The Frequency of Occult Intertrochanteric Fractures among Individuals with Isolated Greater Trochanteric Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, The Catholic University of Korea, Bucheon St. Mary's Hospital, Bucheon, Korea. keeleehip@gmail.com
- KMID: 2448038
- DOI: http://doi.org/10.5371/hp.2019.31.1.23
Abstract
- PURPOSE
Isolated greater trochanteric (GT) fractures are often identified using plain radiography of patients with post-traumatic hip pain. In many cases, the fracture extends to form an occult intertrochanteric fracture. We conducted a study to determine the frequency of occult intertrochanteric fractures in patients diagnosed with isolated GT fractures using plain radiographs.
MATERIALS AND METHODS
Among 3,017 individuals who visited our emergency department with a trauma-induced pertrochanteric femur fracture between July 2004 and March 2018, 100 patients diagnosed with isolated GT fractures using plain radiographs were retrospectively analyzed. Patients were divided into two groups, those with: i) isolated GT fractures (group A) and ii) occult intertrochanteric fractures (group B). In addition, plain radiographs, magnetic resonance imaging results, and treatment methods were further analyzed in each group. If surgery treatment was needed, it was performed by one surgeon, and in all cases, a 2-hole dynamic hip screw was used.
RESULTS
Among the 100 cases of isolated GT fractures diagnosed using plain radiograph, additional examinations revealed that 10 (10.0%) were suffering from isolated GT fractures alone, while the remaining 90 (90.0%) were further diagnosed with occult intertrochanteric fracture. Gender, age, mechanism of injury, and bone mineral density did not correlate with fracture type.
CONCLUSION
In our analysis, 90% of injuries initially diagnosed as isolated GT fractures were found to extend into occult intertrochanteric fractures upon further examination with additional imaging modalities. Therefore, additional evaluation should be performed to test for the potential presence of occult intertrochanteric fractures and to establish appropriate treatment plans.
MeSH Terms
Figure
-
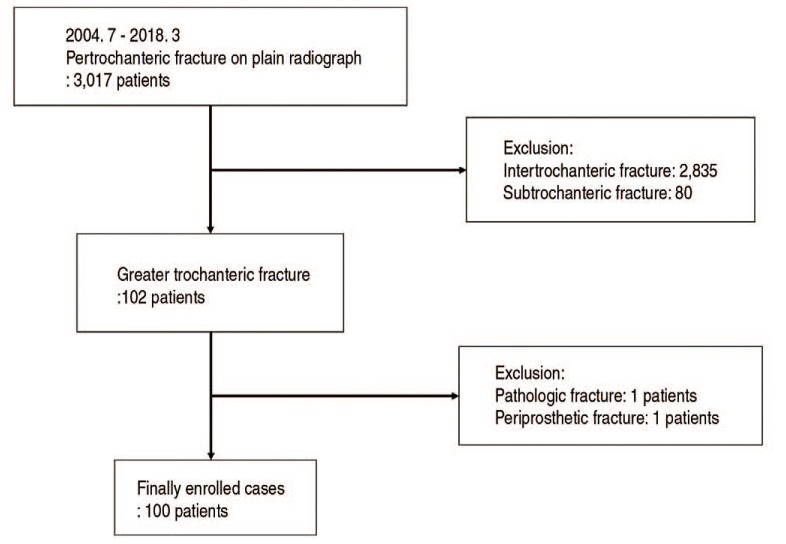
Fig. 1 Flow chart demonstrating how cases were selected and analyzed.

Fig. 2 An 87-year-old woman visited the hospital with right hip pain caused by a fall from height. (A) Plain radiography indicated an isolated greater trochanteric fracture. (B, C) A bone scan also revealed an isolated greater trochanteric fracture. (D) However, magnetic resonance imaging scans indicated that the fracture was more than half of the intertrochanteric area. (E) Surgical treatment was performed using two-hole dynamic hip screws.W.B: whole body bone scan, ANT: anterior, POST: posterior.

Fig. 3 A 36-year-old male patient visited the hospital with left hip pain following a traffic accident. Plain radiography (A) and magnetic resonance imaging (B) each indicated an isolated greater trochanteric fracture, and conservative treatment was performed.

Fig. 4 An 89-year-old woman visited the hospital with right hip pain caused by a fall from height. (A) Plain radiography indicated an isolated greater trochanteric fracture. (B) Magnetic resonance imagingscans further revealed an occult intertrochanteric fracture; however, the fracture was limited to less than half of the intertrochanteric area. (C) Conservative treatment was performed.
