Ann Dermatol.
2019 Apr;31(2):196-200. 10.5021/ad.2019.31.2.196.
Case Series of Morbihan Disease (Extreme Eyelid Oedema Associated with Rosacea): Diagnostic and Therapeutic Approaches
- Affiliations
-
- 1Department of Dermatology, Soonchunhyang University College of Medicine, Cheonan, Korea. dermsung@schmc.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 3Department of Dermatology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 4Department of Ophthalmology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- KMID: 2439065
- DOI: http://doi.org/10.5021/ad.2019.31.2.196
Abstract
- Morbihan disease (MD) is a rare form of rosacea that presents with chronic erythema and solid oedema on the upper half of the face. A diagnosis of MD can be made only after eliminating diseases that are similar in terms of clinical and histopathological presentation. The cause of MD remains unclear and no standardised treatment is yet available. MD often tends to be recalcitrant to therapies commonly used to treat rosacea, including systemic corticosteroids, antibiotics, isotretinoin, and topical regimens. Thus, surgical interventions have been attempted but most cases have exhibited unsatisfactory responses. We treated six patients with extreme eyelid lymphoedema without any other cutaneous manifestation. Surgical eyelid reduction was performed in all patients, because ptosis and narrowing of the visual field were the major complaints. Histopathological tests revealed various extents of perivascular and perifollicular inflammation, and dermal oedema. After surgery, patients with severe inflammatory cell infiltration (including mast cells) exhibited a tendency toward recurrence. Other patients with severe dermal oedema exhibited better responses to surgical reduction, and thus no recurrence. We propose that MD should be included in the differential diagnosis of persistent, chronic eyelid oedema even if eyelid oedema is the only manifestation; the histological features may aid in the selection of appropriate therapeutic strategies. We suggest that eyelid reduction surgery can be a useful treatment option for MD patients when there is no massive mast cell infiltration.
MeSH Terms
Figure
-
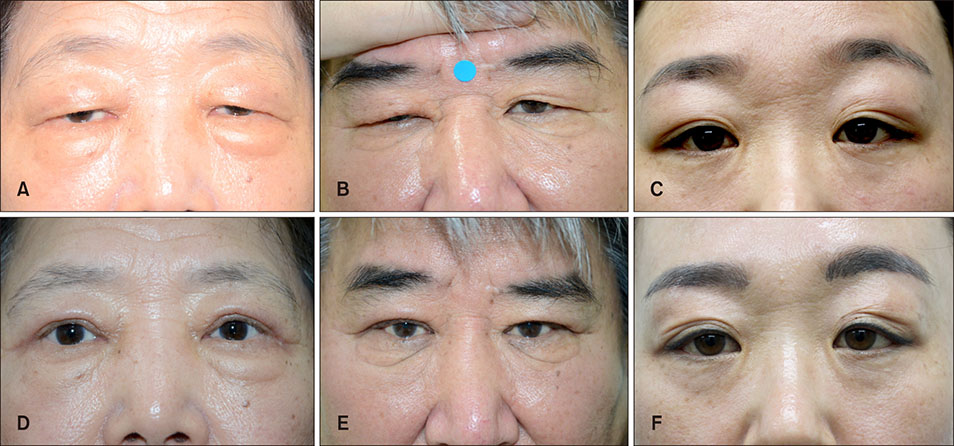
Fig. 1 Initial clinical presentation of patient 1 to 3. (A~C) Soft, non-pitting oedema without erythema on both eyelids. Clinical presentation after 6 months of surgical reduction of patient 1 to 3. (D~F) All showed marked improvement.
