Management of Coarctation of The Aorta in Adult Patients: State of The Art
- Affiliations
-
- 1King Saud Bin Abdulaziz University for Health Science, Jeddah, Saudi Arabia. wakash73@hotmail.com
- 2Department of Cardiology, King Faisal Cardiac Center, Ministry of national Guard Health Affairs, Jeddah, Saudi Arabia.
- 3King Abdullah international medical research center Jeddah, Saudi Arabia.
- 4Department of Pediatrics, Sidra Heart Center, Sidra Medicine, Doha, Qatar.
- 5Weill Cornell Medicine, New York, NY, USA.
- KMID: 2441133
- DOI: http://doi.org/10.4070/kcj.2018.0433
Abstract
- Coarctation of the aorta (CoA) is a common form of congenital heart disease. Adult patients with CoA may be asymptomatic or may present with hypertension. Over the last few years, endovascular management of adult patients with CoA emerged as the preferred strategy. Stent implantation, though technically challenging, offers the best and most lasting therapy. In this paper, we will review technical considerations and outcome of patients undergoing stent implantation for CoA.
MeSH Terms
Figure
-
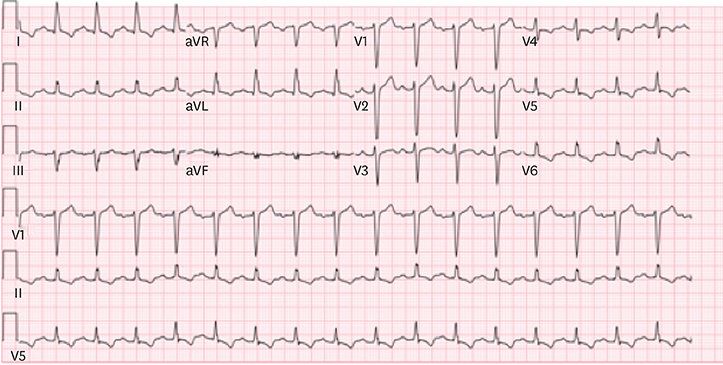
Figure 1 An electrocardiogram of a 45-year old male with coarctation of the aorta. There is evidence of ischemic changes.
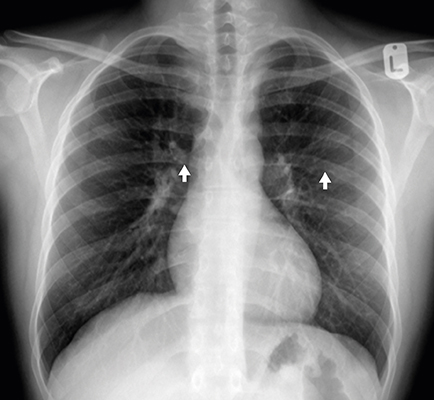
Figure 2 Chest radiograph of a patient with long-standing coarctation of the aorta demonstrating typical findings of coarctation: rib notching (arrows) and ‘3 sign’ beneath the aortic notch.
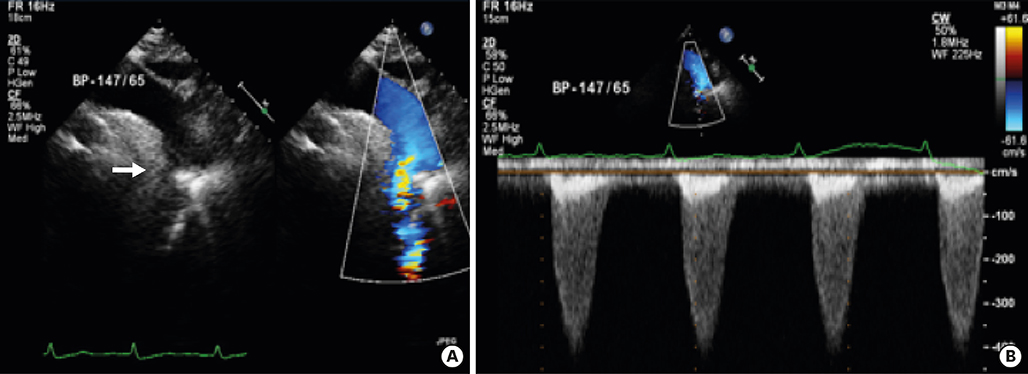
Figure 3 (A) A two-dimensional TTE from the suprasternal view demonstrating a discrete narrowing just distal to the take-off of the left subclavian artery (arrow) with continuous high velocity color Doppler signal across the coarctation. (B) Continuous wave Doppler TTE showing continuation of anterograde flow during diastole and peak pressure gradient of 60 mmHg across the coarctation. TTE = transthoracic echocardiography.