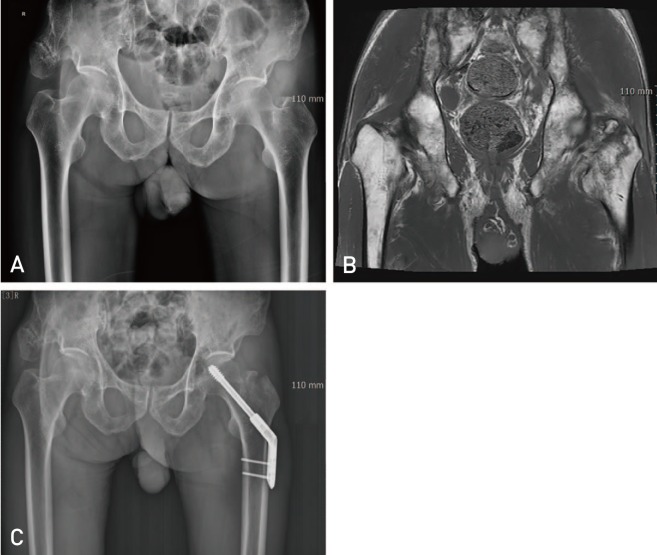
Fig. 5 A 75-year-old male visited the hospital with left hip pain caused by a fall from height. (A) Plain radiography indicated an isolated greater trochanteric fracture. (B) Magnetic resonance imaging scans further revealed an occult intertrochanteric fracture that was more than half of the intertrochanteric area. (C) Surgical treatment was performed using two-hole dynamic hip screws.
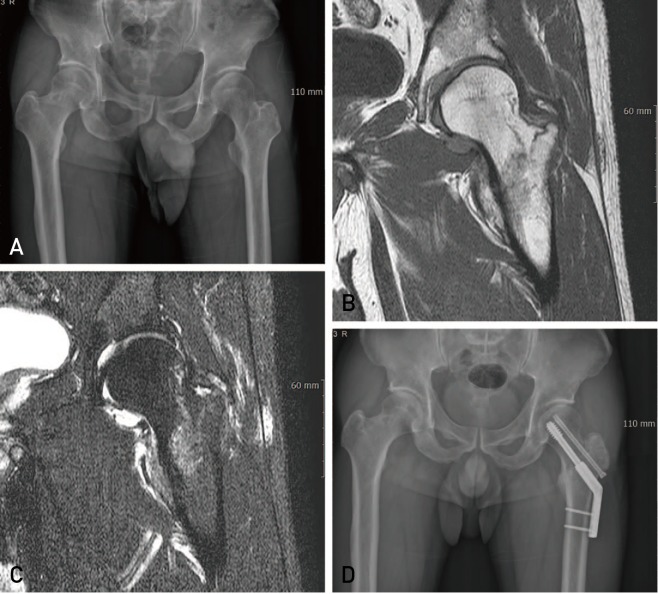
Fig. 6 A 41-year-old male visited the hospital with left hip pain caused by a fall from height. (A) Plain radiography indicated an isolated greater trochanteric fracture. (B, C) Magnetic resonance imaging scans further revealed an occult intertrochanteric fracture extended to more than half of the intertrochanteric area and the base of the neck. (D) Surgical treatment was performed using two-hole dynamic hip screws.
Reference
-
1. Milch H. Avulsion fracture of the great trochanter. Arch Surg. 1939; 38:334–350.
Article2. Beloosesky Y, Hershkovitz A, Guz A, Golan H, Salai M, Weiss A. Clinical characteristics and long-term mortality of occult hip fracture elderly patients. Injury. 2010; 41:343–347. PMID: 19744653.
Article3. Kim KC, Ha YC, Kim TY, Choi JA, Koo KH. Initially missed occult fractures of the proximal femur in elderly patients: implications for need of operation and their morbidity. Arch Orthop Trauma Surg. 2010; 130:915–920. PMID: 20437074.
Article4. Chung PH, Kang S, Kim JP, et al. Occult intertrochanteric fracture mimicking the fracture of greater trochanter. Hip Pelvis. 2016; 28:112–119. PMID: 27536653.
Article5. Feldman F, Staron R, Zwass A, Rubin S, Haramati N. MR imaging: its role in detecting occult fractures. Skeletal Radiol. 1994; 23:439–444. PMID: 7992109.
Article6. Rizzo PF, Gould ES, Lyden JP, Asnis SE. Diagnosis of occult fractures about the hip. Magnetic resonance imaging compared with bone-scanning. J Bone Joint Surg Am. 1993; 75:395–401. PMID: 8444918.
Article7. Chatha H, Ullah S, Cheema Z. Review article: Magnetic resonance imaging and computed tomography in the diagnosis of occult proximal femur fractures. J Orthop Surg (Hong Kong). 2011; 19:99–103. PMID: 21519088.
Article8. Rehman H, Clement RG, Perks F, White TO. Imaging of occult hip fractures: CT or MRI? Injury. 2016; 47:1297–1301. PMID: 26993257.9. Omura T, Takahashi M, Koide Y, et al. Evaluation of isolated fractures of the greater trochanter with magnetic resonance imaging. Arch Orthop Trauma Surg. 2000; 120:195–197. PMID: 10738882.
