Which Osteotomy for Osteonecrosis of the Femoral Head and Which Patient for the Osteotomy?
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. khkoo@snu.ac.kr
- 2Rothman Institute, Thomas Jefferson University Hospital, Philadelphia, PA, USA.
- 3Department of Orthopaedic Surgery, Chung-Ang University College of Medicine, Seoul, Korea.
- KMID: 2445046
- DOI: http://doi.org/10.4055/cios.2019.11.2.137
Abstract
- Transtrochanteric curved varus osteotomy (TCVO) and transtrochanteric rotational osteotomy (TRO) are joint-preserving procedures for osteonecrosis of the femoral head. The purpose of this review is to provide up-to-date guidelines for the osteotomies. One retrospective comparison revealed that TCVO has shorter operation time, less bleeding, lower incidence of osteophyte formation, and lower rate of secondary collapse. To obtain successful results of the osteotomy, the patient should be younger than 40 years and should have a body mass index of less than 24 kg/m². The osteotomy should be performed in early stages of femoral head osteonecrosis before marked collapse of the femoral head. The patient should have a medium-size lesion and an enough viable bone to restore the intact articular surface and subchondral bone in the weight-bearing area.
Keyword
Figure
-
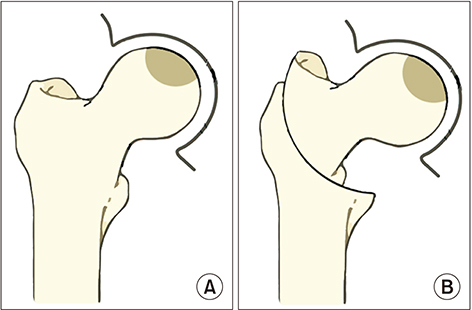
Fig. 1 Transtrochanteric curved varus osteotomy. (A) Osteonecrosis of femoral head. (B) A curved osteotomy is made between the greater and lesser trochanter, and the femoral head is rotated into a varus position.
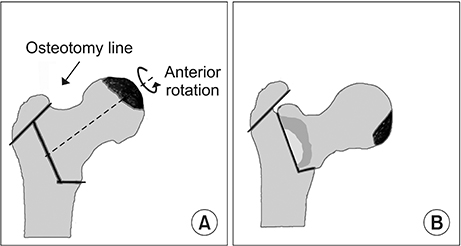
Fig. 2 Transtrochanteric rotational osteotomy. (A) The greater trochanter is osteotomized. (B) The femoral head fragment is rotated anteriorly.
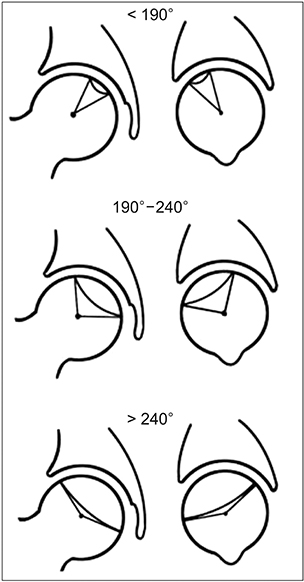
Fig. 3 The osteotomies should be performed in medium-size lesions with a combined necrotic angle between 190° and 240°.
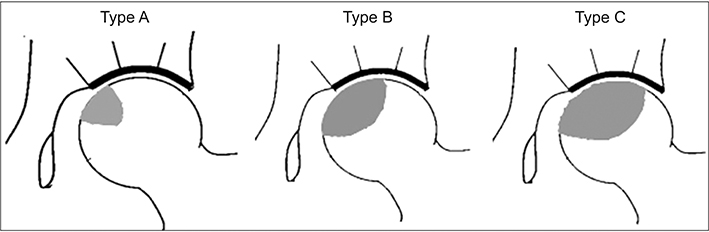
Fig. 4 The osteotomies should be performed in type B lesions involving the medial two-thirds or less of the weight-bearing portion according to Japanese Investigation Committee classification.

Fig. 5 Adequate area of viable bone for transtrochanteric rotational osteotomy is an arc (B) of > 120° between the central vertical line of the femoral head and the posterior margin of the necrotic portion on a midsagittal magnetic resonance imaging scan.