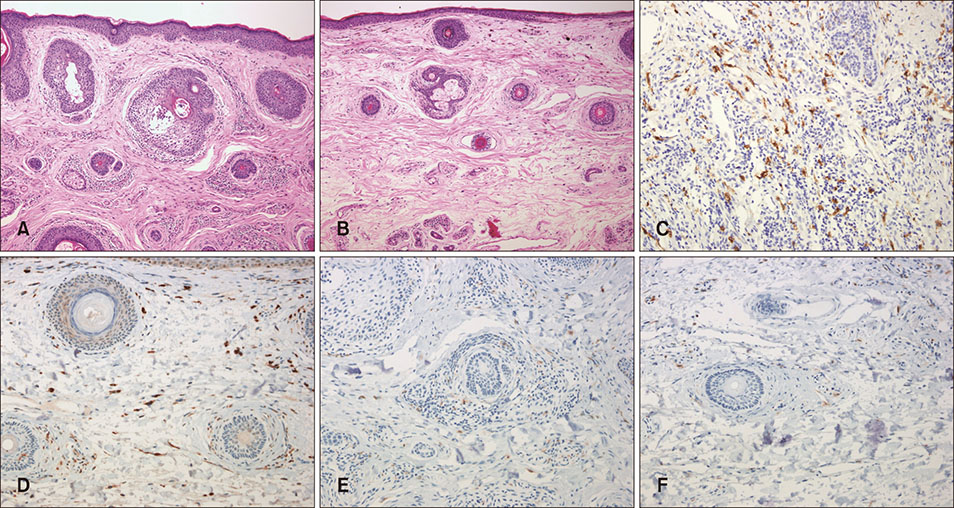
Fig. 2 On H&E staining, (A) perifollicular inflammation with minimal oedema of dermis in inflammatory type and (B) mild perifollicular inflammation in oedema type are found (H&E, ×100). (C) Immunohistochemistry (IHC) for CD117 shows the increased number of mast cell in inflammatory group, (D) comparing to those of odedma group (IHC, ×200). (E) The number of CD68-positive histiocyte is increased in inflammatory group than in (F) odema group (IHC, ×200).
Reference
-
1. Nagasaka T, Koyama T, Matsumura K, Chen KR. Persistent lymphoedema in Morbihan disease: formation of perilymphatic epithelioid cell granulomas as a possible pathogenesis. Clin Exp Dermatol. 2008; 33:764–767.
Article2. Degos R, Civatte J, Beuve-Méry M. Nouveau cas d’oedème érythémateux facial chronique. Bull Soc Fr Dermatol Syph. 1973; 80:257.3. Wohlrab J, Lueftl M, Marsch WC. Persistent erythema and edema of the midthird and upper aspect of the face (morbus morbihan): evidence of hidden immunologic contact urticaria and impaired lymphatic drainage. J Am Acad Dermatol. 2005; 52:595–602.
Article4. Lai TF, Leibovitch I, James C, Huilgol SC, Selva D. Rosacea lymphoedema of the eyelid. Acta Ophthalmol Scand. 2004; 82:765–767.
Article5. Okubo A, Takahashi K, Akasaka T, Amano H. Four cases of Morbihan disease successfully treated with doxycycline. J Dermatol. 2017; 44:713–716.
Article6. Jansen T, Plewig G. The treatment of rosaceous lymphoedema. Clin Exp Dermatol. 1997; 22:57.7. Mascarenhas NL, Wang Z, Chang YL, Di Nardo A. TRPV4 mediates mast cell activation in cathelicidin-induced rosacea inflammation. J Invest Dermatol. 2017; 137:972–975.
Article8. Aroni K, Tsagroni E, Kavantzas N, Patsouris E, Ioannidis E. A study of the pathogenesis of rosacea: how angiogenesis and mast cells may participate in a complex multifactorial process. Arch Dermatol Res. 2008; 300:125–131.
Article9. Crawford GH, Pelle MT, James WD. Rosacea: I. Etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004; 51:327–341.
Article10. Bernardini FP, Kersten RC, Khouri LM, Moin M, Kulwin DR, Mutasim DF. Chronic eyelid lymphedema and acne rosacea. Report of two cases. Ophthalmology. 2000; 107:2220–2223.11. Fujimoto N, Mitsuru M, Tanaka T. Successful treatment of Morbihan disease with long-term minocycline and its association with mast cell infiltration. Acta Derm Venereol. 2015; 95:368–369.
Article12. Kabuto M, Fujimoto N, Honda S, Tanaka T. Successful treatment with long-term use of minocycline for Morbihan disease showing mast cell infiltration: a second case report. J Dermatol. 2015; 42:827–828.
Article13. Shim WH, Jwa SW, Song M, Kim HS, Ko HC, Kim BS, et al. Morbihan disease: a rare variant of rosacea. Korean J Dermatol. 2012; 50:320–323.
