Omental Patching and Purse-String Endosuture Closure after Endoscopic Full-Thickness Resection in Patients with Gastric Gastrointestinal Stromal Tumors
- Affiliations
-
- 1Allama Iqbal Medical College, Lahore, Pakistan. faisalinayat@hotmail.com
- 2Harvard Medical School, Boston, MA, USA.
- 3SUNY Downstate Medical Center, Brooklyn, NY, USA.
- 4Shifa College of Medicine, Islamabad, Pakistan.
- 5Hofstra-Northwell School of Medicine, Hempstead, NY, USA.
- KMID: 2449771
- DOI: http://doi.org/10.5946/ce.2018.116
Abstract
- Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal tract, primarily arising from the stomach. With the widespread utilization of and technical advancements in endoscopy, gastric GISTs are being increasingly detected at an early stage, enabling complete endoscopic resection. Endoscopic full-thickness resection (EFTR) is an advanced technique that has been recognized as a treatment tool for neoplasms in the digestive tract in selected patients. Although a number of methods are available, closing large iatrogenic defects after EFTR can be a concern in clinical practice. If this potential problem is appropriately solved, patients with gastric GISTs would be suitable candidates for resection utilizing this technique. To our knowledge, this is the first study to propose omental patching and purse-string endosuture closure following EFTR as a feasible endoscopic option in patients with gastric GISTs.
Keyword
Figure
-
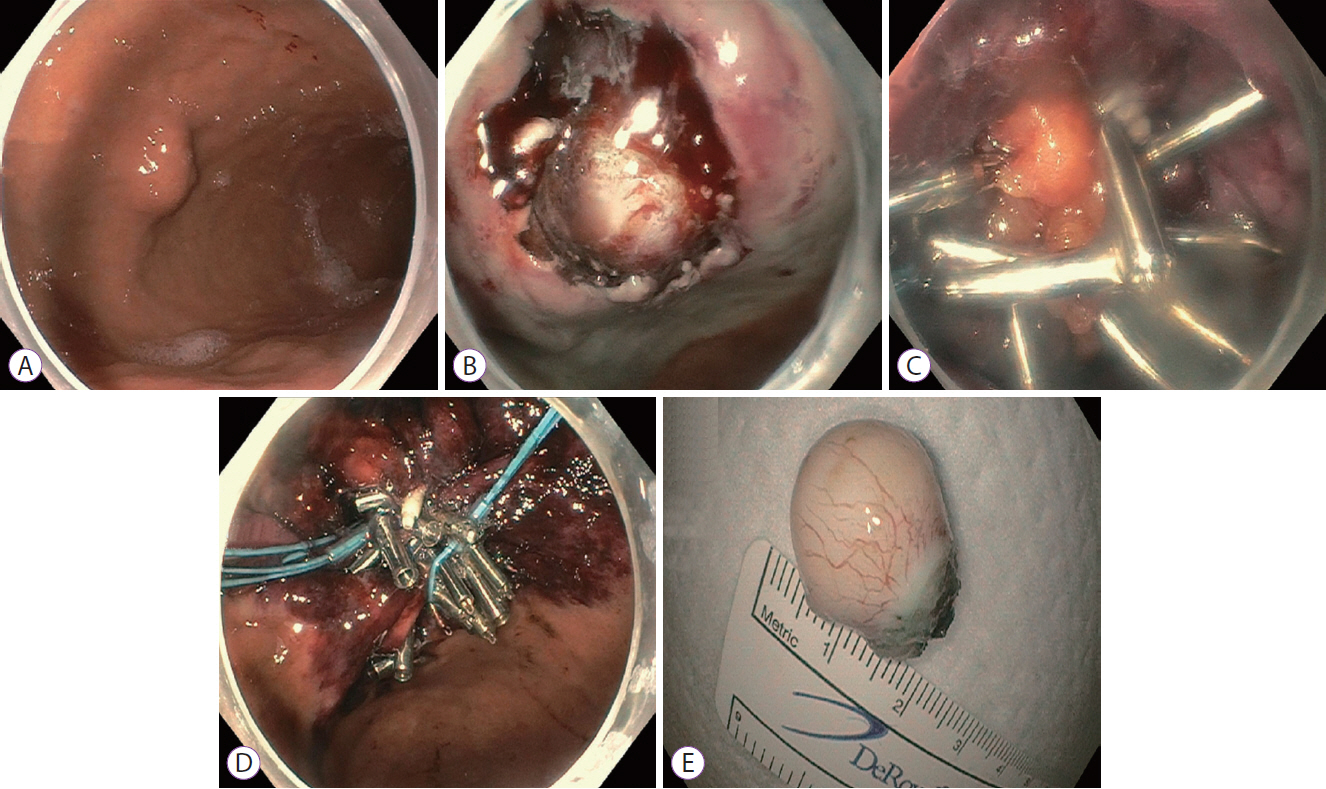
Fig. 1. (A) Esophagogastroduodenoscopy identified an approximately 2-cm round submucosal lesion located in the fundus/proximal body along the greater curvature of the stomach. (B) An iatrogenic full-thickness gastric wall defect was created by the endoscopic full-thickness resection. (C) The defect was successfully closed using omental fat patching. Several hemoclips were deployed to affix the fat plug to the gastric wall. (D) The hemoclips were then joined together by an endoloop. (E) Gross appearance of the resected specimen. A fleshy tan-white mass measuring 22 mm in diameter was resected and sent for pathological examination.
