Intramedullary Blunt K-Wire Fixation for Pediatric Forearm Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. hypark@catholic.ac.kr
- KMID: 2448046
- DOI: http://doi.org/10.12790/ahm.2019.24.2.126
Abstract
- PURPOSE
Intramedullary blunt K-wire fixation was performed for pediatric forearm fractures and we report the clinical results.
METHODS
From January 2014 to December 2017, we retrospectively reviewed 35 patients who underwent surgical treatment for pediatric forearm fractures under 14 years of age. The location of the fracture, pre- and postoperative angulation, and the union time were evaluated using simple radiographs. Patients were evaluated for postoperative immobilization period, postoperative range of motion of the wrist and elbow joints, and postoperative complications.
RESULTS
The mean age of the patients was 8.1 years. The fracture site was the both in 22 cases, the radius in 8 cases, and ulna in 5 cases. The location of fracture was 10 cases in distal diaphysis, 22 cases in mid-shaft, and 3 cases in proximal diaphysis. The mean postoperative immobilization period was 5 weeks and bone union was achieved at 4 weeks. Bony union was obtained in all cases and all cases showed normal range of motion. There were no major complications such as re-fracture, pin fracture, or infection.
CONCLUSION
Intramedullary blunt K-wire fixation for pediatric forearm fractures may be one of the treatment methods that can be considered regardless of the location of the fracture with few complications.
MeSH Terms
Figure
-
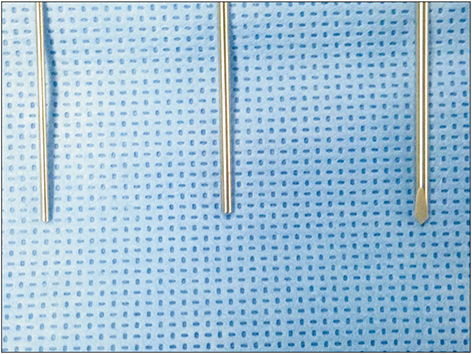
Fig. 1 A 1.1 mm and 1.5 mm K-wires with blunt tip compared to regular K-wire.

Fig. 2 (A) Preoperative simple radiographs showed fracture of the distal radius and ulnar metadiaphyseal junction. (B) Simple radiographs after reduction showed 13 degrees angulation. (C) Intramedullary blunt K-wire fixation was performed and postoperative radiographs showed satisfactory reduction. (D) Postoperative 6 weeks radiographs showed bony union. (E) Postoperative 6 months radiographs after pin removal showed good union.

Fig. 3 (A) Preoperative simple radiographs showed Gustilo–Anderson type I open fracture of radius and ulnar shaft. (B) Intramedullary blunt K-wire fixation was performed and postoperative radiographs showed satisfactory reduction. (C) Postoperative 6 weeks radiographs showed bony union. (D) Postoperative 6 months radiographs after pin removal showed good union.
Reference
-
1. Vopat ML, Kane PM, Christino MA, et al. Treatment of diaphyseal forearm fractures in children. Orthop Rev (Pavia). 2014; 6:5325.
Article2. Price CT. Acceptable alignment of forearm fractures in children: open reduction indications. J Pediatr Orthop. 2010; 30:S82–S84.
Article3. Tarmuzi NA, Abdullah S, Osman Z, Das S. Paediatric forearm fractures: functional outcome of conservative treatment. Bratisl Lek Listy. 2009; 110:563–568.4. Noonan KJ, Price CT. Forearm and distal radius fractures in children. J Am Acad Orthop Surg. 1998; 6:146–156.
Article5. Song BY, Kwak HY, Bae SW, et al. Operative treatment of diaphyseal forearm fracture in children. J Korean Orthop Assoc. 2002; 37:518–524.
Article6. Okoroafor UC, Cannada LK, McGinty JL. Obesity and failure of nonsurgical management of pediatric both-bone forearm fractures. J Hand Surg Am. 2017; 42:711–716.
Article7. Kanellopoulos AD, Yiannakopoulos CK, Soucacos PN. Flexible intramedullary nailing of pediatric unstable forearm fractures. Am J Orthop (Belle Mead NJ). 2005; 34:420–424.8. Kapoor V, Theruvil B, Edwards SE, et al. Flexible intramedullary nailing of displaced diaphyseal forearm fractures in children. Injury. 2005; 36:1221–1225.
Article9. Kim BS, Lee YS, Park SY, Nho JH, Lee SG, Kim YH. Flexible intramedullary nailing of forearm fractures at the distal metadiaphyseal junction in adolescents. Clin Orthop Surg. 2017; 9:101–108.
Article10. Ali AM, Abdelaziz M, El-Lakanney MR. Intramedullary nailing for diaphyseal forearm fractures in children after failed conservative treatment. J Orthop Surg (Hong Kong). 2010; 18:328–331.
Article11. Mahecha-Toro M, Vergara-Amador E, González Ramírez M. Forearm diaphyseal fractures in children: intramedullary Kirschner's wire fixation treatment. Rev Esp Cir Ortop Traumatol. 2018; 62:71–79.
Article12. Kose O, Deniz G, Yanik S, Gungor M, Islam NC. Open intramedullary Kirschner wire versus screw and plate fixation for unstable forearm fractures in children. J Orthop Surg (Hong Kong). 2008; 16:165–169.
Article13. Bombaci H, Guneri B, Caboglu F, Gorgec M. Intramedullary K-wire fixation of pediatric forearm fractures and effects on the wrist. Orthopedics. 2007; 30:866–870.
Article14. Creasman C, Zaleske DJ, Ehrlich MG. Analyzing forearm fractures in children. The more subtle signs of impending problems. Clin Orthop Relat Res. 1984; 40–53.15. Flynn JM, Jones KJ, Garner MR, Goebel J. Eleven years experience in the operative management of pediatric forearm fractures. J Pediatr Orthop. 2010; 30:313–319.
Article16. Battle J, Carmichael KD, Morris RP. Biomechanical comparison of flexible intramedullary nailing versus crossed Kirschner wire fixation in a canine model of pediatric forearm fractures. J Pediatr Orthop B. 2006; 15:370–375.
Article17. Holmes JH 4th, Wiebe DJ, Tataria M, et al. The failure of nonoperative management in pediatric solid organ injury: a multi-institutional experience. J Trauma. 2005; 59:1309–1313.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Transphyseal Intramedullary K-wire Fixation for the Diaphyseal Forearm Fractures in Children
- Percutaneous Transphyseal Intramedullary Kirschner Wire Fixation for Pediatric Diaphyseal Forearm Fractures
- Pediatric Forearm Bone Fractures Treated with Flexible Intramedullary Nail
- Operative Treatment of Diaphyseal Forearm Fracture in Children
- Surgical Treatment of Diaphyseal Fractures of Both Forearm Bones in Adolescents
