Total Ankle Arthroplasty: An Imaging Overview
- Affiliations
-
- 1Department of Diagnostic Radiology, Eulji Hospital, Eulji University, Seoul 01830, Korea. mdcys0128@hanmail.net
- 2Department of Radiology and Imaging, Hospital for Special Surgery, New York, NY 10021, USA.
- 3Department of Orthopaedic Surgery, Eulji Hospital, Eulji University, Seoul 01830, Korea.
- KMID: 2451415
- DOI: http://doi.org/10.3348/kjr.2016.17.3.413
Abstract
- With advances in implant technology, total ankle arthroplasty (TAA) has become an increasingly popular alternative to arthrodesis for the management of end-stage ankle arthritis. However, reports in the literature do not focus on the imaging features of TAA. Through a literature review, we demonstrate basic design features of the current ankle arthroplasty system, and the normal and abnormal postoperative imaging features associated with such devices. Pre- and postoperative evaluations of ankle arthroplasty mainly include radiography; in addition, computed tomography and magnetic resonance imaging provide further characterization of imaging abnormalities. Familiarization with multimodal imaging features of frequent procedural complications at various postoperative intervals is important in radiological practice.
Keyword
MeSH Terms
Figure
-
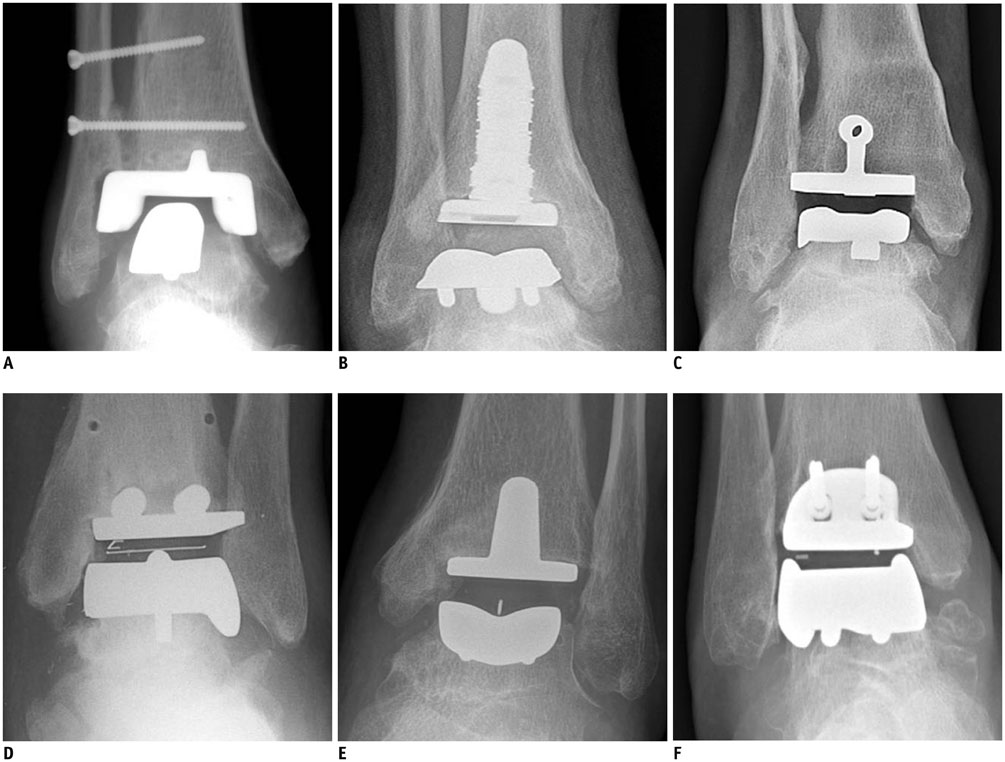
Fig. 1 Total ankle arthroplasty devices. A. Agility (DePuy, Warsaw, IN, USA), semi-constrained, two-component prosthesis. Fusion of distal tibiofibular syndesmosis is desired to stabilize tibial component. B. INBONE (Wright Medical, Arlington, TN, USA), non-constrained, tibial intramedullary modular component that facilitates better fixation in poor tibial bone. C. Salto Talaris (Tornier, Saint Ismier, France), with third-generation cementless meniscal-bearing designs and asymmetric medial and lateral curvatures of talar component that allow inversion and eversion. D. STAR (Waldermar Link, Hamburg, Germany) has two anchorage bars on tibial platform that enhance fixation to tibial bone. E. Mobility (DePuy International, Leeds, UK). Tibial stem and deep sulcus of talar component accommodate matching polyethylene surface, allowing inversion and eversion motions. F. HINTEGRA (Newdeal SA, Lyon, France), unconstrained, three-component system with screw fixation at talar facets and flat tibial cutting (minimize tibial cutting) is not approved by US Food and Drug Administration.