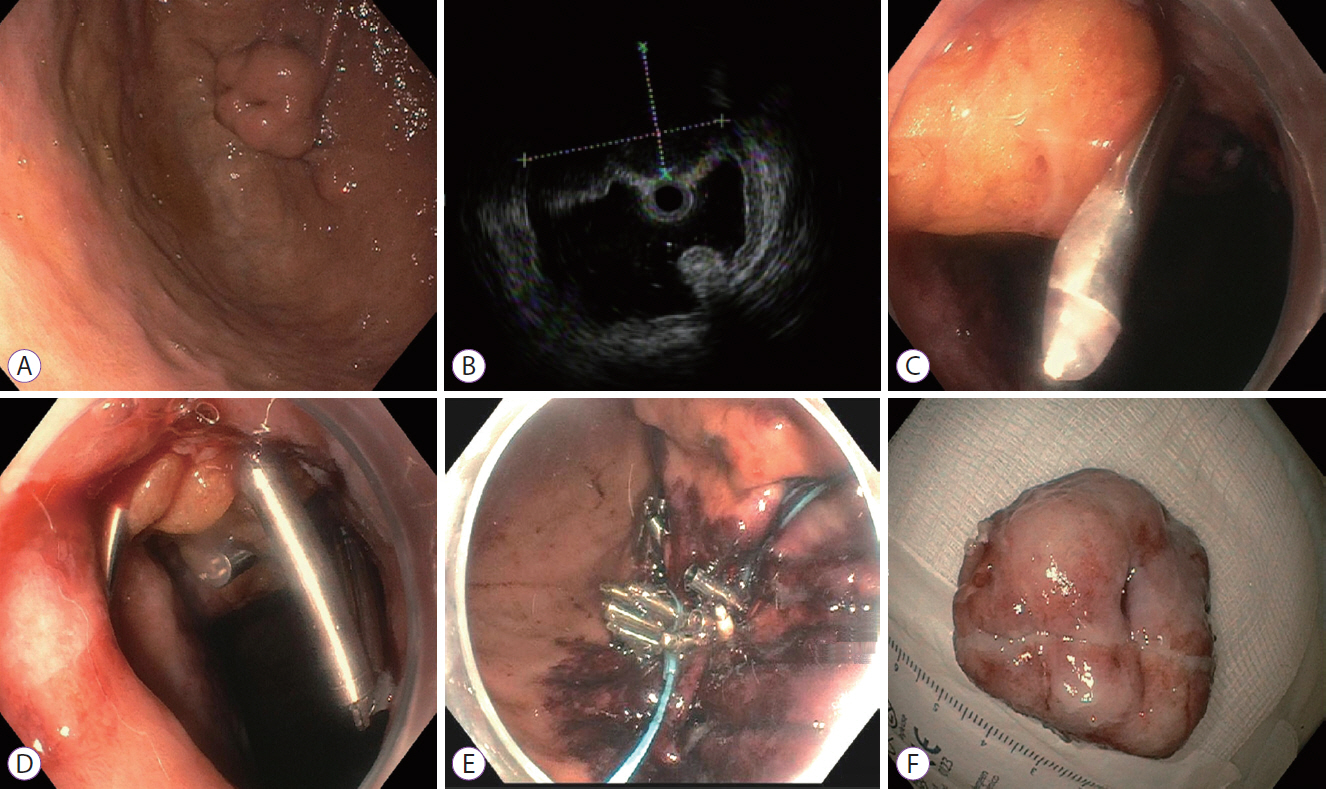
Fig. 2. (A) Esophagogastroduodenoscopy showing an approximately 2.5-cm intramural submucosal lesion in the gastric cardia along the greater curvature. (B) Endoscopic ultrasound image showing an 18.5×13 mm endophytic submucosal lesion originating from the muscularis propria. (C) The omental fat plug was pulled into the gastric lumen in an attempt to close the defect. (D) Multiple hemoclips were deployed to hold the fat plug within the gastric wall. (E) Endosutures were applied in a purse-string fashion around the hemoclips. (F) Gross morphology of the resected specimen. A multinodular mass with 28-mm ulcerations was resected and sent for pathological examination.
