Complex Regional Pain Syndrome of Non-hemiplegic Upper Limb in a Stroke Patient: A Case Report
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital, Seoul, Korea. rmpyun@korea.ac.kr
- 2Brain Convergence Research Center, Korea University Anam Hospital, Seoul, Korea.
- KMID: 2440983
- DOI: http://doi.org/10.5535/arm.2018.42.1.175
Abstract
- Complex regional pain syndrome (CRPS) type I in stroke patients is usually known to affect the hemiplegic upper limb. We report a case of CRPS presented in an ipsilesional arm of a 72-year-old female patient after an ischemic stroke at the left middle cerebral artery territory. Clinical signs such as painful range of motion and hyperalgesia of her left upper extremity, swollen left hand, and dystonic posture were suggestive of CRPS. A three-phase bone scintigraphy showed increased uptake in all phases in the ipsilesional arm. Diffusion tensor tractography showed significantly decreased fiber numbers of the corticospinal tract and the spinothalamic tract in both unaffected and affected hemispheres. Pain and range of motion of the left arm of the patient improved after oral steroids with a starting dose of 50 mg/day.
MeSH Terms
Figure
-
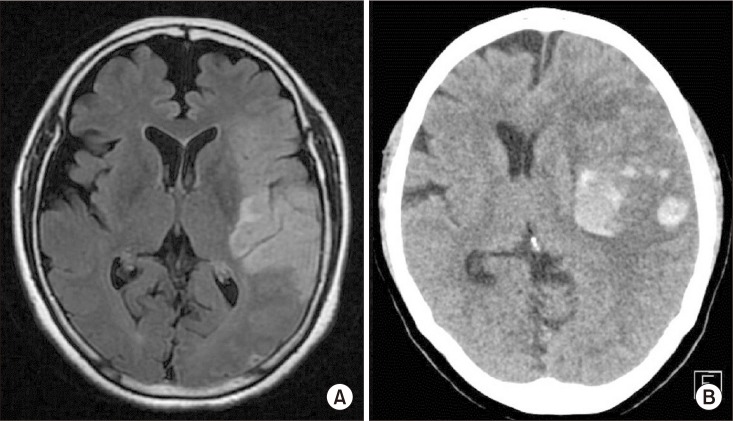
Fig. 1 (A) Brain magnetic resonance imaging (T2 FLAIR image, axial view) showing infarction of the left middle cerebral arterial territory. (B) Brain computed tomography image 1 day after infarction showing an acute hemorrhagic transformation resulting in midline shifting.

Fig. 2 Dystonia like posture of the left upper limb. Note fingers of the left hand forming a ‘V’ shape (arrow).
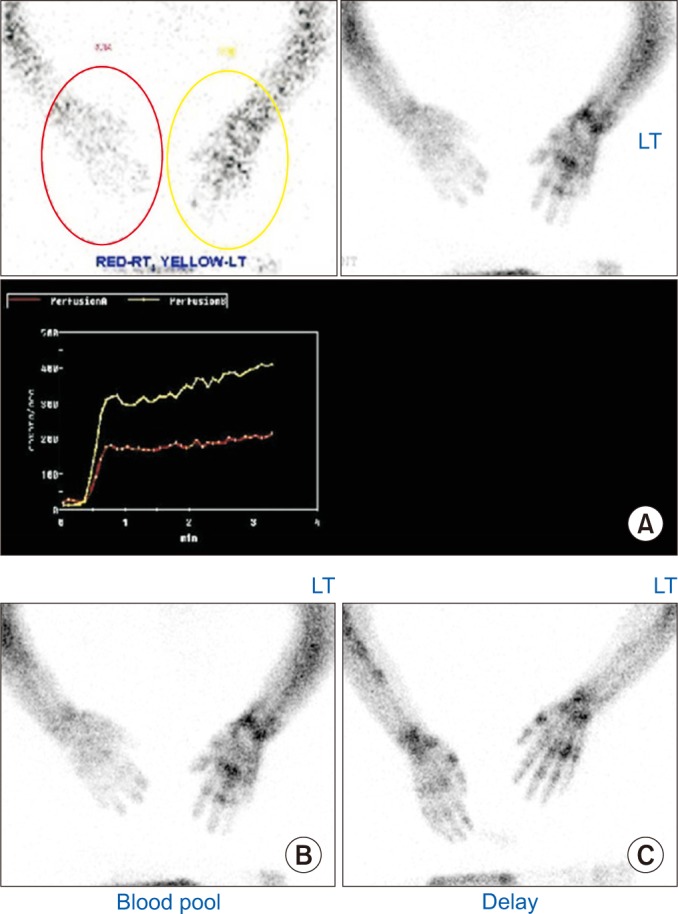
Fig. 3 Three-phase bone scintigraphy of clinically suspected complex regional pain syndrome (CRPS) of a non-hemiplegic upper limb in the patient with left cerebral infarction. (A) Perfusion phase. Perfusion to the left hand was higher than that to the right hand. (B) Blood pool phase. Blood pool to the left hand was higher than that to the right hand. (C) Delayed phase. Diffusely increased radionuclide uptakes in the left upper extremity.