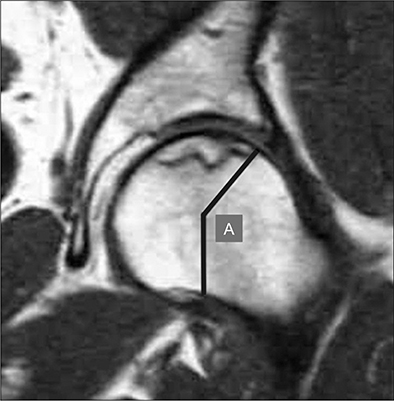
Fig. 6 Adequate area of viable bone for transtrochanteric curved varus osteotomy is an arc (A) of > 150° between the central vertical line of the femoral head and the lateral margin of the necrotic portion on the midcoronal magnetic resonance imaging scan.
Reference
-
1. Gutierrez F, Padilla S, Masia M, et al. Osteonecrosis in patients infected with HIV: clinical epidemiology and natural history in a large case series from Spain. J Acquir Immune Defic Syndr. 2006; 42(3):286–292.2. Shimizu K, Moriya H, Akita T, Sakamoto M, Suguro T. Prediction of collapse with magnetic resonance imaging of avascular necrosis of the femoral head. J Bone Joint Surg Am. 1994; 76(2):215–223.
Article3. Shibatani M, Fujioka M, Arai Y, et al. Degree of corticosteroid treatment within the first 2 months of renal transplantation has a strong influence on the incidence of osteonecrosis of the femoral head. Acta Orthop. 2008; 79(5):631–636.
Article4. Shigemura T, Nakamura J, Kishida S, et al. Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: prospective MRI study. Rheumatology (Oxford). 2011; 50(11):2023–2028.
Article5. Arlet J. Nontraumatic avascular necrosis of the femoral head: past, present, and future. Clin Orthop Relat Res. 1992; (277):12–21.6. Baek SH, Kim SY. Cementless total hip arthroplasty with alumina bearings in patients younger than fifty with femoral head osteonecrosis. J Bone Joint Surg Am. 2008; 90(6):1314–1320.
Article7. Kim YH, Choi Y, Kim JS. Cementless total hip arthroplasty with ceramic-on-ceramic bearing in patients younger than 45 years with femoral-head osteonecrosis. Int Orthop. 2010; 34(8):1123–1127.
Article8. Fye MA, Huo MH, Zatorski LE, Keggi KJ. Total hip arthroplasty performed without cement in patients with femoral head osteonecrosis who are less than 50 years old. J Arthroplasty. 1998; 13(8):876–881.
Article9. Sugioka Y. Transtrochanteric anterior rotational osteotomy of the femoral head in the treatment of osteonecrosis affecting the hip: a new osteotomy operation. Clin Orthop Relat Res. 1978; (130):191–201.10. Atsumi T, Muraki M, Yoshihara S, Kajihara T. Posterior rotational osteotomy for the treatment of femoral head osteonecrosis. Arch Orthop Trauma Surg. 1999; 119(7-8):388–393.
Article11. Nishio A, Sugioka Y. A new technique of the varus osteotomy at the upper end of the femur. Orthop Traumatol. 1971; 20(3):381–386.
Article12. Sakano S, Hasegawa Y, Torii Y, Kawasaki M, Ishiguro N. Curved intertrochanteric varus osteotomy for osteonecrosis of the femoral head. J Bone Joint Surg Br. 2004; 86(3):359–365.
Article13. Ikemura S, Yamamoto T, Jingushi S, Nakashima Y, Mawatari T, Iwamoto Y. Leg-length discrepancy after transtrochanteric curved varus osteotomy for osteonecrosis of the femoral head. J Bone Joint Surg Br. 2007; 89(6):725–729.
Article14. Zhao G, Yamamoto T, Ikemura S, et al. Radiological outcome analysis of transtrochanteric curved varus osteotomy for osteonecrosis of the femoral head at a mean follow-up of 12.4 years. J Bone Joint Surg Br. 2010; 92(6):781–786.
Article15. Lee YK, Park CH, Ha YC, Kim DY, Lyu SH, Koo KH. Comparison of surgical parameters and results between curved varus osteotomy and rotational osteotomy for osteonecrosis of the femoral head. Clin Orthop Surg. 2017; 9(2):160–168.
Article16. Inao S, Ando M, Gotoh E, Matsuno T. Minimum 10-year results of Sugioka's osteotomy for femoral head osteonecrosis. Clin Orthop Relat Res. 1999; (368):141–148.