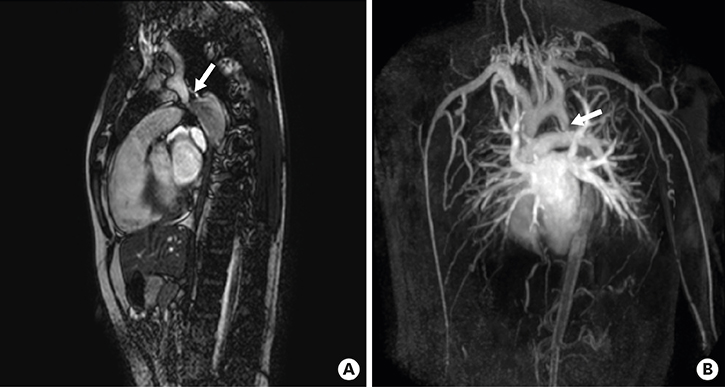
Figure 4 (A) Cardiac magnetic resonance image in sagittal view revealing discrete coarctation of the aorta (arrow). (B) Different view is cardiac magnetic resonance image revealing extensive collaterals.
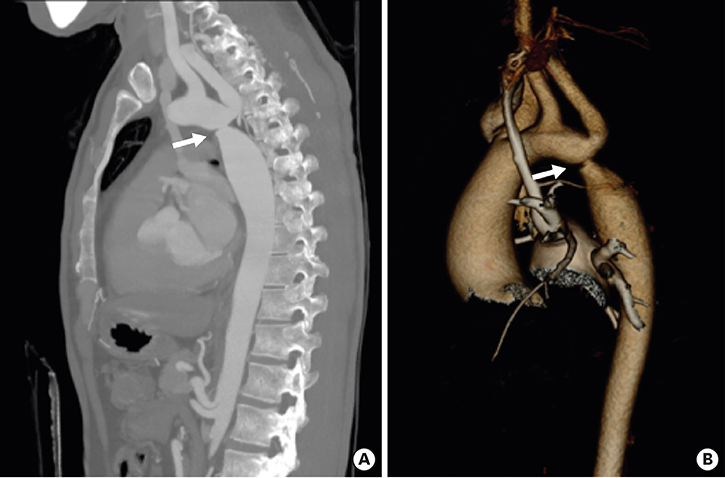
Figure 5 (A) Computed tomographic angiogram is revealing coarctation of the aorta just at the origin of the left subclavian artery (arrow). (B) 3D volume rendered reconstruction of the same patient revealing the coarctation (arrow), note the incidental finding of persistent left superior vena cava to left atrium.
