Anatomical and radiological angiographic study of the coronary ostia in the adult human hearts and their clinical significance
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine, Zagazig University, Zagazig, Egypt. ashrafnaeem2013@gmail.com
- 2Department of Anatomy, Faculty of Medicine, King Abdulaziz University (KAU), Jeddah, Saudi Arabia.
- 3Department of Cardiology, Faculty of Medicine, Zagazig University, Zagazig, Egypt.
- KMID: 2447009
- DOI: http://doi.org/10.5115/acb.2018.51.3.164
Abstract
- This study was carried out to investigate the morphometric parameters and variations of coronary ostia in the hearts of adult human cadavers and coronary angiographs. The hearts of 60 adult human cadavers and 400 coronary angiographs were used in this study. The root of the aorta was carefully dissected to clear aortic sinuses, coronary ostia, and sinutubular junction (STJ). Number, locations, internal diameter distance between coronary ostia and their corresponding STJ, sinus bottom, and valve commissures were investigated. The anterior aortic sinus (AAS) revealed a single ostium for right coronary artery (RCA) in 77.5% of male and 80% of female hearts. This ostium gave a common origin for RCA and third coronary artery (TCA) in 15% of male and 20% of female hearts. However, two separate ostia for RCA and TCA origin were seen in 20% of male and 15% of female hearts. Moreover, three ostia were seen in one male and one female hearts within AAS. Meanwhile, the left posterior aortic sinus showed a single ostium for left coronary artery (LCA) in 97.5% of male and 95% of female hearts and two ostia in one male and one female hearts. The ostia were commonly seen below STJ and less commonly were observed above STJ. The distance between the bottom of aortic sinus and LCA ostium was longer than that of RCA. The internal diameter of RCA ostium was significantly (P<0.05) narrower than that of LCA but with no significant sex difference. Moreover, anomalous of coronary ostia was observed in seven out 400 angiographs and in two cadaveric hearts. Knowledge the morphometric parameters and anatomical variations of coronary ostia helps the cardiac surgeons to overcome the possible difficulties that could occur during surgical and radiological coronary interventions.
Keyword
MeSH Terms
Figure
-
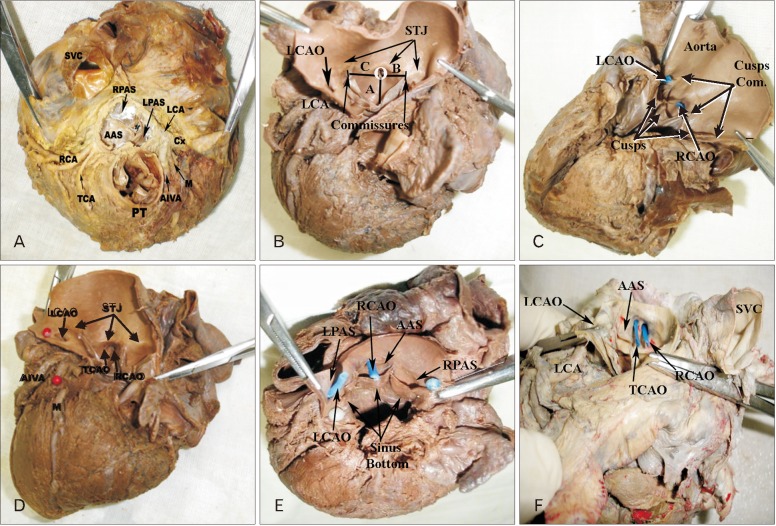
Fig. 1 Light photographs of adult cadaveric human hearts showing the root of the ascending aorta having the aortic sinuses and the ostia of coronary arteries. (A) The ascending aorta lies between the pulmonary trunk (PT) anteriorly and superior vena cava (SVC) posteriorly. It exhibits three aortic sinuses; the anterior aortic sinus (AAS), left posterior aortic sinus (LPAS), and right posterior aortic sinus (RPAS) above their corresponding aortic valve leaflets. The right coronary artery (RCA) and third coronary artery (TCA) originate from AAS through a common ostium, while the left coronary artery (LCA) originates from LPAS through single ostium. AIVA, anterior interventricular. (B) The ostium of the RCA (O) is surrounded by three lines (A–C) that represent the distance between the ostium and the bottom of the sinus vertically and the commissures of valve leaflets at both sides. The ostium of RCA is seen below sinu-tubular junction (STJ) within the AAS. Also, the ostium of LCA is seen below STJ within LPAS. (C) The ostia of both RCA (RCAO) and LCA (LCAO) are seen below the STJ within the corresponding aortic sinus. (D) The AAS shows two ostia below the STJ; one for RCA (RCAO) and the other for the third coronary artery origin (TCAO). (E) The ostia of both RCA (RCAO) and LCA (LCAO) are seen at the level of the STJ. (F) Both RCAO and TCAO are seen within AAS below STJ, while LCAO is present within the LPAS below STJ.