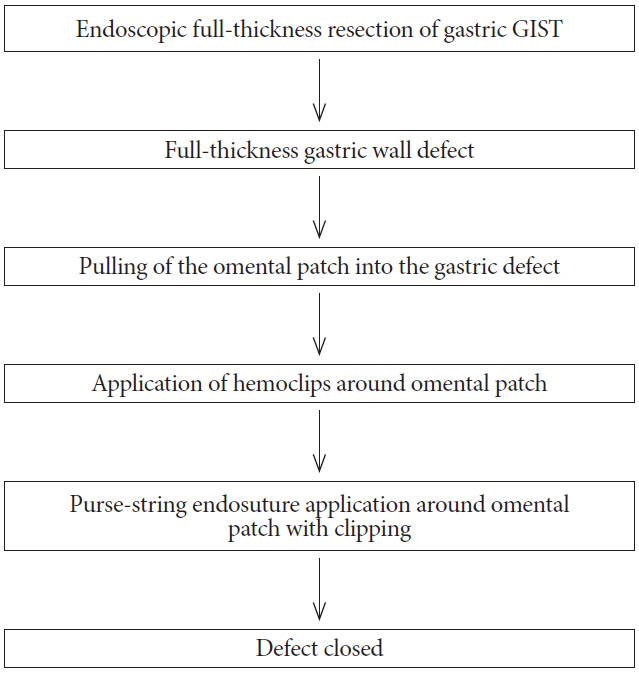
Fig. 3. Flowchart showing the omental patching and purse-string technique for closing endoscopic full-thickness resection-related gastric defects in patients with gastrointestinal stromal tumors (GISTs).
Reference
-
1. Bai J, Wang Y, Guo H, Zhang P, Ling X, Zhao X. Endoscopic resection of small gastrointestinal stromal tumors. Dig Dis Sci. 2010; 55:1950–1954.
Article2. Mori H, Kobara H, Nishiyama N, Masaki T. Current status and future perspectives of endoscopic full-thickness resection. Dig Endosc. 2018; 30 Suppl 1:25–31.
Article3. Backes Y, Kappelle WFW, Berk L, et al. Colorectal endoscopic full-thickness resection using a novel, flat-base over-the-scope clip: a prospective study. Endoscopy. 2017; 49:1092–1097.
Article4. Brigic A, Symons NR, Faiz O, Fraser C, Clark SK, Kennedy RH. A systematic review regarding the feasibility and safety of endoscopic full thickness resection (EFTR) for colonic lesions. Surg Endosc. 2013; 27:3520–3529.
Article5. Raju GS. Endoscopic clip closure of gastrointestinal perforations, fistulae, and leaks. Dig Endosc. 2014; 26 Suppl 1:95–104.
Article6. von Renteln D, Schmidt A, Vassiliou MC, Rudolph HU, Caca K. Endoscopic full-thickness resection and defect closure in the colon. Gastrointest Endosc. 2010; 71:1267–1273.
Article7. Ye LP, Yu Z, Mao XL, Zhu LH, Zhou XB. Endoscopic full-thickness resection with defect closure using clips and an endoloop for gastric subepithelial tumors arising from the muscularis propria. Surg Endosc. 2014; 28:1978–1983.
Article8. Lu J, Jiao T, Li Y, Zheng M, Lu X. Facilitating retroflexed endoscopic full-thickness resection through loop-mediated or rope-mediated countertraction (with videos). Gastrointest Endosc. 2016; 83:223–228.
Article9. Guo J, Liu Z, Sun S, et al. Endoscopic full-thickness resection with defect closure using an over-the-scope clip for gastric subepithelial tumors originating from the muscularis propria. Surg Endosc. 2015; 29:3356–3362.
Article10. Smith D, Roeser M, Naranjo J, Carr JA. The natural history of perforated foregut ulcers after repair by omental patching or primary closure. Eur J Trauma Emerg Surg. 2018; 44:273–277.
Article11. Karanjia ND, Shanahan DJ, Knight MJ. Omental patching of a large perforated duodenal ulcer: a new method. Br J Surg. 1993; 80:65.
Article12. Minami S, Gotoda T, Ono H, Oda I, Hamanaka H. Complete endoscopic closure of gastric perforation induced by endoscopic resection of early gastric cancer using endoclips can prevent surgery (with video). Gastrointest Endosc. 2006; 63:596–601.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Full-Thickness Resection for Gastric Subepithelial Lesions Arising from the Muscularis Propria
- Reconstruction of Large Defects of the Face Utilizing Purse-String Suture
- Natural Orifice Transluminal Endoscopic Surgery and Upper Gastrointestinal Tract
- Endoscopic and Laparoscopic Full-Thickness Resection of Endophytic Gastric Submucosal Tumors Very Close to the Esophagogastric Junction
- Current Techniques for Treating Gastrointestinal Stromal Tumors in the Upper Gastrointestinal Tract
