Comparison of Anterior Translation among Three Sternoclavicular Reconstruction Methods in Cadaver Study
- Affiliations
-
- 1Department of Orthopedic Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea. hjchung29@yonsei.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2438983
- DOI: http://doi.org/10.4055/jkoa.2017.52.2.178
Abstract
- PURPOSE
Currently, biomechanics and function comparison of the reconstruction of structures play important roles in the sternoclavicular joint stability is not much. In order to confirm the improvement in the functional aspects of the sternoclavicular joint after the three most widely used reconstruction methods, we measured the degree of anterior translation of the sternoclavicular joint after the operation using cadavers.
MATERIALS AND METHODS
We studied 24 sternoclavicular joints in the cadavers. First, we measured the anterior translation of the clavicle, which was compared with the sternum in 24 normal sternoclavicular joints. We divided the cadaver into three groups and performed each of the three current operations: figure of eight hamastring tendon reconstruction operation (Group 1), subclavius tendon reconstruction operation (Group 2), and hamstring tendon reconstruction operation (Group 3); then we compared the degree of anterior translation in each group. We did the measurement by adding 10 degrees to the glenohumeral joint each time from 0 degrees to 90 degrees.
RESULTS
In the normal joint, the clavicle was significantly ascended compared with the sternum. The Group 1 had a 1.68±0.25 mm anterior translation while the Group 2 had 1.81±0.23 mm and Group 3 had 2.8±0.58 mm (Group 1: p=0.004, Group 2: p=0.001, Group 3: p=0.002). The Group 1 showed a low ascending rate of up to 60 degrees, which showed no significant difference with that of the normal joint. However, after 60 degrees, the ascending rate showed a significant increase. In the case of Group 2, there was no significant difference with normal joint of up to 50 degrees. Group 3 showed significant anterior ascending from 20 degree.
CONCLUSION
Through measuring the anterior translation of subjects that underwent three representative sternoclavicular joint reconstructions, we found that the result from the Group 1 was most comparable normal translation of the sternoclavicular joint.
MeSH Terms
Figure
-

Figure 1 Five reflective bony markers were attached to the proximal and distal sternum and clavicle to recognize the axis. Vicon motion analysis system (Vicon Motion System, UK) with 6 cameras (MXT10 2 megapixel camera).

Figure 2 Drill two 3- to 4-mm diameter drill-holes for each sternum and clavicle. Pass a hamstring tendon through the holes in the sternum and clavicle in a figure 8 shape, then bind the hamstring tendon (Hamstring tendon figure of eight reconstruction).
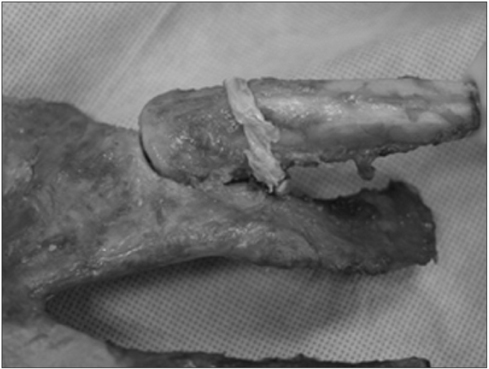
Figure 3 Start drilling in a superior to inferior direction in accordance with the position of the subclavius tendon. Impale the subclavius tendon in an inferior to superior direction at the drill hole and use one No. 2 Ethibond to suture up and bind subclavius tendon (subclavius tendon reconstruction).
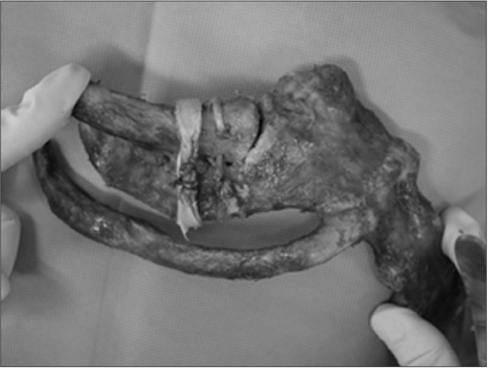
Figure 4 In a superior to inferior direction, use the drill to make a hole at the medial side of the clavicle and pass the hamstring tendon through the hole. Then, sling the hamstring tendon around the first rib while maintaining tight tension. Use No. 2 Ethibond to bind the hamstring tendon. The remaining tendon was used for a simple sling around the clavicle and the first rib at the outer radius of the reconstruction site (Hamstring tendon sling reconstruction).