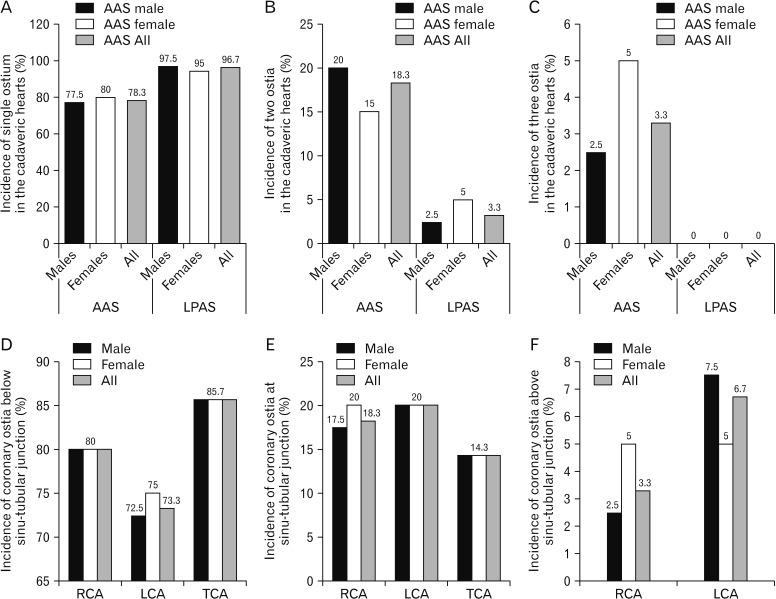
Fig. 2 The numerical and positional incidence of the coronary ostia in the cadaveric hearts (%). (A) The incidence of single ostium in the anterior aortic sinus (AAS) and left posterior aortic sinus (LPAS) is represented in male, female and all cadaveric hearts. (B) The incidence of two coronary ostia in both AAS and LPAS that are observed in male, female and all cadaveric hearts (%). (C) The incidence of three coronary ostia that are recorded within both AAS and LPAS in male, female and all cadaveric hearts (%). (D) The incidence of both right coronary artery (RCA) and left coronary artery (LCA) ostia below the level of the sinutubular junction (STJ) in male, female and all cadaveric hearts (%). TCA, third coronary artery. (E) The incidence of both RCA and LCA ostia at the level of the STJ in male, female and all cadaveric hearts (%). (F) The incidence of both RCA and LCA ostia above the level of the STJ in male, female and all cadaveric hearts (%).