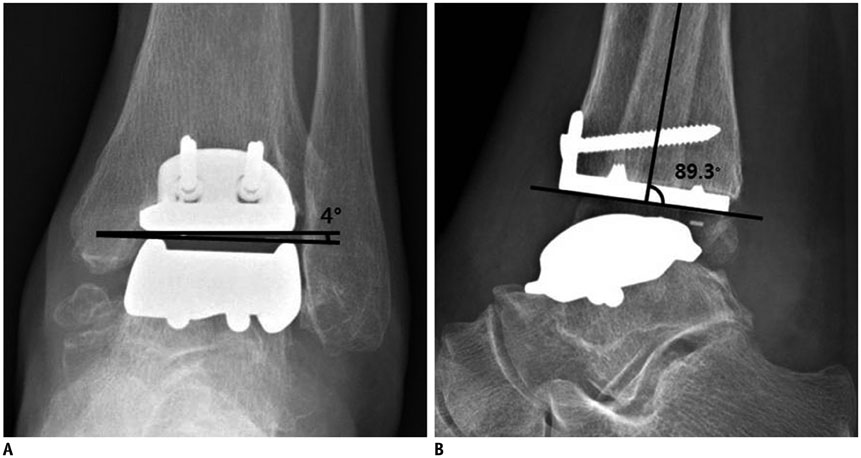
Fig. 2 Normal appearance of total ankle arthroplasty (TAA) as seen on radiography. Weight-bearing anteroposterior (A) and lateral (B) radiographs of HINTEGRA TAA show normal appearance. Tibial-talar angle (A) and anterior distal tibial angle (B) are within their normal ranges (< 10° and 89 ± 3°, respectively).

Fig. 3 Normal appearance of total ankle arthroplasty (TAA) as seen on computed tomography. Coronal (A) and sagittal (B) computed tomographic images (140 kVp with rotation time of 0.6 seconds and collimation of 20 mm using gemstone spectral imaging, 2-mm thickness) show normal appearance of Mobility TAA.

Fig. 4 Normal appearance of total ankle arthroplasty (TAA) as seen on magnetic resonance imaging. Sagittal proton-density-weighted (A) and multi-acquisition with variable resonance image combination inversion recovery (B) magnetic resonance images of INBONE TAA with corresponding ankle lateral radiograph (C).
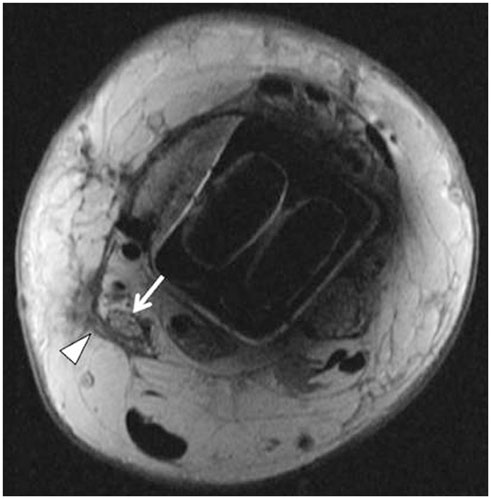
Fig. 5 45-year-old woman with posterior ankle pain and tibial neuroma. Axial proton-density-weighted magnetic resonance image shows neuroma of posterior tibial nerve (arrow) with swelling of nerve fascicles. Thickening of overlying flexor retinaculum (arrowhead) is seen.

