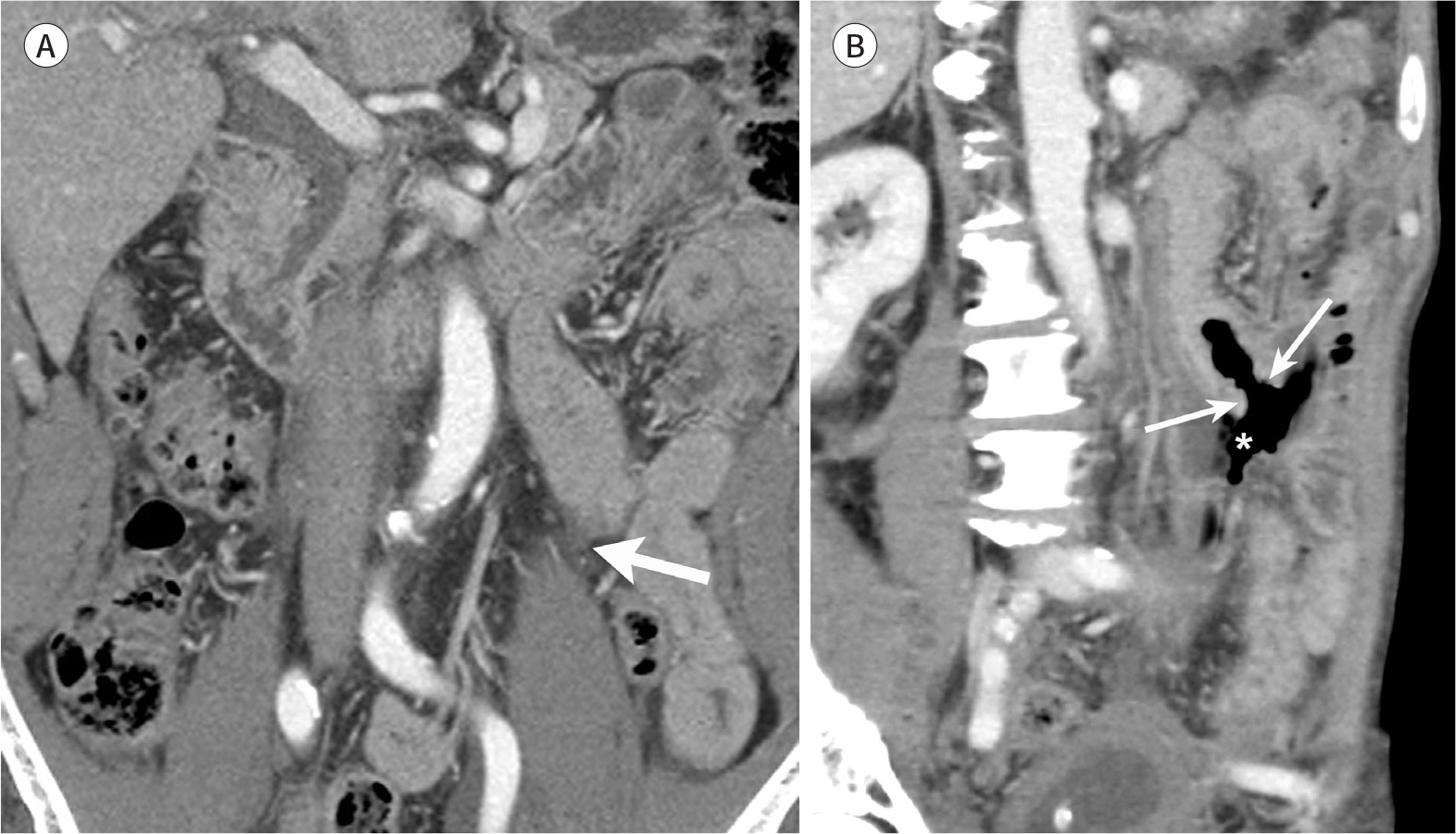
Fig. 20. Delayed bowel perforation in a 62-year-old man after a motor vehicle accident. A. The initial contrast-enhanced CT image shows minimal amount of mesenteric fluid (arrow) without abnormality of the bowel. B. The contrast-enhanced CT image acquired 5 days later shows a newly developed mural defect of the small bowel (arrows) with extraluminal air (asterisk).