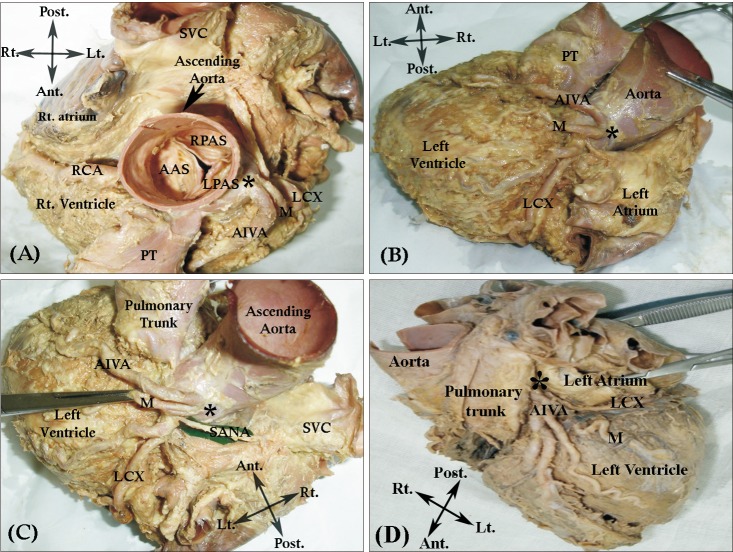
Fig. 3 Light photograph of cadaveric hearts showing original variations of the left coronary artery. (A) The anterior aortic sinus (AAS), left posterior aortic sinus (LPAS), and right posterior aortic sinus (RPAS) above the corresponding aortic cusps at the beginning of ascending aorta. The right coronary artery (RCA) originates from AAS and the branches of left coronary artery (LCA) originate from LPAS. The pulmonary trunk (PT) lies anterior to ascending aorta and superior vena cava (SVC) lies posterior to it. (B, C) The anterior interventricular (AIVA) and left circumflex branches (LCX) originate from LPAS through a common ostium (*) with an absence of LCA. The median branch (M) originates from LCX. (D) The large AIVA and small LCX branches of LCA originate directly from LPAS through a common ostium (*) with an absence of LCA. A median branch (M) is seen originating from AIVA.
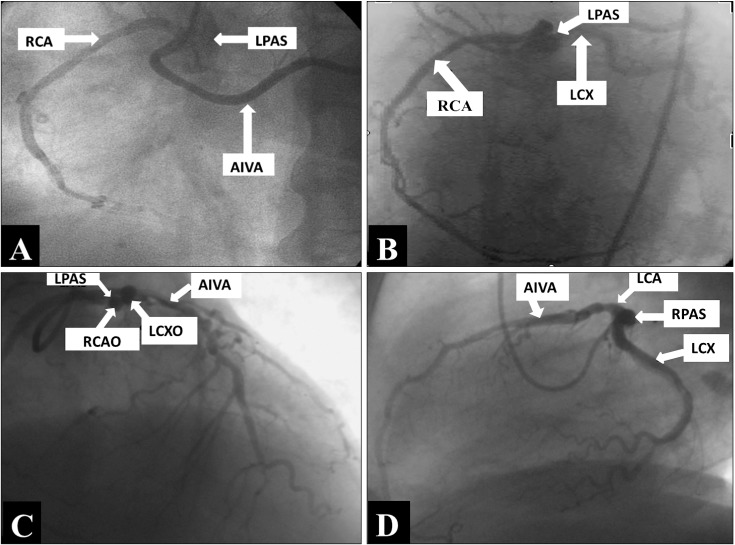
Fig. 4 Coronary angiographs of adult male human hearts showing different original variations of coronary arteries. (A) The right coronary artery (RCA) originates from the anterior interventricular branch (AIVA) of left coronary artery (LCA). (B) The RCA originates from the left posterior aortic sinus (LPAS). (C) The RCA and left circumflex branch (LCX) originate from LPAS. LCX and AIVA originate from two separate aortic sinuses. RCAO, ostium of the right coronary artery. (D) The LCA originates from the right posterior aortic sinus (RPAS).
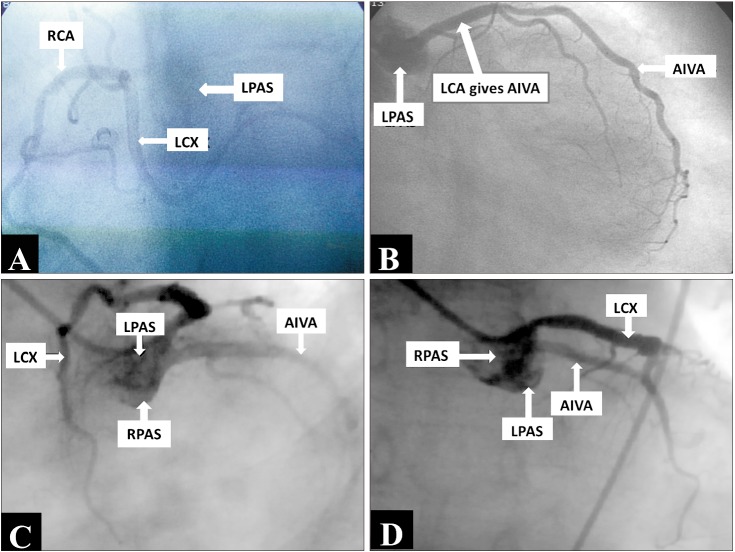
Fig. 5 Coronary angiographs of adult females showing the original anomalous of coronary arteries. (A) The right coronary artery (RCA) originates from the left circumflex branch (LCX). (B) The left coronary artery (LCA) gives only the anterior interventricular branch (AIVA). (C, D) The RCA originates from the LCX. AIVA originates from the right posterior aortic sinus (RPAS) and the LCX originates from the left posterior aortic sinus (LPAS).
