Anesthetic considerations for a patient with situs inversus totalis undergoing cardiac surgery: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, CHA Bundang Medical Center, Seongnam, Korea. aescula72@hanmail.net
- 2Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2447968
- DOI: http://doi.org/10.17085/apm.2019.14.2.193
Abstract
- A 58-year-old male patient with situs inversus totalis, a rare congenital malformation characterized by all asymmetric organs being formed as the mirror images of their normal morphologies, underwent mitral valve repair due to mitral valve prolapse. This case was reported to suggest that anesthesiologists should thoroughly understand the anatomy of these types of patients before providing cardiac anesthesia that often requires advanced monitoring and rely on their accurate interpretation. Accordingly, a few key points will be discussed with emphasis on reversing lead placement during electrocardiogram monitoring, using the left internal jugular vein for pulmonary artery catheterization, and firmly comprehending mirror image heart morphology to better conduct transesophageal echocardiography.
Keyword
MeSH Terms
Figure
-
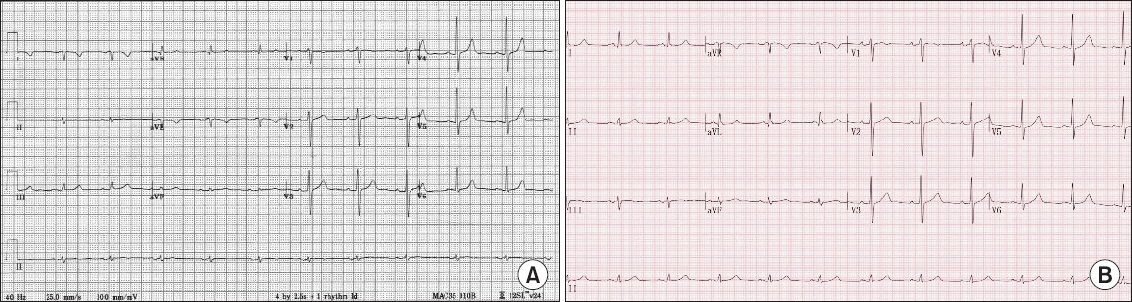
Fig. 1 (A) Echocardiogram with normal lead placement showing right axis deviation. (B) Normal echocardiogram with reverse lead placement. ECG: electrocardiogram.

Fig. 2 Anteroposterior chest X-ray on postoperative day 1. Arrows show the right curved shape of pulmonary artery inserted directly via left internal jugular vein without crossing the midline.
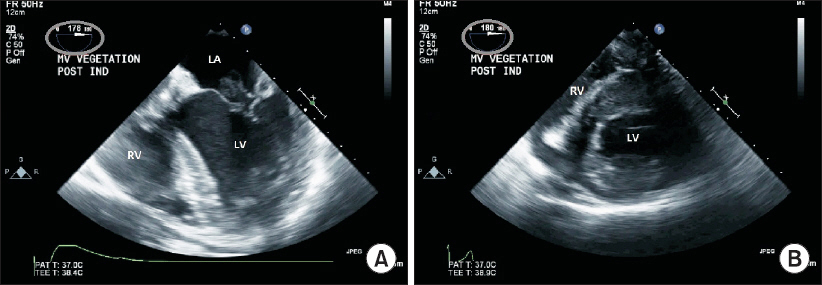
Fig. 3 (A) Transesophageal echocardiographic midesophageal four chamber view. (B) Transesophageal echocardiographic transgastric short axis view. These views were obtained at angle of 180° (circle). LA: left atrium, LV: left ventricle, RV: right ventricle.
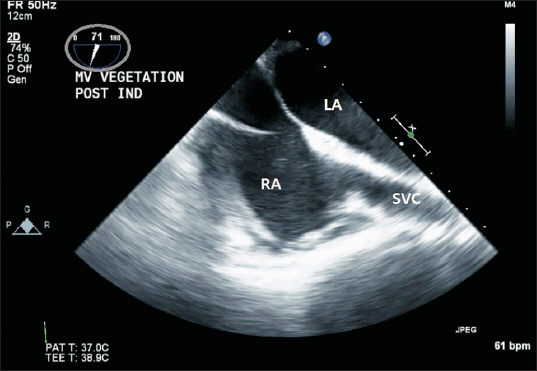
Fig. 4 Transesophageal echocardiographic bicaval view obtained at 70° (circle). LA: left atrium, RA: right atrium, SVC: superior vena cava.

Fig. 5 Transesophageal echocardiographic aortic valve short-axis view obtained at 140° (circle). AV: aortic valve, LA: left atrium, RA: right atrium, RV: right ventricle.
Reference
-
1. Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N. Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol. 2003; 88:143–55. DOI: 10.1016/S0167-5273(02)00539-9.2. Channabasappa SM, Mohan HS, Sarma J. A patient with situs inversus totalis presenting for emergency laparoscopic appendectomy: consideration for safe anesthetic management. Anesth Essays Res. 2013; 7:127–9. DOI: 10.4103/0259-1162.114019. PMID: 25885734. PMCID: PMC4173507.3. Bush A, Chodhari R, Collins N, Copeland F, Hall P, Harcourt J, et al. Primary ciliary dyskinesia: current state of the art. Arch Dis Child. 2007; 92:1136–40. DOI: 10.1136/adc.2006.096958. PMID: 17634184. PMCID: PMC2066071.4. Garg R, Goila A, Sood R, Pawar M, Borthakur B. Perioperative anesthetic management of a patient with biliary atresia, situs inversus totalis, and kartegener syndrome for hepatobiliary surgery. J Anaesthesiol Clin Pharmacol. 2011; 27:256–8. DOI: 10.4103/0970-9185.81837. PMID: 21772694. PMCID: PMC3127313.5. Koç A, Sönmez Y, Balaban O. Anaesthetic management for appendectomy in a patient with situs inversus totalis. Turk J Anaesthesiol Reanim. 2016; 44:105–7. DOI: 10.5152/TJAR.2016.33716. PMID: 27366569. PMCID: PMC4894195.6. Raut MS, Maheshwari A, Shad S, Rachna G. How standard transesophageal echocardiography views change with dextrocardia. Ann Card Anaesth. 2013; 16:218–20. DOI: 10.4103/0971-9784.114261. PMID: 23816679.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Port Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: A Case Report
- Neonatal Duodenal Obstruction Associated with Situs Inversus Totalis: A Case Report
- Laparoscopic cholecystectomy in a case of situs inversus totalis: a review of technical challenges and adaptations
- Laparoscopic Low Anterior Resection in a Rectal Cancer Patient with Situs Inversus Totalis: A Case Report
- Radical Subtotal Gastrectomy in Early Gastric Cancer Patient with Situs Inversus Totalis