Fig. 6 66-year-old man with loosening around tibial component. Patient underwent total ankle arthroplasty several years ago and had global ankle pain. Loosening (arrows) is seen on anteroposterior radiograph (A). Coronal multi-acquisition with variable resonance image combination proton-density-weighted magnetic resonance image (B) shows circumferential loosening (arrows) around tibial component.

Fig. 7 66-year-old woman with particle disease with periprosthetic osteolysis and tibial subsidence. Ankle radiograph (A) and coronal computed tomographic image (B) show cystic soft tissue mass (arrow) communicating with pseudocapsule, and periprosthetic osteolysis (open arrows) around tibial/talar trays with tibial subsidence.
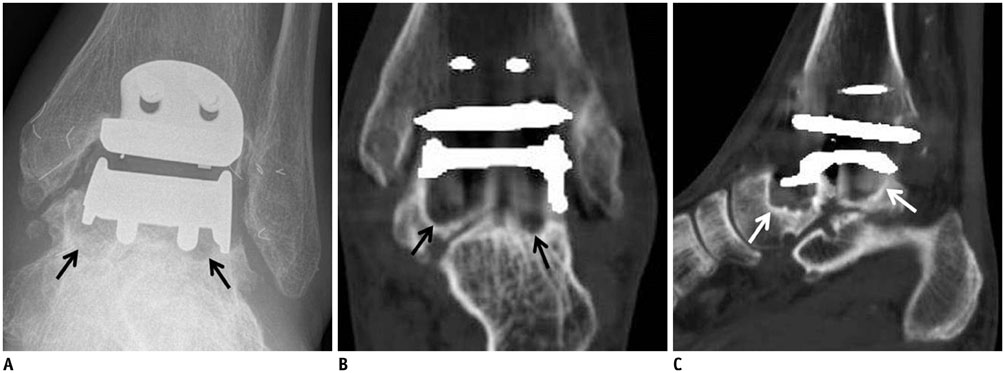
Fig. 8 77-year-old man with periprosthetic osteolysis of talus. Ankle anteroposterior radiograph (A), and coronal (B) and sagittal (C) computed tomographic images show osteolysis (arrows) at inferior aspect of talar tray.
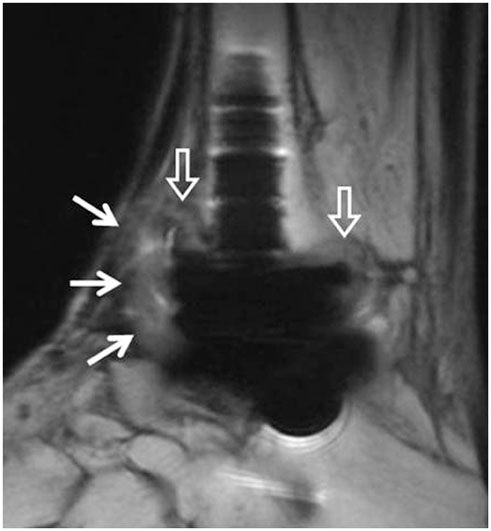
Fig. 9 82-year-old man with polymeric synovitis and tibial osteolysis. Sagittal multi-acquisition with variable resonance image combination proton-density-weighted magnetic resonance image shows bulky polymeric synovitis (arrows) with tibial resorption and osteolysis (open arrows).

Fig. 10 57-year-old man with chronic osteomyelitis and soft tissue infection. Sagittal computed tomographic image shows chronic osteomyelitis with antibiotic beads insertion (arrow) at anterior distal tibial metaphysis. Diffuse subcutaneous tissue swelling is also observed.

Fig. 11 55-year-old woman with aggravated rheumatoid arthritis and distal syndesmosis instability. Patient had underlying rheumatoid arthritis. Coronal computed tomographic image shows newly developed multifocal erosions (arrows) at distal tibia and fibula. Distal tibiofibular clear space is widened.

Fig. 12 71-year-old woman with talar subsidence. Talar subsidence is seen on postoperative ankle anteroposterior radiograph (A). Angular change of more than 5° in measure angle of either component suggests component migration or subsidence. Revision of total ankle arthroplasty is shown, with corrected tibial-talar angle (B).