Reference
-
1. Standring S. Gray's anatomy: the anatomical basis of clinical practice. 41st ed. Philadelphia, PA: Elsevier Churchill Livingstone;2016.2. Joshi SD, Joshi SS, Athavale SA. Origins of the coronary arteries and their significance. Clinics (Sao Paulo). 2010; 65:79–84. PMID: 20126349.3. Cavalcanti JS, de Melo NC, de Vasconcelos RS. Morphometric and topographic study of coronary ostia. Arq Bras Cardiol. 2003; 81:359–362. 365–368. PMID: 14666278.4. Kalpana R. A study on principal branches of coronary arteries on humans. J Anat Soc India. 2003; 52:137–140.5. Loukas M, Groat C, Khangura R, Owens DG, Anderson RH. The normal and abnormal anatomy of the coronary arteries. Clin Anat. 2009; 22:114–128. PMID: 19097062.6. Avirmed A, Auyrzana A, Nyamsurendejid D, Tumenjin E, Enebish S, Amgalanbaatar D. Morphometry of the coronary artery and heart microcirculation in infants. Folia Morphol (Warsz). 2012; 71:93–99. PMID: 22648587.7. Gajbe UL, Gosavi S, Meshram S, Gajbhiye VM. The anomalous origin of multiple coronary ostia and their clinical significance. J Clin Diagn Res. 2010; 4:2129–2133.8. Agrawal R. Anatomical study of coronary ostia in cadaveric human heart. Global J Res Anal. 2018; 7:23–25.9. Udaya Sankari T, Vijaya Kumar J, Saraswathi P. The anatomy of right conus artery and its clinical significance. Recent Res Sci Technol. 2011; 3:30–39.10. Bhele AV, Ughade HM, Shaikh S, Joge US. A study of course, branches and variations of the coronary arteries in the human cadaveric heart. Int J Contemp Med Res. 2017; 4:1533–1537.11. Fiss DM. Normal coronary anatomy and anatomic variations. Appl Radiol. 2007; 36:14–26.12. Stankovic I, Jesic M. Morphometric characteristics of the conal coronary artery. MJM. 2004; 8:2–6.13. Nalluri HB, Mohammed AA, Leela V. Anatomic variability of coronary ostia in adult human cadaveric hearts. Int J Anat Res. 2016; 4:1905–1911.14. Babaliaros V, Block P. State of the art percutaneous intervention for the treatment of valvular heart disease: a review of the current technologies and ongoing research in the field of percutaneous valve replacement and repair. Cardiology. 2007; 107:87–96. PMID: 16837777.15. Sirikonda P, Sreelatha S. Measurements and location of coronary ostia. Int J Biol Med Res. 2012; 3:2489–2496.16. Govsa F, Celik S, Aktaş EO, Aktaş S, Koçak A, Boydak B, Sen F. Anatomic variability of the coronary arterial orifices. Anadolu Kardiyol Derg. 2010; 10:3–8. PMID: 20149996.17. López-Mínguez JR, Climent V, Yen-Ho S, González-Fernández R, Nogales-Asensio JM, Sánchez-Quintana D. Structural features of the sinus of valsalva and the proximal portion of the coronary arteries: their relevance to retrograde aortocoronary dissection. Rev Esp Cardiol. 2006; 59:696–702. PMID: 16938212.18. Kulkarni JP, Paranjpe V. Topography, morphology and morphometry of coronary ostia: a cadaveric study. Eur J Anat. 2015; 19:165–170.19. Pejković B, Krajnc I, Anderhuber F. Anatomical variations of coronary ostia, aortocoronary angles and angles of division of the left coronary artery of the human heart. J Int Med Res. 2008; 36:914–922. PMID: 18831884.20. Manju M, Kaur D, Nair N. Morphology and morphometry of coronary ostia in adult human cadaveric hearts. J Anat Soc India. 