Article17. Koo KH, Song HR, Yang JW, Yang P, Kim JR, Kim YM. Trochanteric rotational osteotomy for osteonecrosis of the femoral head. J Bone Joint Surg Br. 2001; 83(1):83–89.
Article18. Tooke SM, Amstutz HC, Hedley AK. Results of transtrochanteric rotational osteotomy for femoral head osteonecrosis. Clin Orthop Relat Res. 1987; (224):150–157.
Article19. Ha YC, Kim HJ, Kim SY, Kim KC, Lee YK, Koo KH. Effects of age and body mass index on the results of transtrochanteric rotational osteotomy for femoral head osteonecrosis. J Bone Joint Surg Am. 2010; 92(2):314–321.
Article20. Dean MT, Cabanela ME. Transtrochanteric anterior rotational osteotomy for avascular necrosis of the femoral head: long-term results. J Bone Joint Surg Br. 1993; 75(4):597–601.
Article21. Hammond BT, Charnley J. The sphericity of the femoral head. Med Biol Eng. 1967; 5(5):445–453.
Article22. Ha YC, Kim HJ, Kim SY, Kim KC, Lee YK, Koo KH. Effects of age and body mass index on the results of transtrochanteric rotational osteotomy for femoral head osteonecrosis: surgical technique. J Bone Joint Surg Am. 2011; 93:Suppl 1. 75–84.
Article23. Parfitt AM. Age-related structural changes in trabecular and cortical bone: cellular mechanisms and biomechanical consequences. Calcif Tissue Int. 1984; 36:Suppl 1. S123–S128.
Article24. Sugano N, Takaoka K, Ohzono K, Matsui M, Saito M, Saito S. Rotational osteotomy for non-traumatic avascular necrosis of the femoral head. J Bone Joint Surg Br. 1992; 74(5):734–739.
Article25. Hisatome T, Yasunaga Y, Takahashi K, Ochi M. Progressive collapse of transposed necrotic area after transtrochanteric rotational osteotomy for osteonecrosis of the femoral head induces osteoarthritic change: mid-term results of transtrochanteric rotational osteotomy for osteonecrosis of the femoral head. Arch Orthop Trauma Surg. 2004; 124(2):77–81.
Article26. Mont MA, Zywiel MG, Marker DR, McGrath MS, Delanois RE. The natural history of untreated asymptomatic osteonecrosis of the femoral head: a systematic literature review. J Bone Joint Surg Am. 2010; 92(12):2165–2170.
Article27. Mont MA, Fairbank AC, Krackow KA, Hungerford DS. Corrective osteotomy for osteonecrosis of the femoral head. J Bone Joint Surg Am. 1996; 78(7):1032–1038.28. Ha YC, Jung WH, Kim JR, Seong NH, Kim SY, Koo KH. Prediction of collapse in femoral head osteonecrosis: a modified Kerboul method with use of magnetic resonance images. J Bone Joint Surg Am. 2006; 88:Suppl 3. 35–40.
Article29. Sugano N, Atsumi T, Ohzono K, Kubo T, Hotokebuchi T, Takaoka K. The 2001 revised criteria for diagnosis, classification, and staging of idiopathic osteonecrosis of the femoral head. J Orthop Sci. 2002; 7(5):601–605.
Article30. Atsumi T, Kuroki Y. Modified Sugioka's osteotomy: more than 130 degrees posterior rotation for osteonecrosis of the femoral head with large lesion. Clin Orthop Relat Res. 1997; (334):98–107.31. Hiranuma Y, Atsumi T, Kajiwara T, Tamaoki S, Asakura Y. Evaluation of instability after transtrochanteric anterior rotational osteotomy for nontraumatic osteonecrosis of the femoral head. J Orthop Sci. 2009; 14(5):535–542.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posttraumatic Osteonecrosis of the Femoral Head after Nine Years of Posterior Femoral Head Fracture Dislocation
- Pelvic Osteotomy in Adults
- The Early Result of Anterior Rotational Osteotomy in the Treatment of Osteonecrosis of the Femoral Head
- Result of Sugioka's Transtrochanteric Osteotomy forOsteonecrosis of Femoral Head
- Femoral Varus Osteotomy Versus Salter Innominate Osteotomy in the Treatment of Legg - Calve - Perthes Disease
