Percutaneous Transabdominal Metallic Stent Placement for Palliation of Afferent Loop Syndrome: A Case Report
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Medical School and Hospital, Jeonju, Korea. ymhan@jbnu.ac.kr
- 2Research Institute of Clinical Medicine, Chonbuk National University Medical School and Hospital, Jeonju, Korea.
- 3Biomedical Research Institute, Chonbuk National University Medical School and Hospital, Jeonju, Korea.
- KMID: 2442523
- DOI: http://doi.org/10.3348/jksr.2019.80.2.333
Abstract
- The authors report a successful outcome after percutaneous transabdominal placement of a self-expandable metallic stent in a patient who had afferent loop syndrome caused by recurrent common bile duct adenocarcinoma. Enhanced abdominal CT showed marked dilation of the afferent loop adjacent to the anterior peritoneum, multiple hepatic metastases and lymph node metastasis around the choledochojejunal anastomosis site without marked dilation of intrahepatic bile ducts. Percutaneous drainage catheter was successfully placed to the dilated afferent loop just below the abdominal wall. Subsequent successful palliation of the afferent loop obstruction was achieved by placing a self-expandable metallic stent via the transabdominal route with the aid of cone-beam CT.
MeSH Terms
Figure
-
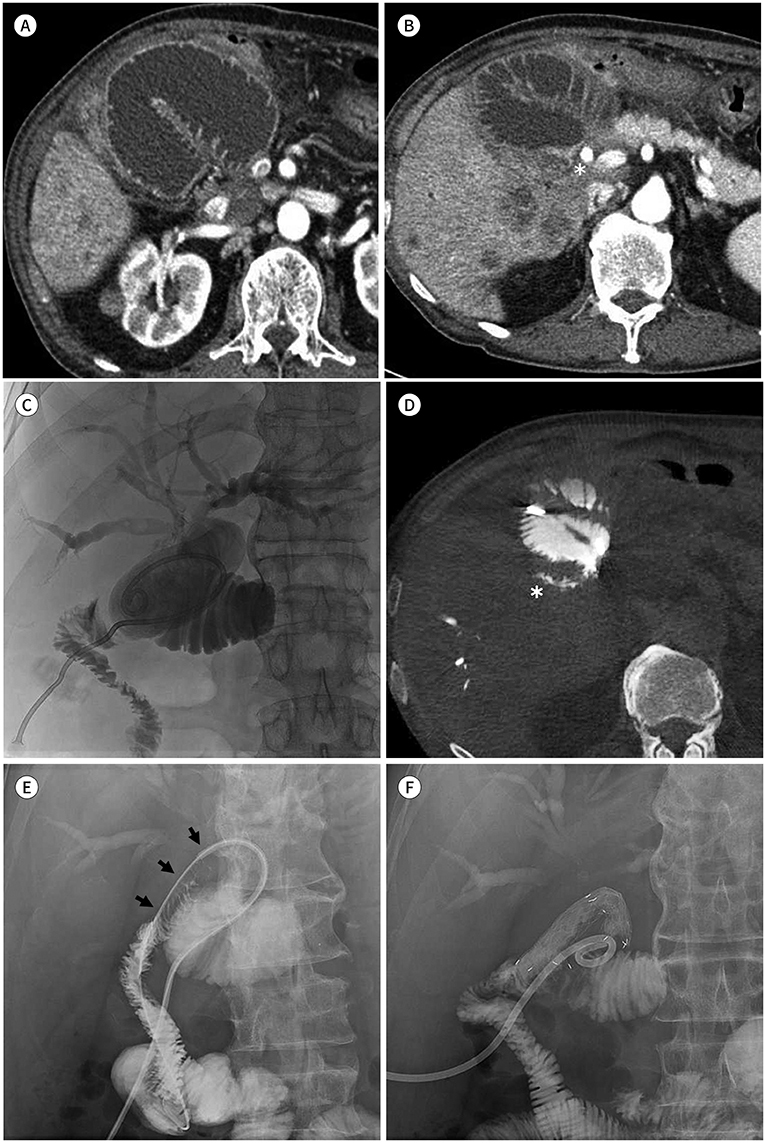
Fig. 1 A 72-year-old man diagnosed with afferent loop syndrome, treated with percutaneous transabdominal metallic stent placement for palliation. A. Abdominal contrast-enhanced CT on admission shows a markedly dilated afferent loop adjacent to the anterior peritoneum. B. The afferent loop is kinked at the choledochojejunostomy site (asterisk). Multiple masses with low enhancement suggesting hepatic metastasis of adenocarcinoma, and lymph node metastases around the choledochojejunal anastomosis site are shown without marked dilation of both intrahepatic bile ducts. C. An 8.5-Fr pigtail catheter is inserted into the afferent loop via the percutaneous transabdominal route. The biliary tree is dilated due to the infused contrast media. D. Cone-beam CT shows the outflow tract at the posterior aspect of the afferent limb (asterisk). E. Jejunography confirms an approximately 4-cm-long stricture of the afferent loop (arrows). F. A 20-mm and 8-cm self-expanding metallic stent was placed across the stenosis via the transabdominal route. A 12-Fr pigtail catheter is placed at the end of stent placement.