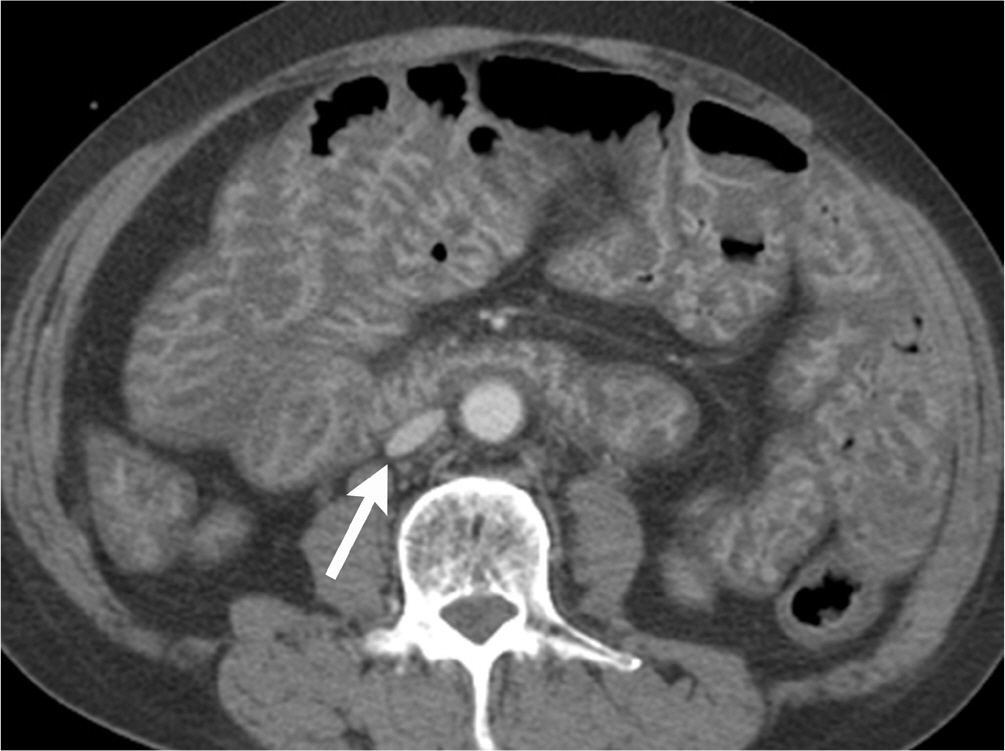
Fig. 21. Hypoperfusion complex in a 61-year-old man after a motor vehicle accident. The contrast-enhanced CT image demonstrates hyperen-hancement of the small bowel mucosa, consistent with a shock bowel. Flattening of the inferior vena cava (arrow) is also seen.
Reference
-
References
1. Hughes TM, Elton C. The pathophysiology and management of bowel and mesenteric injuries due to blunt trauma. Injury. 2002; 33:295–302.
Article2. Soto JA, Anderson SW. Multidetector CT of blunt abdominal trauma.Radiology. 2012; 265:678–693.3. Rieger M, Sparr H, Esterhammer R, Fink C, Bale R, Czermak B, et al. Modern CT diagnosis of acute thoracic and abdominal trauma. Anaesthesist. 2002; 51:835–842.4. Hilbert P, Zur Nieden K, Hofmann GO, Hoeller I, Koch R, Stuttmann R. New aspects in the emergency room management of critically injured patients: a multislice CT-oriented care algorithm.Injury. 2007; 38:552–558.5. Hajibandeh S, Hajibandeh S. Systematic review: effect of whole-body computed tomography on mortality in trauma patients.J Inj Violence Res. 2015; 7:64–74.6. Fanucci E, Fiaschetti V, Rotili A, Floris R, Simonetti G. Whole body 16-row multislice CT in emergency room: effects of different protocols on scanning time, image quality and radiation exposure. Emerg Radiol. 2007; 13:251–257.