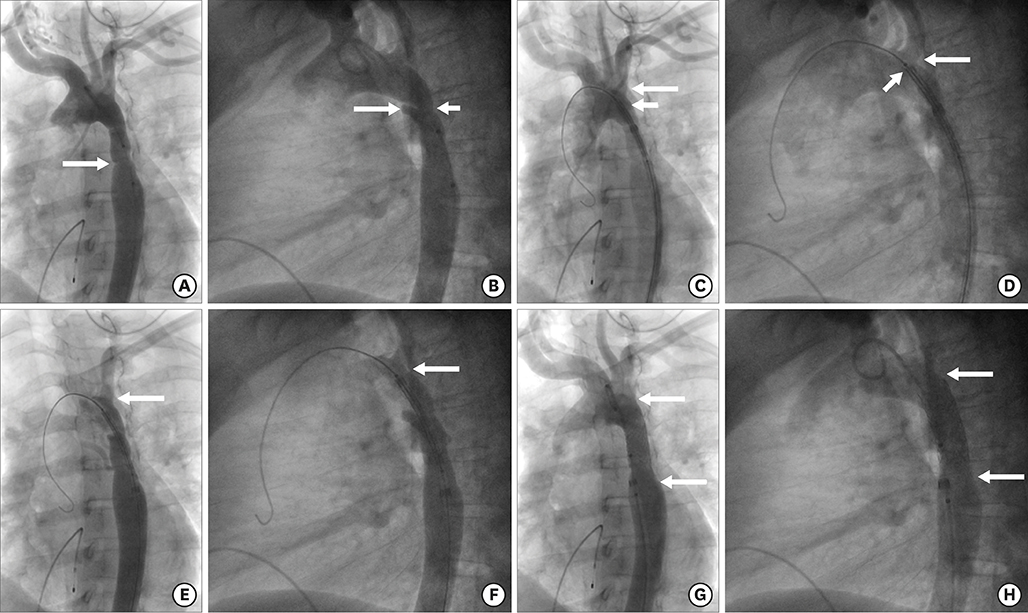
Figure 6 Angiogram in the transverse arch in left anterior oblique 30° (A) and straight lateral 90° (B) in a 28 years female patient with severe coarctation of the aorta, with a gradient of 30 mmHg. (A) The coarctation ridge (arrow). (B) Ductal diverticulum (long arrow) and the coarctation juxta ductal (shorter arrow). Note, there is a pacing catheter in the right ventricle. (C, D) Angiogram via side arm of delivery sheath (covered stent [Bentley 14 mm×39 mm] is uncovered half way). (C) Origin of the left subclavian artery (long arrow) and proximal tip of the stent (short arrow). (E, F) Angiogram via side arm of sheath after uncovering the stent completely. Note, origin of the left subclavian artery (arrow). (G, H) Angiogram via pigtail catheter in transverse arch after complete stent deployment showing good position (arrows) and remodelling of the area of coarctation. Residual gradient was 0 mmHg.
Reference
-
1. Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998–2005. J Pediatr. 2008; 153:807–813.
Article2. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002; 39:1890–1900.
Article3. Donti A, Spinardi L, Brighenti M, et al. Frequency of intracranial aneurysms determined by magnetic resonance angiography in children (mean age 16) having operative or endovascular treatment of coarctation of the aorta (mean age 3). Am J Cardiol. 2015; 116:630–633.
Article4. Connolly HM, Huston J 3rd, Brown RD Jr, Warnes CA, Ammash NM, Tajik AJ. Intracranial aneurysms in patients with coarctation of the aorta: a prospective magnetic resonance angiographic study of 100 patients. Mayo Clin Proc. 2003; 78:1491–1499.
Article5. Ho SY, Anderson RH. Coarctation, tubular hypoplasia, and the ductus arteriosus. Histological study of 35 specimens. Br Heart J. 1979; 41:268–274.
Article6. Rudolph AM, Heymann MA, Spitznas U. Hemodynamic considerations in the development of narrowing of the aorta. Am J Cardiol. 1972; 30:514–525.
Article7. Lin AE, Basson CT, Goldmuntz E, et al. Adults with genetic syndromes and cardiovascular abnormalities: clinical history and management. Genet Med. 2008; 10:469–494.
Article8. Wilson PD, Loffredo CA, Correa-Villaseñor A, Ferencz C. Attributable fraction for cardiac malformations. Am J Epidemiol. 1998; 148:414–423.
Article9. Preventza O, Livesay JJ, Cooley DA, Krajcer Z, Cheong BY, Coselli JS. Coarctation-associated aneurysms: a localized disease or diffuse aortopathy. Ann Thorac Surg. 2013; 95:1961–1967.
Article10. Campbell M. Natural history of coarctation of the aorta. Br Heart J. 1970; 32:633–640.