Reference
-
1. Jordan GL Jr. Surgical management of postgastrectomy problems. Arch Surg. 1971; 102:251–259.
Article2. Stabile BE, Passaro EJ. Sequels of surgery for peptic ulcer. In : Bockus HL, Berk JE, editors. Bockus gastroenterology. 4th ed. Philadelphia: WB Saunders;1985.3. Caldicott DG, Ziprin P, Morgan R. Transhepatic insertion of a metallic stent for the relief of malignant afferent loop obstruction. Cardiovasc Intervent Radiol. 2000; 23:138–140.
Article4. Gwon DI. Percutaneous transhepatic placement of covered, self-expandable nitinol stent for the relief of afferent loop syndrome: report of two cases. J Vasc Interv Radiol. 2007; 18:157–163.
Article5. Han K, Song HY, Kim JH, Park JH, Nam DH, Ryu MH, et al. Afferent loop syndrome: treatment by means of the placement of dual stents. AJR Am J Roentgenol. 2012; 199:W761–W766.
Article6. Lee LI, Teplick SK, Haskin PH, Sammon JK, Wolferth C, Amron G. Refractory afferent loop problems: percutaneous transhepatic management of two cases. Radiology. 1987; 165:49–50.
Article7. McDonald DG, Khalil MF, Vernon JK. Percutaneous transhepatic insertion of a jejunal feeding tube. Radiology. 1983; 148:309–310.
Article8. Morita S, Takemura T, Matsumoto S, Odani R. Septic shock after percutaneous transhepatic drainage of obstructed afferent loop: case report. Cardiovasc Intervent Radiol. 1989; 12:66–68.
Article9. Chevallier P, Novellas S, Motamedi JP, Gugenheim J, Brunner P, Bruneton JN. Percutaneous jejunostomy and stent placement for treatment of malignant Roux-en-Y obstruction: a case report. Clin Imaging. 2006; 30:283–286.
Article10. Laasch HU. Obstructive jaundice after bilioenteric anastomosis: transhepatic and direct percutaneous enteral stent insertion for afferent loop occlusion. Gut Liver. 2010; 4:Suppl 1. S89–S95.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous metallic stent placement for malignant afferent loop syndrome via the blind end of the jejunal limb after biliary reconstruction
- Metal Stent Placement in the Afferent Loop Obstructed by Peritoneal Metastases—Experience of Five Cases
- Percutaneous Enteral Stent Placement Using a Transhepatic Access for Palliation of Malignant Bowel Obstruction after Surgery
- Perforated Afferent Loop Syndrome in a Patient with Recurrent Gastric Cancer: Non-Surgical Treatment with Percutaneous Transhepatic Duodenal Drainage and Endoscopic Stent
- A Case of Afferent Loop Syndrome Treated by Endoscopic Metal Stent Insertion Using Two Endoscopes