Article7. Boscak AR, Shanmuganathan K, Mirvis SE, Fleiter TR, Miller LA, Sliker CW, et al. Optimizing trauma multidetector CT protocol for blunt splenic injury: need for arterial and portal venous phase scans.Radiology. 2013; 268:79–88.8. Leung V, Sastry A, Woo TD, Jones HR. Implementation of a split-bolus single-pass CT protocol at a UK major trauma centre to reduce excess radiation dose in trauma pan-CT.Clin Radiol. 2015; 70:1110–1115.9. Huber-Wagner S, Lefering R, Qvick LM, Körner M, Kay MV, Pfeifer KJ, et al. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study.Lancet. 2009; 373:1455–1461.10. Brink M, De Lange F, Oostveen LJ, Dekker HM, Kool DR, Deunk J, et al. Arm raising at exposure-controlled multidetector trauma CT of thoracoabdominal region: higher image quality, lower radiation dose.Radiology. 2008; 249:661–670.11. Federle MP, Goldberg HI, Kaiser JA, Moss AA, Jeffrey RB Jr, Mall JC. Evaluation of abdominal trauma by computed tomography.Radiology. 1981; 138:637–644.12. Miller LA, Shanmuganathan K. Multidetector CT evaluation of abdominal trauma.Radiol Clin North Am. 2005; 43:1079–1095.13. Shanmuganathan K, Mirvis SE, Sover ER. Value of contrast-enhanced CT in detecting active hemorrhage in patients with blunt abdominal or pelvic trauma. AJR Am J Roentgenol. 1993; 161:65–69.
Article14. Orwig D, Federle MP. Localized clotted blood as evidence of visceral trauma on CT: the sentinel clot sign.AJR Am J Roentgenol. 1989; 153:747–749.15. Livingston DH, Lavery RF, Passannante MR, Skurnick JH, Baker S, Fabian TC, et al. Free fluid on abdominal computed tomography without solid organ injury after blunt abdominal injury does not mandate celiotomy. Am J Surg. 2001; 182:6–9.
Article16. Harris HW, Morabito DJ, Mackersie RC, Halvorsen RA, Schecter WP. Leukocytosis and free fluid are important indicators of isolated intestinal injury after blunt trauma.J Trauma. 1999; 46:656–659.17. Matthes G, Stengel D, Seifert J, Rademacher G, Mutze S, Ekkernkamp A. Blunt liver injuries in polytrauma: results from a cohort study with the regular use of whole-body helical computed tomography. World J Surg. 2003; 27:1124–1130.
Article18. Shuman WP. CT of blunt abdominal trauma in adults.Radiology. 1997; 205:297–306.19. Shanmuganathan K, Mirvis SE. CT scan evaluation of blunt hepatic trauma.Radiol Clin North Am. 1998; 36:399–411.20. Yoon W, Jeong YY, Kim JK, Seo JJ, Lim HS, Shin SS, et al. CT in blunt liver trauma. Radiographics. 2005; 25:87–104.
Article21. Miele V, Andreoli C, De Cicco ML, Adami L, David V. Hemoretroperitoneum associated with liver bare area injuries: CT evaluation.Eur Radiol. 2002; 12:765–769.22. Graves JA, Hanna TN, Herr KD. Pearls and pitfalls of hepatobiliary and splenic trauma: what every trauma radiologist needs to know. Emerg Radiol. 2017; 24:557–568.
Article23. Yu J, Fulcher AS, Turner MA, Halvorsen RA. Multidetector computed tomography of blunt hepatic and splenic trauma: pearls and pitfalls.Semin Roentgenol. 2012; 47:352–361.24. Romano L, Giovine S, Guidi G, Tortora G, Cinque T, Romano S. Hepatic trauma: CT findings and considerations based on our experience in emergency diagnostic imaging.Eur J Radiol. 2004; 50:59–66.25. Baghdanian AH, Armetta AS, Baghdanian AA, LeBedis CA, Anderson SW, Soto JA. CT of major vascular injury in blunt abdominopelvic trauma.Rad/iiographics. 2016; 36:872–890.26. Willmann JK, Roos JE, Platz A, Pfammatter T, Hilfiker PR, Marincek B, et al. Multidetector CT: detection of active hemorrhage in patients with blunt abdominal trauma. AJR Am J Roentgenol. 2002; 179:437–444.
