J Rhinol.
2019 May;26(1):52-55. 10.18787/jr.2019.26.1.52.
Treatment of Facial Neuralgia Developed after Inferior Meatal Antrostomy by Narrowing of the Inlet with Endoscopic Cartilage Graft
- Affiliations
-
- 1Doctor Jin's Premium Nose Clinic, Seoul, Korea. doctorjin@daum.net
- KMID: 2449030
- DOI: http://doi.org/10.18787/jr.2019.26.1.52
Abstract
- Inferior meatal antrostomy (IMA) is a widely performed surgical technique to treat postoperative maxillary mucocele. The method is safe and easy to perform, without major complications compared with other approaches. Facial pain after IMA is a rare clinical entity that can be challenging to diagnose and treat. The authors present an unusual case of acute facial neuralgia triggered by cold air that developed after IMA. The antrostomy was located at the anterior-most part of the inferior meatus, and the inlet size was relatively large compared with the size of the remaining sinus. Surgical narrowing of the antrostomy inlet using endoscopy dramatically reduced the symptoms, and symptom relief was maintained for up to one year after surgery.
Keyword
Figure
-

Fig. 1 OMU CT scan showed small, contracted left maxillary sinus with fibrosis and new bone formation. The antrostomy inlet is relatively large compared to the small sinus.
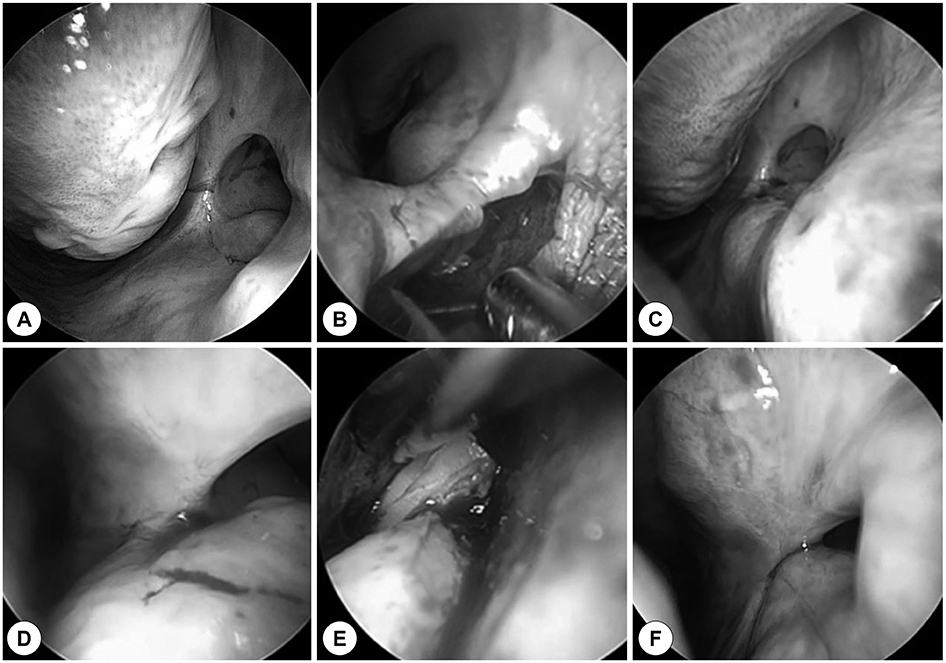
Fig. 2 IMA site reconstruction. A: About 1.0 cm sized, patent antrostomy at the anterior part of the left inferior meatus, B: endoscopic vestibular incision, C, D: dissection of pocket, E: insertion of cartilage chips, F: ostium narrowing after surgery.