Article11. Rhodes JF, Hijazi ZM, Sommer RJ. Pathophysiology of congenital heart disease in the adult, part II. Simple obstructive lesions. Circulation. 2008; 117:1228–1237.12. Kenny D, Hijazi ZM. Coarctation of the aorta: from fetal life to adulthood. Cardiol J. 2011; 18:487–495.
Article13. Liberthson RR, Pennington DG, Jacobs ML, Daggett WM. Coarctation of the aorta: review of 234 patients and clarification of management problems. Am J Cardiol. 1979; 43:835–840.
Article14. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease. J Am Coll Cardiol. 2018.15. Baumgartner H, Bonhoeffer P, De Groot NM, et al. ESC guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J. 2010; 31:2915–2957.16. Marshall AC, Perry SB, Keane JF, Lock JE. Early results and medium-term follow-up of stent implantation for mild residual or recurrent aortic coarctation. Am Heart J. 2000; 139:1054–1060.
Article17. Kaemmerer H. Aortic coarctation and interrupted aortic arch. In : Gatzoulis MA, Webb GD, Daubeney PE, editors. Diagnosis and Management of Adult Congenital Heart Disease. 2nd edition. Philadelphia, PA: Elselvier Saunders;2011. p. 261–270.18. Walhout RJ, Lekkerkerker JC, Oron GH, Hitchcock FJ, Meijboom EJ, Bennink GB. Comparison of polytetrafluoroethylene patch aortoplasty and end-to-end anastomosis for coarctation of the aorta. J Thorac Cardiovasc Surg. 2003; 126:521–528.
Article19. Beekman RH, Rocchini AP, Behrendt DM, et al. Long-term outcome after repair of coarctation in infancy: subclavian angioplasty does not reduce the need for reoperation. J Am Coll Cardiol. 1986; 8:1406–1411.
Article20. Thomson JD, Mulpur A, Guerrero R, Nagy Z, Gibbs JL, Watterson KG. Outcome after extended arch repair for aortic coarctation. Heart. 2006; 92:90–94.
Article21. Burch PT, Cowley CG, Holubkov R, et al. Coarctation repair in neonates and young infants: is small size or low weight still a risk factor? J Thorac Cardiovasc Surg. 2009; 138:547–552.
Article22. Karamlou T, Bernasconi A, Jaeggi E, et al. Factors associated with arch reintervention and growth of the aortic arch after coarctation repair in neonates weighing less than 2.5 kg. J Thorac Cardiovasc Surg. 2009; 137:1163–1167.
Article23. Wada T, Yao H, Miyamoto T, Mukai S, Yamamura M. Prevention and detection of spinal cord injury during thoracic and thoracoabdominal aortic repairs. Ann Thorac Surg. 2001; 72:80–84.
Article24. Lock JE, Bass JL, Amplatz K, Fuhrman BP, Castaneda-Zuniga W. Balloon dilation angioplasty of aortic coarctations in infants and children. Circulation. 1983; 68:109–116.
Article25. Mendelsohn AM, Lloyd TR, Crowley DC, Sandhu SK, Kocis KC, Beekman RH 3rd. Late follow-up of balloon angioplasty in children with a native coarctation of the aorta. Am J Cardiol. 1994; 74:696–700.
Article26. O'Laughlin MP, Perry SB, Lock JE, Mullins CE. Use of endovascular stents in congenital heart disease. Circulation. 1991; 83:1923–1939.27. Trent MS, Parsonnet V, Shoenfeld R, et al. A balloon-expandable intravascular stent for obliterating experimental aortic dissection. J Vasc Surg. 1990; 11:707–717.
Article28. Forbes TJ, Garekar S, Amin Z, et al. Procedural results and acute complications in stenting native and recurrent coarctation of the aorta in patients over 4 years of age: a multi-institutional study. Catheter Cardiovasc Interv. 2007; 70:276–285.
Article29. Cheatham JP. Stenting of coarctation of the aorta. Catheter Cardiovasc Interv. 2001; 54:112–125.
