Ann Rehabil Med.
2018 Feb;42(1):166-174. 10.5535/arm.2018.42.1.166.
Rehabilitation of Advanced Cancer Patients in Palliative Care Unit
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Seoul Medical Center, Seoul, Korea. jongkyukim@seoulmc.or.kr
- 2Division of Medical Oncology and Hematology, Department of Internal Medicine, Seoul Medical Center, Seoul, Korea.
- 3Department of Family Medicine, Seoul Medical Center, Seoul, Korea.
- KMID: 2440982
- DOI: http://doi.org/10.5535/arm.2018.42.1.166
Abstract
OBJECTIVE
To evaluate the compliance and satisfaction of rehabilitation recommendations for advanced cancer patients hospitalized in the palliative care unit.
METHODS
Advanced cancer patients admitted to a hospice palliative care unit were recruited. Patients with advanced cancer and a life expectancy of less than 6 months, as assumed by the oncologist were included. Patients who were expected to die within 3 days were excluded. ECOG and Karnofsky performance scales, function ambulatory category, level of ambulation, and survival days were evaluated under the perspective of comprehensive rehabilitation. Problem-based rehabilitations were provided categorized as physical therapy at the gym, bedside physical therapy, physical modalities, medications and pain intervention. Investigation of compliance for each category was completed. Patient satisfaction was surveyed using a questionnaire.
RESULTS
Forty-five patients were recruited and received evaluations for rehabilitation perspective. The subjects were reported to have gait-related difficulties (71.1%), pain (68.9%), poor medical conditions (68.9%), bladder or bowel problems (44.4%), dysphagias (11.1%), mental status issues (11.1%), edemas (11.1%), spasticity (2.2%), and pressure sores (2.2%). In the t-test, patients with good compliance for GymPT showed higher survival days (p < 0.05). In the satisfaction survey, patients with performance scales showed a greater satisfaction in Spearman's correlation analysis (p < 0.05).
CONCLUSION
Advanced cancer patients admitted to the hospice palliative care unit have many rehabilitation needs. Patients with a longer survival time showed better compliance for GymPT. Patients with a better performance scale showed a higher satisfaction. Comprehensive rehabilitation may be needed to advanced cancer patients in the hospice palliative care unit.
Keyword
MeSH Terms
Figure
-
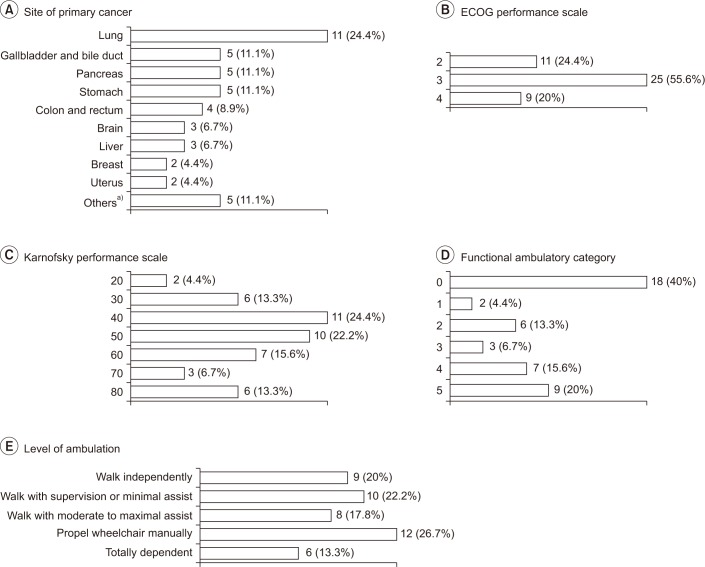
Fig. 1 Characteristics of included patients. (A) Site of primary cancer, (B) Eastern Cooperative Oncology Group (ECOG) performance scale, (C) Karnofsky performance scale, (D) Functional Ambulatory Category, and (E) level of ambulation. Others include ovary, esophagus, prostate, bone (osteosarcoma) and blood (leukemia).
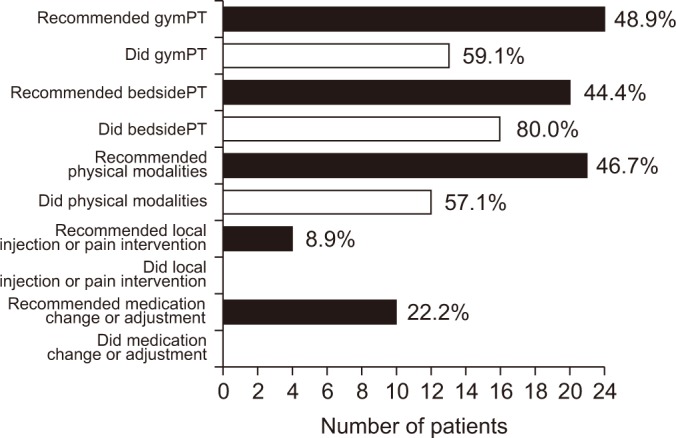
Fig. 2 Compliance of recommended rehabilitation approach.