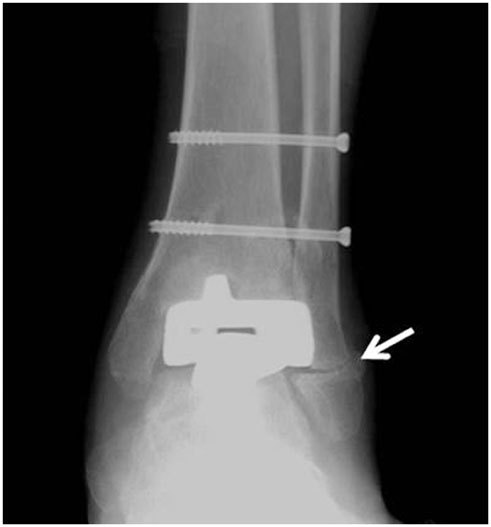
Fig. 13 51-year-old woman with postoperative lateral malleolar fracture. Anteroposterior radiograph acquired 4 months after total ankle arthroplasty shows lateral malleolar fracture (arrow).

Fig. 14 67-year-old woman with postoperative talar fracture. Ankle anteroposterior radiograph acquired 5 months after total ankle arthroplasty shows talar fracture (arrows). Reduction and internal fixation for talar fracture was conducted.
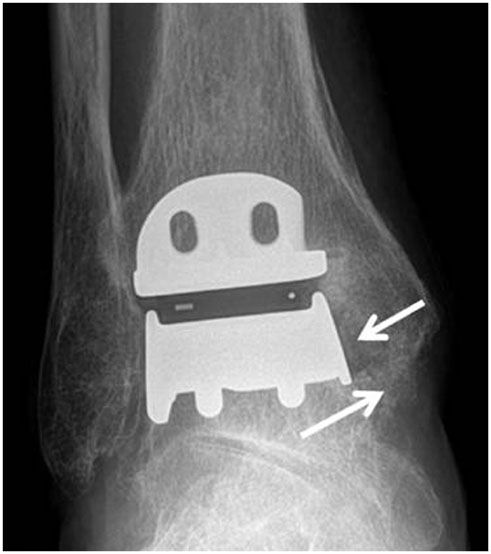
Fig. 15 63-year-old man with medial impingement. Ankle anteroposterior radiograph shows narrowing of medial gutter caused by bony overgrowth (arrows) at inferior tip of medial malleolus and medial talar neck.
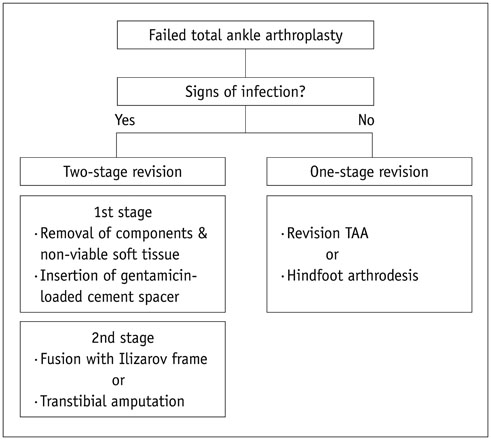
Fig. 16 Management of failed total ankle arthroplasty (TAA) according to presence of infection.