Article10. Craig JG, Moed BR, Eyler WR, van Holsbeeck M. Fractures of the greater trochanter: intertrochanteric extension shown by MR imaging. Skeletal Radiol. 2000; 29:572–576. PMID: 11127679.
Article11. Frihagen F, Nordsletten L, Tariq R, Madsen JE. MRI diagnosis of occult hip fractures. Acta Orthop. 2005; 76:524–530. PMID: 16195069.
Article12. Feldman F, Staron RB. MRI of seemingly isolated greater trochanteric fractures. AJR Am J Roentgenol. 2004; 183:323–329. PMID: 15269019.
Article13. Lee KH, Kim HM, Kim YS, et al. Isolated fractures of the greater trochanter with occult intertrochanteric extension. Arch Orthop Trauma Surg. 2010; 130:1275–1280. PMID: 20499242.
Article14. Arshad R, Riaz O, Aqil A, Bhuskute N, Ankarath S. Predicting intertrochanteric extension of greater trochanter fractures of the hip on plain radiographs. Injury. 2017; 48:692–694. PMID: 28126317.
Article15. Park JH, Shon HC, Chang JS, et al. How can MRI change the treatment strategy in apparently isolated greater trochanteric fracture? Injury. 2018; 49:824–828. PMID: 29566988.
Article16. Iwata T, Nozawa S, Dohjima T, et al. The value of T1-weighted coronal MRI scans in diagnosing occult fracture of the hip. J Bone Joint Surg Br. 2012; 94:969–973. PMID: 22733955.
Article17. Holder LE, Schwarz C, Wernicke PG, Michael RH. Radionuclide bone imaging in the early detection of fractures of the proximal femur (hip): multifactorial analysis. Radiology. 1990; 174:509–515. PMID: 2404320.
Article18. Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging. 5th ed. Philadelphia: W.B. Saunders Company;2006. p. 269–270.19. Deleanu B, Prejbeanu R, Tsiridis E, et al. Occult fractures of the proximal femur: imaging diagnosis and management of 82 cases in a regional trauma center. World J Emerg Surg. 2015; 10:55. PMID: 26587053.
Article20. Haubro M, Stougaard C, Torfing T, Overgaard S. Sensitivity and specificity of CT- and MRI-scanning in evaluation of occult fracture of the proximal femur. Injury. 2015; 46:1557–1561. PMID: 26015154.
Article21. Yun BJ, Myriam Hunink MG, Prabhakar AM, et al. Diagnostic imaging strategies for occult hip fractures: a decision and cost-effectiveness analysis. Acad Emerg Med. 2016; 23:1161–1169. PMID: 27286291.
Article22. Motomura G, Yamamoto T, Karasuyama K, Iwamoto Y. Bone SPECT/CT of femoral head subchondral insufficiency fracture. Clin Nucl Med. 2015; 40:752–754. PMID: 26164176.
Article23. Rieger B, Friederich NF, Rasch H, Hirschmann MT. [Non-dislocated osteoporotic insufficiency fracture of the medial femoral neck. SPECT/CT makes the diagnostic difference]. Unfallchirurg. 2014; 117:369–373. German. PMID: 23949134.24. Reddy T, McLaughlin PD, Mallinson PI, et al. Detection of occult, undisplaced hip fractures with a dual-energy CT algorithm targeted to detection of bone marrow edema. Emerg Radiol. 2015; 22:25–29.
Article25. Safran O, Goldman V, Applbaum Y, et al. Posttraumatic painful hip: sonography as a screening test for occult hip fractures. J Ultrasound Med. 2009; 28:1447–1452. PMID: 19854958.26. Alam A, Willett K, Ostlere S. The MRI diagnosis and management of incomplete intertrochanteric fractures of the femur. J Bone Joint Surg Br. 2005; 87:1253–1255. PMID: 16129752.
Article27. Rubin G, Malka I, Rozen N. Should we operate on occult hip fractures? Isr Med Assoc J. 2010; 12:316–317. PMID: 20929092.28. LaLonde B, Fenton P, Campbell A, Wilson P, Yen D. Immediate weight-bearing in suspected isolated greater trochanter fractures as delineated on MRI. Iowa Orthop J. 2010; 30:201–204. PMID: 21045999.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Occult Intertrochanteric Fracture Mimicking the Fracture of Greater Trochanter
- The Neccessity of Additional Supporting Fixation for the Unstable Intertrochanteric Fractures of the Femur in the Elderly
- Effect of Unreduced Lesser Trochanteric Fracture on Stability in Intertrochanteric Fracture of Femur
- Surgical Treatment of Femoral Unstable Intertrochanteric Fractures in Elderly Patients: Comparative Study between Compressive Hip Screws and Additional Trochanteric Stabilizing Plates
- Methods to Increase the Effectiveness of Trochanteric Stabilizing Plate for Unstable Femoral Intertrochanteric Fractures with Gtreater Trochanteric Fracture: Fixation of Greater Trochanter with Wire and Screw