Article30. Hartman EM, Groenendijk IM, Heuvelman HM, Roos-Hesselink JW, Takkenberg JJ, Witsenburg M. The effectiveness of stenting of coarctation of the aorta: a systematic review. EuroIntervention. 2015; 11:660–668.
Article31. Forbes TJ, Moore P, Pedra CA, et al. Intermediate follow-up following intravascular stenting for treatment of coarctation of the aorta. Catheter Cardiovasc Interv. 2007; 70:569–577.
Article32. Bulbul ZR, Bruckheimer E, Love JC, Fahey JT, Hellenbrand WE. Implantation of balloon-expandable stents for coarctation of the aorta: implantation data and short-term results. Cathet Cardiovasc Diagn. 1996; 39:36–42.
Article33. Pilla CB, Fontes VF, Pedra CA. Endovascular stenting for aortic coarctation. Expert Rev Cardiovasc Ther. 2005; 3:879–890.
Article34. Golden AB, Hellenbrand WE. Coarctation of the aorta: stenting in children and adults. Catheter Cardiovasc Interv. 2007; 69:289–299.
Article35. Yang L, Chua X, Rajgor DD, Tai BC, Quek SC. A systematic review and meta-analysis of outcomes of transcatheter stent implantation for the primary treatment of native coarctation. Int J Cardiol. 2016; 223:1025–1034.
Article36. Meadows J, Minahan M, McElhinney DB, McEnaney K, Ringel R. COAST Investigators. Intermediate outcomes in the prospective, multicenter coarctation of the aorta stent trial (COAST). Circulation. 2015; 131:1656–1664.
Article37. Taggart NW, Minahan M, Cabalka AK, et al. Immediate outcomes of covered stent placement for treatment or prevention of aortic wall injury associated with coarctation of the aorta (COAST II). JACC Cardiovasc Interv. 2016; 9:484–493.38. Sohrabi B, Jamshidi P, Yaghoubi A, et al. Comparison between covered and bare Cheatham-Platinum stents for endovascular treatment of patients with native post-ductal aortic coarctation: immediate and intermediate-term results. JACC Cardiovasc Interv. 2014; 7:416–423.39. Forbes TJ, Kim DW, Du W, et al. Comparison of surgical, stent, and balloon angioplasty treatment of native coarctation of the aorta: an observational study by the CCISC (Congenital Cardiovascular Interventional Study Consortium). J Am Coll Cardiol. 2011; 58:2664–2674.40. Carr JA. The results of catheter-based therapy compared with surgical repair of adult aortic coarctation. J Am Coll Cardiol. 2006; 47:1101–1107.
Article41. Bocelli A, Favilli S, Pollini I, et al. Prevalence and long-term predictors of left ventricular hypertrophy, late hypertension, and hypertensive response to exercise after successful aortic coarctation repair. Pediatr Cardiol. 2013; 34:620–629.
Article42. Canniffe C, Ou P, Walsh K, Bonnet D, Celermajer D. Hypertension after repair of aortic coarctation--a systematic review. Int J Cardiol. 2013; 167:2456–2461.43. Choudhary P, Canniffe C, Jackson DJ, Tanous D, Walsh K, Celermajer DS. Late outcomes in adults with coarctation of the aorta. Heart. 2015; 101:1190–1195.
Article44. O'Sullivan J. Late hypertension in patients with repaired aortic coarctation. Curr Hypertens Rep. 2014; 16:421.45. Kenny D, Polson JW, Martin RP, Paton JF, Wolf AR. Hypertension and coarctation of the aorta: an inevitable consequence of developmental pathophysiology. Hypertens Res. 2011; 34:543–547.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Coarctation of the Aorta Treated with Balloon Angioplasty
- Extraanatomic Aortic Bypass through a Median Sternotomy in a Patient with Coarctation of Aorta Associated with Annuloaortic Ectasia: A case report
- Use of Covered Stents to Treat Coarctation of the Aorta
- A Case Report of Balloon Angioplasty for Coarctation of Aorta in Adult
- Extraanatomic Ascending-to-Descending Aorta Bypass Graft for Atypical Coarctation: A case report