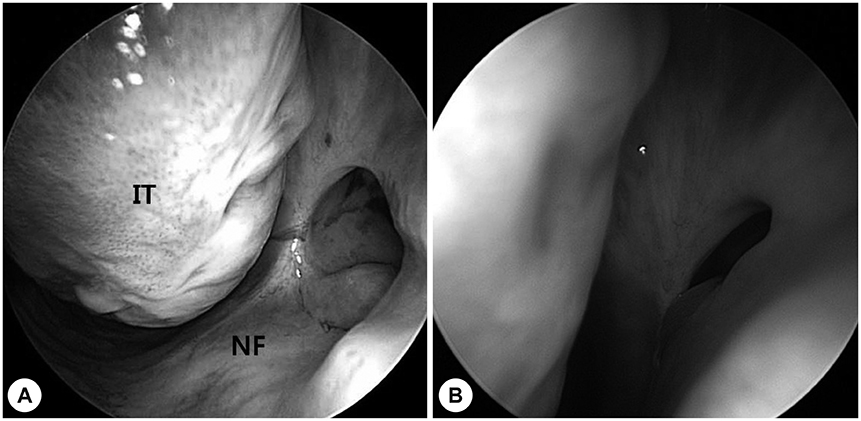
Fig. 3 Pre (A) and postoperative 6 months (B) endoscopic view of the IMA opening. Narrowed antrostomy inlet was well maintained. IT: inferior turbinate, NF: nasal floor
Reference
-
1. Basu MK, Rout PG, Rippin JW, Smith AJ. The post-operative maxillary cyst. Experience with 23 cases. Int J Oral Maxillofac Surg. 1988; 17:282–284.2. Saito T, Ikeda T, Kono Y, Ohtsubo T, Noda I, Saito H. Implications of endoscopic endonasal surgery for the treatment of postoperative maxillary mucoceles. ORL J Otorhinolaryngol Relat Spec. 2000; 62:43–48.
Article3. Huang CC, Chen CW, Lee TJ, Chang PH, Chen YW, Chen YL, et al. Transnasal endoscopic marsupialization of postoperative maxillary mucoceles: middle meatal antrostomy versus inferior meatal antrostomy. Eur Arch Otorhinolaryngol. 2011; 268:1583–1587.
Article4. Lee JY, Baek BJ, Byun JY, Shin JM. Long-term efficacy of inferior meatal antrostomy for treatment of postoperative maxillary mucoceles. Am J Otolaryngol. 2014; 727–730.
Article5. Lund VJ. Fundamental considerations of the design and function of intranasal antrostomies. Rhinology. 1985; 23:231–236.6. Krafft RM. Trigeminal neuralgia. Am Fam Physician. 2008; 77:1291–1296.7. Sharma N, De M, Pracy P. Recurrent facial paresthesia secondary to maxillary antral cyst and dehiscent infraorbital canal: case report. J Laryngol Otol. 2007; 121:e6.8. Hollinshead WH. Anatomy for regeon v.1: the head and neck. New York: Harper & Row;1968.9. Gray HGCM. Anatomy of the human body. Philadelphia, PA: Lea & Febiger;1966.10. Whittet HB. Infraorbital nerve dehiscence: the anatomic cause of maxillary sinus “vacuum headache”? Otolaryngol Head Neck Surg. 1992; 107(1):21–28.
Article11. Mirza S, Richardson H. Otic barotrauma from air travel. J Laryngol Otol. 2005; 119:366–370.
Article12. Falck B, Svanholm H, Aust R, Bäcklund L. The relationship between body posture and pressure in occluded maxillary sinus of man. Rhinology. 1989; 27:161–167.13. Sessle BJ. Peripheral and central mechanisms of orofacial inflammatory pain. Int Rev Neurobiol. 2011; 97:179–206.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long-Term Outcomes of Transnasal Endoscopic Marsupialization through Middle, Inferior Meatal Antrostomy or Extended Middle Meatal Antrostomy in Maxillary Sinus Mucoceles
- Advantage of Middle Meatal Antrostomy in Transnasal Endoscopic Reconstruction of Medial Orbital Blow-out Fracture
- Endoscopic Maxillary Sinus Surgery Using the Microdebrider
- Clinical Characteristics According to the Radiological Classifications of Maxillary Sinus Fungus Ball
- Sinusitis Managment Associated with Maxillary Sinus Augmentation: Case Report