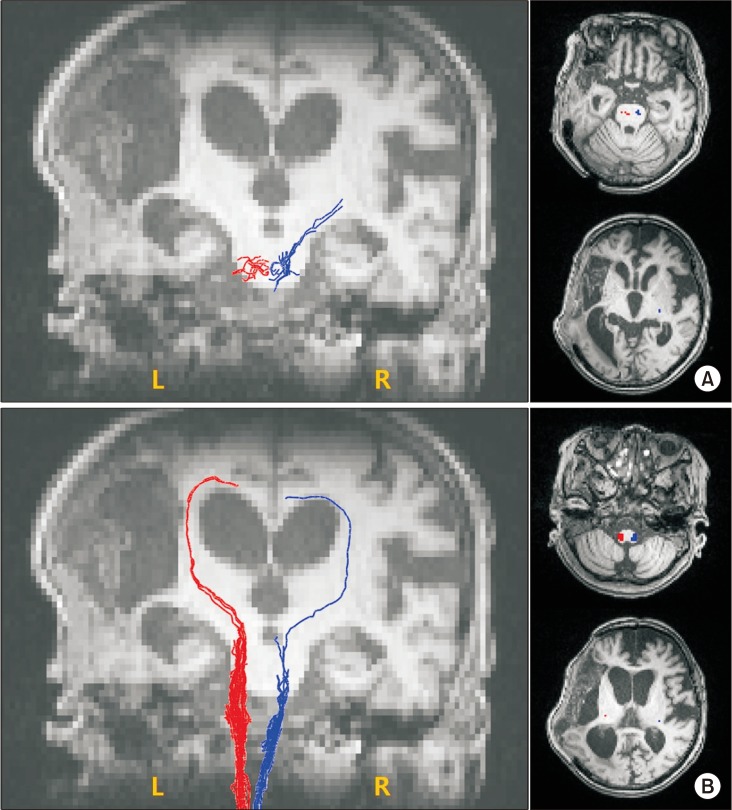
Fig. 4 Tractography for the corticospinal tract (A) and spinothalamic tract (B) showing significant volume reduction in both hemispheres.
Reference
-
1. Norman Harden R, Bruehl SP. Diagnostic criteria: the statistical derivation of the four criterion factors. In : Wilson PR, Stanton-Hicks M, Harden RN, editors. CRPS: current diagnosis and therapy. 1st ed. Seattle: IASP Press;2005. p. 45–58.2. Marinus J, Moseley GL, Birklein F, Baron R, Maihofner C, Kingery WS, et al. Clinical features and pathophysiology of complex regional pain syndrome. Lancet Neurol. 2011; 10:637–648. PMID: 21683929.
Article3. Chae J. Poststroke complex regional pain syndrome. Top Stroke Rehabil. 2010; 17:151–162. PMID: 20797958.
Article4. Schwenkreis P, Maier C, Tegenthoff M. Functional imaging of central nervous system involvement in complex regional pain syndrome. AJNR Am J Neuroradiol. 2009; 30:1279–1284. PMID: 19386737.
Article5. Geha PY, Baliki MN, Harden RN, Bauer WR, Parrish TB, Apkarian AV. The brain in chronic CRPS pain: abnormal gray-white matter interactions in emotional and autonomic regions. Neuron. 2008; 60:570–581. PMID: 19038215.
Article6. Azqueta-Gavaldon M, Schulte-Gocking H, Storz C, Azad S, Reiners A, Borsook D, et al. Basal ganglia dysfunction in complex regional pain syndrome: a valid hypothesis? Eur J Pain. 2017; 21:415–424. PMID: 27805769.7. Han EY, Jung HY, Kim MO. Absent median somatosensory evoked potential is a predictor of type I complex regional pain syndrome after stroke. Disabil Rehabil. 2014; 36:1080–1084. PMID: 24050813.
Article8. Hong JH, Kim SH, Kim OL, Byun WM, Jang SH. Neural tract injuries by brain herniations after head trauma. J Head Trauma Rehabil. 2012; 27:154–158. PMID: 21386711.
Article9. Hong JH, Bai DS, Jeong JY, Choi BY, Chang CH, Kim SH, et al. Injury of the spino-thalamo-cortical pathway is necessary for central post-stroke pain. Eur Neurol. 2010; 64:163–168. PMID: 20699616.
Article10. Wasner G, Schattschneider J, Binder A, Baron R. Complex regional pain syndrome: diagnostic, mechanisms, CNS involvement and therapy. Spinal Cord. 2003; 41:61–75. PMID: 12595868.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Contralateral Mirror Image Spreading in Post-Stroke Complex Regional Pain Syndrome
- Infrared Thermal Imaging in Hemiplegic Patients of Upper Extremity by Stroke
- Complex Regional Pain Syndrome Type I after Stroke
- Musculoskeletal Problems in Upper Extremity after Stroke
- Application of Segmental Phase Angle for Assessment of Post-Stroke Complex Regional Pain Syndrome
