Yonsei Med J.
2012 Sep;53(5):992-998.
Analysis of Clinical Feature and Management of Laryngeal Fracture: Recent 22 Case Review
- Affiliations
-
- 1Department of Otorhinolaryngology, Gyeongsang National University, Jinju, Korea. lesaby@hanmail.net
- 2Institute of Health Sciences, Gyeongsang National University, Jinju, Korea.
- 3Department of Otolaryngology, Thyroid/Head & Neck Cancer Center of The Dongnam Institute of Radiological & Medical Sciences (DIRAMS), Busan, Korea.
Abstract
- PURPOSE
Laryngeal fracture is rare, but complications are frequent and severe. Controversy still exists in regards to its proper management. The aim of this study was to present the clinical findings and management of laryngeal fracture in Korea.
MATERIALS AND METHODS
We analyzed the medical records of 22 patients with laryngeal fracture at a tertiary care trauma center from 2000 to 2010 retrospectively.
RESULTS
In total, 22 patients (19 men and 3 woman) presented with laryngeal fractures caused by blunt (n=13) or penetrating (n=9) injury. Pain (68.1%), odynophagia (68.1%), hoarseness (18.1%), hemoptysis (13.6%), and subcutaneous emphysema (9%) were the common presenting symptoms and noncomminuted fracture was common. High velocity blunt trauma (mostly traffic accidents) patients had more extensive injury and poor voice outcomes. Penetrating trauma patients due to physical assault or suicide attempt demonstrated more frequently injuries on the left side.
CONCLUSION
In driver-caused traffic accidents, where injuries in a wide area within the larynx occurred, poor voice results were seen, and these injuries required aggressive treatment. When endotracheal intubation was performed at experienced emergency centers with fiberoptic laryngoscopes, airway management was safely achieved. In addition, if the fractured laryngeal framework was corrected at appropriate times, voice results were good.
MeSH Terms
Figure
-

Fig. 1 Severity of laryngeal injury (Schaefer Fuhrman's classification). LT, laryngo tracheal.
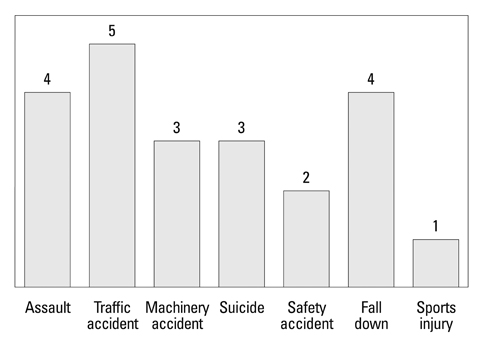
Fig. 2 Causes of laryngeal fracture.

Fig. 3 Subsite of injury in laryngeal fracture.

Fig. 4 Severity of laryngeal fracture due to driver-caused TAs and non-driver-caused TAs. TA, traffic accident.

Fig. 5 Characteristic features of penetrating injury with laryngeal fracture.

Fig. 6 Operating management of laryngeal fracture. ORIF, open reduction & internal fixation.
Reference
-
1. Schaefer SD. The acute management of external laryngeal trauma. A 27-year experience. Arch Otolaryngol Head Neck Surg. 1992. 118:598–604.
Article2. Gussack GS, Jurkovich GJ, Luterman A. Laryngotracheal trauma: a protocol approach to a rare injury. Laryngoscope. 1986. 96:660–665.3. Jalisi S, Zoccoli M. Management of laryngeal fractures--a 10-year experience. J Voice. 2011. 25:473–479.
Article4. Bent JP 3rd, Silver JR, Porubsky ES. Acute laryngeal trauma: a review of 77 patients. Otolaryngol Head Neck Surg. 1993. 109(3 Pt 1):441–449.
Article5. Minard G, Kudsk KA, Croce MA, Butts JA, Cicala RS, Fabian TC. Laryngotracheal trauma. Am Surg. 1992. 58:181–187.6. Hwang SY, Yeak SC. Management dilemmas in laryngeal trauma. J Laryngol Otol. 2004. 118:325–328.
Article7. Butler AP, Wood BP, O'Rourke AK, Porubsky ES. Acute external laryngeal trauma: experience with 112 patients. Ann Otol Rhinol Laryngol. 2005. 114:361–368.
Article8. Eliachar I. Management of acute laryngeal trauma. Acta Otorhinolaryngol Belg. 1996. 50:151–158.9. Fuhrman GM, Stieg FH 3rd, Buerk CA. Blunt laryngeal trauma: classification and management protocol. J Trauma. 1990. 30:87–92.10. Jewett BS, Shockley WW, Rutledge R. External laryngeal trauma analysis of 392 patients. Arch Otolaryngol Head Neck Surg. 1999. 125:877–880.
Article11. Grewal H, Rao PM, Mukerji S, Ivatury RR. Management of penetrating laryngotracheal injuries. Head Neck. 1995. 17:494–502.
Article12. Lee WT, Eliashar R, Eliachar I. Acute external laryngotracheal trauma: diagnosis and management. Ear Nose Throat J. 2006. 85:179–184.
Article13. Irish JC, Hekkenberg R, Gullane PJ, Brown DH, Rotstein LE, Neligan P, et al. Penetrating and blunt neck trauma: 10-year review of a Canadian experience. Can J Surg. 1997. 40:33–38.14. Hanft K, Posternack C, Astor F, Attarian D. Diagnosis and management of laryngeal trauma in sports. South Med J. 1996. 89:631–633.
Article15. Vassiliu P, Baker J, Henderson S, Alo K, Velmahos G, Demetriades D. Aerodigestive injuries of the neck. Am Surg. 2001. 67:75–79.16. Hirano M, Kurita S, Terasawa R. Difficulty in high-pitched phonation by laryngeal trauma. Arch Otolaryngol. 1985. 111:59–61.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experience of Laryngeal Tube Insertion in a Patient of Expected Difficult Intubation : A case report
- Recent Advances in Management of Laryngeal Cancer
- Laser surgery for the laryngeal polyps and nodules: narrative review
- Fracture of Laryngeal Mask Airway during General Anesthesia
- A Case of Horizontal Partial Laryngectomy for Laryngeal Trauma