Figure 5 Anterior translation of the clavicle during the coronal plane abduction of glenohumeral joint.
Reference
-
1. Gardner MA, Bidstrup BP. Intrathoracic great vessel injury resulting from blunt chest trauma associated with posterior dislocation of the sternoclavicular joint. Aust N Z J Surg. 1983; 53:427–430.
Article2. Jougon JB, Lepront DJ, Dromer CE. Posterior dislocation of the sternoclavicular joint leading to mediastinal compression. Ann Thorac Surg. 1996; 61:711–713.
Article3. Noda M, Shiraishi H, Mizuno K. Chronic posterior sternoclavicular dislocation causing compression of a subclavian artery. J Shoulder Elbow Surg. 1997; 6:564–569.
Article4. Ono K, Inagawa H, Kiyota K, Terada T, Suzuki S, Maekawa K. Posterior dislocation of the sternoclavicular joint with obstruction of the innominate vein: case report. J Trauma. 1998; 44:381–383.5. Rayan GM. Compression brachial plexopathy caused by chronic posterior dislocation of the sternoclavicular joint. J Okla State Med Assoc. 1994; 87:7–9.6. Southworth SR, Merritt TR. Asymptomatic innominate vein tamponade with retromanubrial clavicular dislocation. A case report. Orthop Rev. 1988; 17:789–791.7. Acus RW 3rd, Bell RH, Fisher DL. Proximal clavicle excision: an analysis of results. J Shoulder Elbow Surg. 1995; 4:182–187.
Article8. Barth E, Hagen R. Surgical treatment of dislocations of the sternoclavicular joint. Acta Orthop Scand. 1983; 54:746–747.
Article9. Booth CM, Roper BA. Chronic dislocation of the sternoclavicular joint: an operative repair. Clin Orthop Relat Res. 1979; (140):17–20.10. Brinker MR, Bartz RL, Reardon PR, Reardon MJ. A method for open reduction and internal fixation of the unstable posterior sternoclavicular joint dislocation. J Orthop Trauma. 1997; 11:378–381.
Article11. Cooper GJ, Stubbs D, Waller DA, Wilkinson GA, Saleh M. Posterior sternoclavicular dislocation: a novel method of external fixation. Injury. 1992; 23:565–566.
Article12. Eskola A, Vainionpää S, Vastamäki M, Slätis P, Rokkanen P. Operation for old sternoclavicular dislocation. Results in 12 cases. J Bone Joint Surg Br. 1989; 71:63–65.
Article13. Ferrandez L, Yubero J, Usabiaga J, No L, Martin F. Sternoclavicular dislocation. Treatment and complications. Ital J Orthop Traumatol. 1988; 14:349–355.14. Lunseth PA, Chapman KW, Frankel VH. Surgical treatment of chronic dislocation of the sterno-clavicular joint. J Bone Joint Surg Br. 1975; 57:193–196.
Article15. Martínez A, Rodríguez A, González G, Herrera A, Domingo J. Atraumatic spontaneous posterior subluxation of the sternoclavicular joint. Arch Orthop Trauma Surg. 1999; 119:344–346.
Article16. Rockwood CA Jr, Groh GI, Wirth MA, Grassi FA. Resection arthroplasty of the sternoclavicular joint. J Bone Joint Surg Am. 1997; 79:387–393.
Article17. Burrows HJ. Tenodesis of subclavius in the treatment of recurrent dislocation of the sterno-clavicular joint. J Bone Joint Surg Br. 1951; 33B:240–243.
Article18. Reilly P, Bruguera JA, Copeland SA. Erosion and nonunion of the first rib after sternoclavicular reconstruction with Dacron. J Shoulder Elbow Surg. 1999; 8:76–78.
Article19. Spencer EE, Kuhn JE, Huston LJ, Carpenter JE, Hughes RE. Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg. 2002; 11:43–47.
Article20. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion–Part II: shoulder, elbow, wrist and hand. J Biomech. 2005; 38:981–992.
Article21. Ribo M, Pinz A, Fuhrmann AL. A new optical tracking system for virtual and augmented reality applications. Paper presented at: IEEE Instrumentation and Measurement Technology Conference. 2001 May 21-23; Budapest, Hungary.22. Leighton RK, Buhr AJ, Sinclair AM. Posterior sternoclavicular dislocations. Can J Surg. 1986; 29:104–106.23. Clark RL, Milgram JW, Yawn DH. Fatal aortic perforation and cardiac tamponade due to a Kirschner wire migrating from the right sternoclavicular joint. South Med J. 1974; 67:316–318.
Article24. Ferrández L, Usabiaga J, Ramos L, Yubero J, No L. Migration of Kirschner wires into the mediastinum after stabilization of sterno-clavicular lesions. A report of two cases. Chir Organi Mov. 1991; 76:301–304.25. Janssens de Varebeke B, Van Osselaer G. Migration of Kirschner's pin from the right sternoclavicular joint resulting in perforation of the pulmonary artery main trunk. Acta Chir Belg. 1993; 93:287–291.26. Lyons FA, Rockwood CA Jr. Migration of pins used in operations on the shoulder. J Bone Joint Surg Am. 1990; 72:1262–1267.
Article27. Pate JW, Wilhite JL. Migration of a foreign body from the sternoclavicular joint to the heart: a case report. Am Surg. 1969; 35:448–449.28. Smolle-Juettner FM, Hofer PH, Pinter H, Friehs G, Szyskowitz R. Intracardiac malpositioning of a sternoclavicular fixation wire. J Orthop Trauma. 1992; 6:102–105.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Traumatic Sternoclavicular Joint Anterior Dislocation with a Sternal Fracture
- Posterior Sternoclavicular Dislocation: A Case Report
- Traumatic Posterior Dislocation of the Sternoclavicular Joint: A case Report
- Treatment of Traumatic Posterior Dislocation of the Sternoclavicular Joint: A Case Report
- Anatomical versus Non-Anatomical Single Bundle Anterior Cruciate Ligament Reconstruction: A Cadaveric Study of Comparison of Knee Stability