Reference
-
1. Park JS, Mroczek KJ. Total ankle arthroplasty. Bull NYU Hosp Jt Dis. 2011; 69:27–35.2. Bestic JM, Peterson JJ, DeOrio JK, Bancroft LW, Berquist TH, Kransdorf MJ. Postoperative evaluation of the total ankle arthroplasty. AJR Am J Roentgenol. 2008; 190:1112–1123.3. Gougoulias NE, Khanna A, Maffulli N. History and evolution in total ankle arthroplasty. Br Med Bull. 2009; 89:111–151.4. Brunner S, Knupp M, Hintermann B. Total ankle replacement for the valgus unstable osteoarthritic ankle. Tech Foot Ankle Surg. 2010; 9:165–174.5. Easley ME, Adams SB Jr, Hembree WC, DeOrio JK. Results of total ankle arthroplasty. J Bone Joint Surg Am. 2011; 93:1455–1468.6. Lee AY, Ha AS, Petscavage JM, Chew FS. Total ankle arthroplasty: a radiographic outcome study. AJR Am J Roentgenol. 2013; 200:1310–1316.7. Bonasia DE, Dettoni F, Femino JE, Phisitkul P, Germano M, Amendola A. Total ankle replacement: why, when and how? Iowa Orthop J. 2010; 30:119–130.8. Bestic JM, Bancroft LW, Peterson JJ, Kransdorf MJ. Postoperative imaging of the total ankle arthroplasty. Radiol Clin North Am. 2008; 46:1003–1015. v–vi.9. Hintermann B. Ankle osteoarthritis: five take-home points regarding total ankle arthroplasty in the rest of the world. In : 26th Annual Summer Meeting of the American Orthopaedic Foot & Ankle Society; 2010 July 7-10; National Harbor, MD USA.10. Hanna RS, Haddad SL, Lazarus ML. Evaluation of periprosthetic lucency after total ankle arthroplasty: helical CT versus conventional radiography. Foot Ankle Int. 2007; 28:921–926.11. Kohonen Ia, Koivu H, Vahlberg T, Larjava H, Mattila K. Total ankle arthroplasty: optimizing computed tomography imaging protocol. Skeletal Radiol. 2013; 42:1507–1513.12. Lee MJ, Kim S, Lee SA, Song HT, Huh YM, Kim DH, et al. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics. 2007; 27:791–803.13. Higashigaito K, Angst F, Runge VM, Alkadhi H, Donati OF. Metal artifact reduction in pelvic computed tomography with hip prostheses: comparison of virtual monoenergetic extrapolations from dual-energy computed tomography and an iterative metal artifact reduction algorithm in a phantom study. Invest Radiol. 2015; 50:828–834.14. Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics. 2004; 24:1679–1691.15. Hayter CL, Koff MF, Shah P, Koch KM, Miller TT, Potter HG. MRI after arthroplasty: comparison of MAVRIC and conventional fast spin-echo techniques. AJR Am J Roentgenol. 2011; 197:W405–W411.16. Hargreaves BA, Worters PW, Pauly KB, Pauly JM, Koch KM, Gold GE. Metal-induced artifacts in MRI. AJR Am J Roentgenol. 2011; 197:547–555.17. Sofka CM. Postoperative magnetic resonance imaging of the foot and ankle. J Magn Reson Imaging. 2013; 37:556–565.18. Jackson MP, Singh D. Total ankle replacement. Curr Orthop. 2003; 17:292–298.19. Haskell A, Mann RA. Perioperative complication rate of total ankle replacement is reduced by surgeon experience. Foot Ankle Int. 2004; 25:283–289.20. Glazebrook MA, Arsenault K, Dunbar M. Evidence-based classification of complications in total ankle arthroplasty. Foot Ankle Int. 2009; 30:945–949.21. DeOrio JK, Parekh SG. Total Ankle Replacement: An Operative Manual. 2014. Philadelphia: Lippincott Williams and Wilkins;2014. p. 116–122.22. DeOrio JK, Easley ME. Total ankle arthroplasty. Instr Course Lect. 2008; 57:383–413.23. Kopp FJ, Patel MM, Deland JT, O'Malley MJ. Total ankle arthroplasty with the Agility prosthesis: clinical and radiographic evaluation. Foot Ankle Int. 2006; 27:97–103.24. Knecht SI, Estin M, Callaghan JJ, Zimmerman MB, Alliman KJ, Alvine FG, et al. The Agility total ankle arthroplasty Seven to sixteen-year follow-up. J Bone Joint Surg Am. 2004; 86-A:1161–1171.25. Doets HC, Brand R, Nelissen RG. Total ankle arthroplasty in inflammatory joint disease with use of two mobile-bearing designs. J Bone Joint Surg Am. 2006; 88:1272–1284.26. Spirt AA, Assal M, Hansen ST Jr. Complications and failure after total ankle arthroplasty. J Bone Joint Surg Am. 2004; 86-A:1172–1178.27. Kotnis R, Pasapula C, Anwar F, Cooke PH, Sharp RJ. The management of failed ankle replacement. J Bone Joint Surg Br. 2006; 88:1039–1047.