2007; 56:115.21. Kim SY, Seo JB, Do KH, Heo JN, Lee JS, Song JW, Choe YH, Kim TH, Yong HS, Choi SI, Song KS, Lim TH. Coronary artery anomalies: classification and ECG-gated multi-detector row CT findings with angiographic correlation. Radiographics. 2006; 26:317–333. PMID: 16549600.22. Montaudon M, Latrabe V, Iriart X, Caix P, Laurent F. Congenital coronary arteries anomalies: review of the literature and multidetector computed tomography (MDCT)-appearance. Surg Radiol Anat. 2007; 29:343–355. PMID: 17563833.23. D'Souza MR, Ray B, Saxena A, Rastogi P, D'Souza AS, Gupta C, Muralimanju BV, Shetty P, Kumar V, Kumar N. Variations of origin of coronary artery and their importance. J Morphol Sci. 2015; 32:1–7.24. Saremi F, Abolhoda A, Ashikyan O, Milliken JC, Narula J, Gurudevan SV, Kaushal K, Raney A. Arterial supply to sinuatrial and atrioventricular nodes: imaging with multidetector CT. Radiology. 2008; 246:99–107. PMID: 18024438.25. Perez-Pomares JM, de la Pompa JL, Franco D, Henderson D, Ho SY, Houyel L, Kelly RG, Sedmera D, Sheppard M, Sperling S, Thiene G, van den Hoff M, Basso C. Congenital coronary artery anomalies: a bridge from embryology to anatomy and pathophysiology: a position statement of the development, anatomy, and pathology ESC Working Group. Cardiovasc Res. 2016; 109:204–216. PMID: 26811390.26. Harikrishnan S, Jacob SP, Tharakan J, Titus T, Kumar VK, Bhat A, Sivasankaran S, Bimal F, Moorthy KM, Kumar RP. Congenital coronary anomalies of origin and distribution in adults: a coronary arteriographic study. Indian Heart J. 2002; 54:271–275. PMID: 12216922.27. Leong SW, Borges AJ, Henry J, Butany J. Anomalous left coronary artery from the pulmonary artery: case report and review of the literature. Int J Cardiol. 2009; 133:132–134. PMID: 18279981.28. Zhang LJ, Yang GF, Huang W, Zhou CS, Chen P, Lu GM. Incidence of anomalous origin of coronary artery in 1879 Chinese adults on dual-source CT angiography. Neth Heart J. 2010; 18:466–470. PMID: 20978590.29. Smettei OA, Sayed S, Abazid RM. The prevalence of coronary artery anomalies in Qassim Province detected by cardiac computed tomography angiography. J Saudi Heart Assoc. 2017; 29:84–89. PMID: 28373781.30. Fujimoto S, Kondo T, Orihara T, Sugiyama J, Kondo M, Kodama T, Fukazawa H, Nagaoka H, Oida A, Yamazaki J, Takase S. Prevalence of anomalous origin of coronary artery detected by multidetector computed tomography at one center. J Cardiol. 2011; 57:69–76. PMID: 21146363.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Troponin T and I Expression in Failing and Hypertrophic Heart, and during Normal Development in Human
- The Incidence and Pattern of Coronary Artery Anomalies in the North-West of Iran: A Coronary Arteriographic Study
- Takayasu's Arteritis Involving the Ostia of Three Large Coronary Arteries
- Anatomical considerations of percutaneous transvenous mitral annuloplasty: a novel procedure for treatment of functional mitral regurgitation
- Ischemia-guided Revascularization for Stable Ischemic Heart Disease
