Pneumoperitoneum after Endoscopic Duodenal Stent Insertion in a Patient with Percutaneous Transhepatic Biliary Drainage and Biliary Stent: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea. smpark@chungbuk.ac.kr
- 2Department of Radiology, Chungbuk National University Hospital, Cheongju, Korea.
- 3Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 2449772
- DOI: http://doi.org/10.5946/ce.2018.128
Abstract
- Early removal of a percutaneous transhepatic biliary drainage (PTBD) tube commonly causes pneumoperitoneum. However, we encountered a patient who developed pneumoperitoneum even with an indwelling PTBD tube. An 84-year-old man was admitted with type III combined duodenal and biliary obstruction secondary to metastatic bladder cancer. A biliary stent was placed using a percutaneous approach, and a duodenal stent was placed endoscopically. A large amount of subphrenic free air was detected after the procedures. Laboratory tests indicated intestinal perforation; however, peritoneal signs were absent. The patient was treated conservatively using an indwelling Levin tube. Seven days later, the massive amount of subphrenic free air disappeared. Follow-up tubography revealed unrestricted bile flow into the small intestine, and the PTBD tube was removed. Prolonged endoscopic procedures in patients with a PTBD tract communicating with the gastrointestinal tract can precipitate pneumoperitoneum. Clinicians should be careful to avoid misdiagnosing this condition as intestinal perforation.
Keyword
MeSH Terms
Figure
-

Fig. 1. Abdominal computed tomography and endoscopic images show type III combined duodenal and biliary obstruction. The distended proximal duodenum (A, arrows), luminal stenosis at the distal common bile duct (B, arrow), the proximal bile duct dilatation (C, arrow), and a normal papilla (D) can be observed.

Fig. 2. Images show radiological and endoscopic intervention for type III combined duodenal and biliary obstruction. (A) Biliary metal stent insertion (arrow) through percutaneous transhepatic biliary drainage (arrow heads) and (B) endoscopic duodenal stent insertion after a guidewire has been advanced deep beyond the stricture (arrow). (C) Endoscopic images show incomplete expansion of the duodenal stent. (D) Abdominal computed tomography shows pneumoperitoneum (arrows) after the endoscopic procedure.
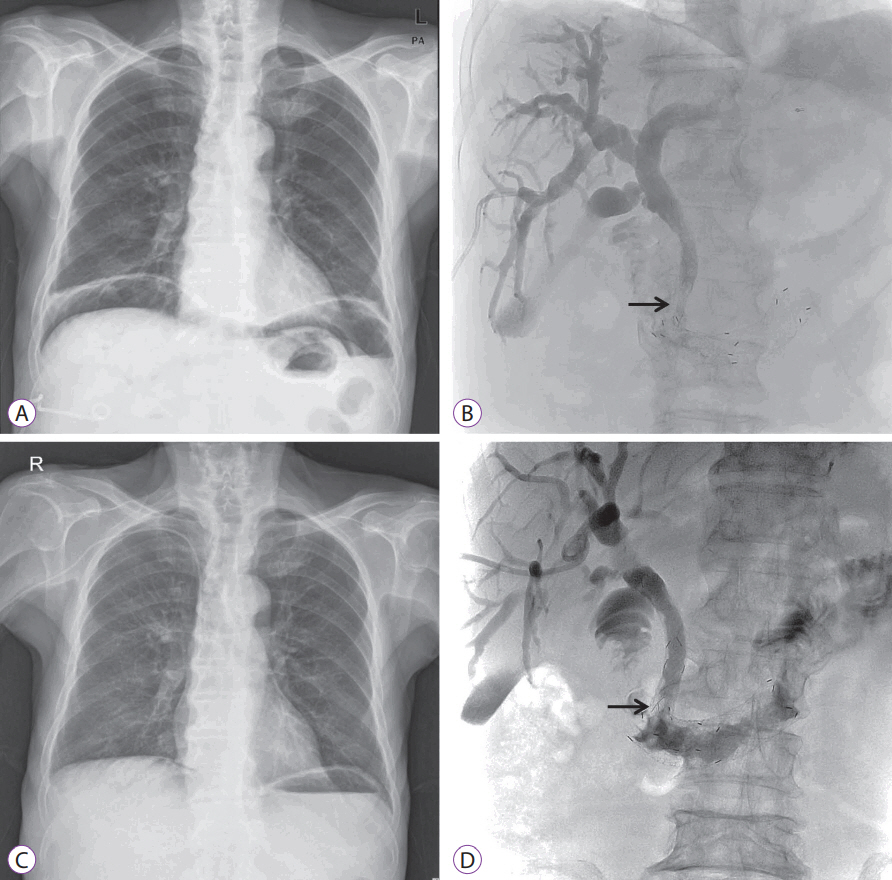
Fig. 3. Abdominal radiography (A and C) and tubography (B and D) images show persistence of subphrenic air (A) with restricted bile flow owing to incomplete expansion of the duodenal stent (B, arrow). Subphrenic air seems to have disappeared (C) following unrestricted drainage of the bile into the intestinal tract after complete expansion of the duodenal stent (D, arrow).
Reference
-
1. Lee JH, Lee DH, Yu JS, Lee SJ, Kwon WC, Kim KW. Pneumoperitoneum caused by transhepatic air leak after metallic biliary stent placement. Cardiovasc Intervent Radiol. 2000; 23:482–484.
Article2. Amonkar SJ, Laasch HU, Valle JW. Pneumoperitoneum following percutaneous biliary intervention: not necessarily a cause for alarm. Cardiovasc Intervent Radiol. 2008; 31:439–443.
Article3. Hui YT, Lam WM, Lam TW, Cheung WC, Sze SF, Wong CT. Benign pneumoperitoneum developed after endoscopic biliary metallic stent placement with the rendezvous procedure. Gastrointest Endosc. 2008; 67:179–180.
Article4. Chuang CH, Chen CY, Tsai HM. Pneumoperitoneum caused by air leakage through the percutaneous puncture tract as a complication of rendezvous technique: a case report. Kaohsiung J Med Sci. 2008; 24:614–617.
Article5. Virgilio E, Chieco PA, Salaj A, et al. Conservative management of pneumoperitonitis after percutaneous transhepatic insertion of metallic biliary stents. Am Surg. 2015; 81:E418–E419.
Article6. Jonnalagadda S, Azar R. Avoiding pneumomediastinum during ERCP after percutaneous transhepatic biliary drainage. Gastrointest Endosc. 2008; 68:809. author reply 809-810.
Article7. Baron TH. Management of simultaneous biliary and duodenal obstruction: the endoscopic perspective. Gut Liver. 2010; 4 Suppl 1:S50–S56.
Article8. Lisle DA, Hunter JC, Pollard CW, Borrowdale RC. Percutaneous gelfoam embolization of chronic enterocutaneous fistulas: report of three cases. Dis Colon Rectum. 2007; 50:251–256.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous transhepatic access to allow per-oral enteric stent insertion for malignant duodenal obstruction following failed endoscopic attempt
- Endoscopic Reintervention for Recurrence of Malignant Biliary Obstruction: Developing the Best Strategy
- Two Double Stents Insertion for Commen Bile Duct and Duodenal Obstruction Caused by Pancreatic Cancer
- Endoscopic Stent Placement in the Palliation of Malignant Biliary Obstruction
- Percutaneous Endoscopic Biliary Stent (PEBS): A case report