Article27. Nguyen CT, Saksobhavivat N, Shanmuganathan K, Steenburg SD, Moeslein FM, Mirvis SE, et al. MDCT diagnosis of posttraumatic hepatic arterio-portal fistulas.Emerg Radiol. 2013; 20:225–232.28. Hatten MT, Hamrick-Turner JE. Segmental hepatic necrosis after blunt abdominal trauma: CT findings.AJR Am J Roentgenol. 1996; 167:769–770.29. Poletti PA, Mirvis SE, Shanmuganathan K, Killeen KL, Coldwell D. CT criteria for management of blunt liver trauma: correlation with angiographic and surgical findings. Radiology. 2000; 216:418–427.
Article30. LeBedis CA, Anderson SW, Mercier G, Kussman S, Coleman SL, Golden L, et al. The utility of CT for predicting bile leaks in hepatic trauma.Emerg Radiol. 2015; 22:101–107.31. Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. Organ injury scaling: spleen and liver (1994 revision).J Trauma. 1995; 38:323–324.32. Coccolini F, Catena F, Moore EE, Ivatury R, Biffl W, Peitzman A, et al. WSES classification and guidelines for liver trauma.World J Emerg Surg. 2016; 11:50.33. Harbrecht BG, Zenati MS, Ochoa JB, Puyana JC, Alarcon LH, Peitzman AB. Evaluation of a 15-year experience with splenic injuries in a state trauma system.Surgery. 2007; 141:229–238.34. Pimpl W, Dapunt O, Kaindl H, Thalhamer J. Incidence of septic and thromboembolic-related deaths after splenectomy in adults.Br J Surg. 1989; 76:517–521.35. Schweizer W, Böhlen L, Dennison A, Blumgart LH. Prospective study in adults of splenic preservation after traumatic rupture. Br J Surg. 1992; 79:1330–1333.
Article36. Dachman AH, Ros PR, Murari PJ, Olmsted WW, Lichtenstein JE. Nonparasitic splenic cysts: a report of 52 cases with radiologic-pathologic correlation. AJR Am J Roentgenol. 1986; 147:537–542.
Article37. Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD, et al. Blunt splenic injury in adults: multiinstitutional study of the Eastern association for the surgery of trauma. J Trauma. 2000; 49:177–187. ; discussion 187–189.
Article38. Marmery H, Shanmuganathan K, Alexander MT, Mirvis SE. Optimization of selection for nonoperative management of blunt splenic injury: comparison of MDCT grading systems. AJR Am J Roentgenol. 2007; 189:1421–1427.
Article39. Saksobhavivat N, Shanmuganathan K, Chen HH, DuBose JJ, Richard H, Khan MA, et al. Blunt splenic injury: use of a multidetector CT-based splenic injury grading system and clinical parameters for triage of patients at admission.Radiology. 2015; 274:702–711.40. Cirillo RL Jr, Koniaris LG. Detecting blunt pancreatic injuries.J Gastrointest Surg. 2002; 6:587–598.41. Gupta A, Stuhlfaut JW, Fleming KW, Lucey BC, Soto JA. Blunt trauma of the pancreas and biliary tract: a multimodality imaging approach to diagnosis.Radiographics. 2004; 24:1381–1395.42. Bradley EL 3rd, Young PR Jr, Chang MC, Allen JE, Baker CC, Meredith W, et al. Diagnosis and initial management of blunt pancreatic trauma: guidelines from a multiinstitutional review.Ann Surg. 1998; 227:861–869.43. Wong YC, Wang LJ, Lin BC, Chen CJ, Lim KE, Chen RJ. CT grading of blunt pancreatic injuries: prediction of ductal disruption and surgical correlation.J Comput Assist Tomogr. 1997; 21:246–250.44. Brestas PS, Karakyklas D, Gardelis J, Tsouroulas M, Drossos C. Sequential CT evaluation of isolated nonpenetrating pancreatic trauma.JOP. 2006; 7:51–55.45. Wong YC, Wang LJ, Fang JF, Lin BC, Ng CJ, Chen RJ. Multidetector-row computed tomography (CT) of blunt pancreatic injuries: can contrast-enhanced multiphasic CT detect pancreatic duct injuries?J Trauma. 2008; 64:666–672.46. Rekhi S, Anderson SW, Rhea JT, Soto JA. Imaging of blunt pancreatic trauma. Emerg Radiol. 2010; 17:13–19.