Reference
-
1. Shin HY, Lee JY, Song J, Lee S, Lee J, Lim B, et al. Cause-of-death statistics in the Republic of Korea, 2014. J Korean Med Assoc. 2016; 59:221–232.
Article2. Jo JM, Hwang JH, Lee CH, Kang HJ, Yu JN. The need of cancer patients for rehabilitation services. J Korean Acad Rehabil Med. 2010; 34:691–700.3. Okamura H. Importance of rehabilitation in cancer treatment and palliative medicine. Jpn J Clin Oncol. 2011; 41:733–738. PMID: 21622762.
Article4. Lipsett A, Barrett S, Haruna F, Mustian K, O'Donovan A. The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: a systematic review and meta-analysis. Breast. 2017; 32:144–155. PMID: 28189100.
Article5. Carduff E, Kendall M, Murray SA. Living and dying with metastatic bowel cancer: serial in-depth interviews with patients. Eur J Cancer Care (Engl). 2017.
Article6. Dasch B, Kalies H, Feddersen B, Ruderer C, Hiddemann W, Bausewein C. Care of cancer patients at the end of life in a German university hospital: a retrospective observational study from 2014. PLoS One. 2017; 12:e0175124. PMID: 28384214.
Article7. Hartogh GD. Suffering and dying well: on the proper aim of palliative care. Med Health Care Philos. 2017; 20:413–424. PMID: 28374105.
Article8. Kanach FA, Brown LM, Campbell RR. The role of rehabilitation in palliative care services. Am J Phys Med Rehabil. 2014; 93:342–345. PMID: 24196973.
Article9. McIlfatrick S, Connolly M, Collins R, Murphy T, Johnston B, Larkin P. Evaluating a dignity care intervention for palliative care in the community setting: community nurses' perspectives. J Clin Nurs. 2017; 26:4300–4312. PMID: 28178386.
Article10. Eyigor S, Akdeniz S. Is exercise ignored in palliative cancer patients? World J Clin Oncol. 2014; 5:554–559. PMID: 25114869.
Article11. Talbot Rice H, Malcolm L, Norman K, Jones A, Lee K, Preston G, et al. An evaluation of the St Christopher's Hospice rehabilitation gym circuits classes: patient uptake, outcomes, and feedback. Prog Palliat Care. 2014; 22:319–325. PMID: 25414550.
Article12. Gerber LH. Cancer rehabilitation into the future. Cancer. 2001; 92(4 Suppl):975–979. PMID: 11519023.
Article13. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982; 5:649–655. PMID: 7165009.
Article14. Karnofsky DA, Abelmann WH, Craver LF, Burchenal JH. The use of the nitrogen mustards in the palliative treatment of carcinoma: with particular reference to bronchogenic carcinoma. Cancer. 1948; 1:634–656.15. Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl-Baker L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys Ther. 1984; 64:35–40. PMID: 6691052.16. DeLisa JA. A history of cancer rehabilitation. Cancer. 2001; 92(4 Suppl):970–974. PMID: 11519022.
Article17. Cheville A. Rehabilitation of patients with advanced cancer. Cancer. 2001; 92(4 Suppl):1039–1048. PMID: 11519031.
Article18. Jung HY. Impact and application of the internal classification functioning, disability and health in the medical rehabilitation. J Korean Acad Rehabil Med. 2004; 28:401–411.19. Abrahm JL, Banffy MB, Harris MB. Spinal cord compression in patients with advanced metastatic cancer: “all I care about is walking and living my life”. JAMA. 2008; 299:937–946. PMID: 18314436.20. Stubblefield MD, Keole N. Upper body pain and functional disorders in patients with breast cancer. PM R. 2014; 6:170–183. PMID: 24360839.
Article21. Stubblefield MD, Custodio CM. Upper-extremity pain disorders in breast cancer. Arch Phys Med Rehabil. 2006; 87(3 Suppl 1):S96–S99. PMID: 16500198.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Psychological Aspects of Care in Cancer Patients in the Last Weeks/Days of Life
- Management of Physical Symptoms in Patients with Advanced Cancer during the Last Weeks and Days of Life
- Understanding of Changes to Hospice & Palliative Care Brought by the Enforcement of the Act on Hospice & Palliative Care and Dying Patient Determination of Life Sustaining Treatments
- Policy on Hospice and Palliative Care in Korea
- Cases and Literature Review of Timing for Withdrawal of Palliative Chemotherapy