Article47. Menegaux F, Trésallet C, Gosgnach M, Nguyen-Thanh Q, Langeron O, Riou B. Diagnosis of bowel and mesenteric injuries in blunt abdominal trauma: a prospective study.Am J Emerg Med. 2006; 24:19–24.48. Atri M, Hanson JM, Grinblat L, Brofman N, Chughtai T, Tomlinson G. Surgically important bowel and/or mesenteric injury in blunt trauma: accuracy of multidetector CT for evaluation. Radiology. 2008; 249:524–533.
Article49. Hawkins AE, Mirvis SE. Evaluation of bowel and mesenteric injury: role of multidetector CT. Abdom Imaging. 2003; 28:505–514.
Article50. Brody JM, Leighton DB, Murphy BL, Abbott GF, Vaccaro JP, Jagminas L, et al. CT of blunt trauma bowel and mesenteric injury: typical findings and pitfalls in diagnosis.Rad/iiographics. 2000; 20:1525–1536. ;discussion 1536–1537.51. Furukawa A, Sakoda M, Yamasaki M, Kono N, Tanaka T, Nitta N, et al. Gastrointestinal tract perforation: CT diagnosis of presence, site, and cause.Abdom Imaging. 2005; 30:524–534.52. Rizzo MJ, Federle MP, Griffiths BG. Bowel and mesenteric injury following blunt abdominal trauma: evaluation with CT. Radiology. 1989; 173:143–148.
Article53. Hanks PW, Brody JM. Blunt injury to mesentery and small bowel: CT evaluation.Radiol Clin North Am. 2003; 41:1171–1182.54. Cho HS, Woo JY, Hong HS, Park MH, Ha HI, Yang I, et al. Multidetector CT findings of bowel transection in blunt abdominal trauma. Korean J Radiol. 2013; 14:607–615.
Article55. Brofman N, Atri M, Hanson JM, Grinblat L, Chughtai T, Brenneman F. Evaluation of bowel and mesenteric blunt trauma with multidetector CT.Radiographics. 2006; 26:1119–1131.56. Evrimler S, Okumuser I, Delibas D. Delayed small bowel perforation with findings of severe ischemia following blunt abdominal trauma. Pol J Radiol. 2017; 82:271–274.
Article57. Subramanian V, Raju RS, Vyas FL, Joseph P, Sitaram V. Delayed jejunal perforation following blunt abdominal trauma.Ann R Coll Surg Engl. 2010; 92:W23–W24.58. Tarrant AM, Ryan MF, Hamilton PA, Benjaminov O. A pictorial review of hypovolaemic shock in adults.Br J Radiol. 2008; 81:252–257.59. Lubner M, Demertzis J, Lee JY, Appleton CM, Bhalla S, Menias CO. CT evaluation of shock viscera: a pictorial review.Emerg Rad/iiol. 2008; 15:1–11.60. Wiesner W, Khurana B, Ji H, Ros PR. CT of acute bowel ischemia. Radiology. 2003; 226:635–650.
Article61. Shanmuganathan K, Mirvis SE, Amoroso M. Periportal low density on CT in patients with blunt trauma: association with elevated venous pressure. AJR Am J Roentgenol. 1993; 160:279–283.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multidetector CT Findings of Bowel Transection in Blunt Abdominal Trauma
- Duodenal Injury after Blunt Abdominal Trauma: Report of Two Cases
- The Efficacy of Emergency Ultrasonography in Blunt Abdominal Trauma
- Multidetector CT Findings of Solid Organ Injury Based on 2018 Updated American Association for the Surgery of Trauma Organ Injury Scaling System
- Traumatic Abdominal Wall Hernia: A Case Report
