Intraoperative and Postoperative Complications after Arthroscopic Coracoclavicular Stabilization
- Affiliations
-
- 1Department of Orthopaedic Surgery, Eulji Hospital, Eulji University School of Medicine, Seoul, Korea. 20140149@eulji.ac.kr
- KMID: 2438340
- DOI: http://doi.org/10.4055/cios.2019.11.1.103
Abstract
- BACKGROUND
Arthroscopic stabilization of torn coracoclavicular (CC) ligaments gained popularity recently. However, loss of reduction after the operation and complications unique to this technique involving tunnel placement through the distal clavicle and coracoid process are concerns. The purpose of this study was to report intraoperative and early postoperative complications associated with this procedure.
METHODS
This study retrospectively evaluated 18 consecutive patients who had undergone arthroscopic stabilization for torn CC ligaments between 2014 and 2015. The indications for surgery were acute or chronic acromioclavicular dislocation and acute fracture of the distal clavicle, associated with CC ligament disruption. Clinical outcomes were evaluated with the American Shoulder and Elbow Surgeons (ASES) and the University of California, Los Angeles (UCLA) scores. Intra- and postoperative complications and reoperations were investigated.
RESULTS
There were six female and 12 male patients with a mean age of 47 years (range, 22 to 86 years). At a mean follow-up of 17 ± 10 months (range, 10 to 28 months), the mean ASES score was 88.8 ± 19.9 and the mean UCLA score was 30.9 ± 5.2. Intraoperatively, seven complications developed: breach of lateral cortex of the coracoid process in five patients, medial cortex of the coracoid process in one, and anterior cortex of the clavicle in one. Postoperative complications developed in eight patients: four ossifications of the CC interspace, four tunnel widening of the clavicle, one bony erosion on the clavicle, and one superficial infection. A loss of reduction was found in six patients. Reoperation was performed in three patients for loss of reduction in two and superficial infection in the other.
CONCLUSIONS
Arthroscopic CC stabilization resulted in high rates of intraoperative and early postoperative complications. Most of them were related to the surgical technique involving bone tunnel placement in the coracoid process and the clavicle.
MeSH Terms
Figure
-

Fig. 1 (A) Arthroscopic coracoclavicular stabilization of the left shoulder in a 27-year-old male patient, viewing from posterior portal. A guide pin was drilled in the center and base of the inferior surface in the coracoid process. (B) The tunnel was made with a 4.0-mm cannulated reamer, and a suture was passed for shuttle relay though the reamer. The cortical button and FiberTape sutures were prepared before fixation (C) and properly placed on the subcoracoidal location (D).
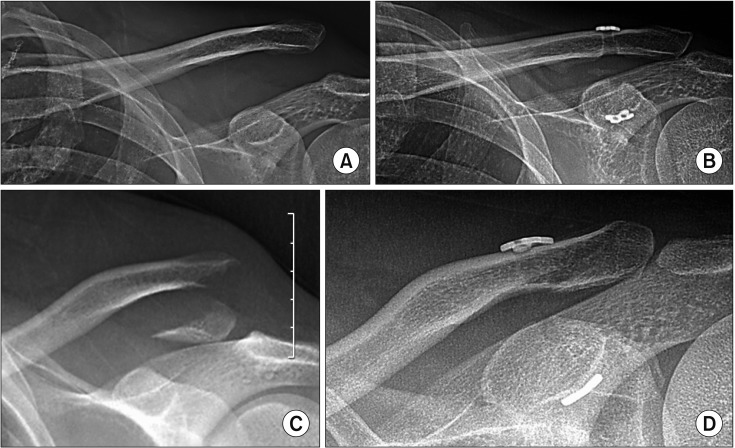
Fig. 2 Preoperative (A) and 24-month postoperative (B) radiographs of a 27-year-old patient with acromioclavicular dislocation of the left shoulder (Rockwood classification, type 5). Preoperative (C) and 6-month postoperative (D) radiographs of a 45-year-old male patient with a distal clavicle fracture of the left shoulder (Neer classification, type IIB).
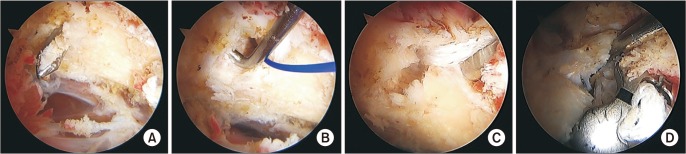
Fig. 3 (A) Arthroscopic image of the right shoulder in a 24-year-old female patient, viewing from posterior portal. A drill guide seemed to be placed properly into the base and center of the inferior surface in the coracoid process; however, lateral cortex breach of the coracoid process occurred after reaming (B) and the bone tunnel was further damaged during pull-out of the FiberTape sutures (C). (D) Arthroscopic image of the right shoulder of a 57-year-old female patient showing lateral cortex breach after placement of the cortical button and sutures.
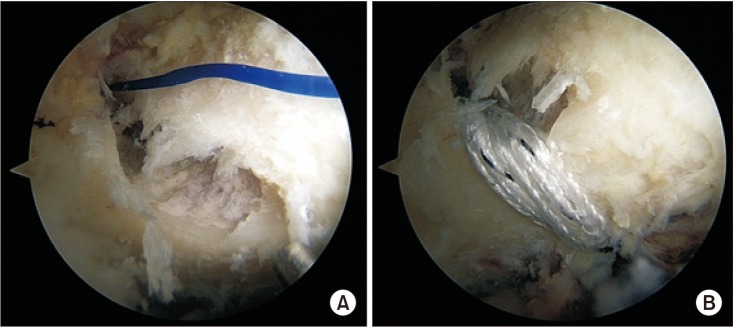
Fig. 4 Arthroscopic images of the right shoulder of a 28-year-old male patient, viewing from the posterior portal. (A) A lateral cortex breach occurred during reaming. (B) The fixation method was converted to the coracoid loop technique where the FiberTape was looped below the coracoid process instead of being passed through the coracoid bone tunnel.
Reference
-
1. Bosworth BM. Complete acromioclavicular dislocation. N Engl J Med. 1949; 241(6):221–225. PMID: 18138673.
Article2. Balog TP, Min KS, Rumley JC, Wilson DJ, Arrington ED. Arthroscopic anatomic coracoclavicular ligament repair using a 6-strand polyester suture tape and cortical button construct. Arthrosc Tech. 2015; 4(6):e757–e761. PMID: 27284507.
Article3. Pennington WT, Hergan DJ, Bartz BA. Arthroscopic coracoclavicular ligament reconstruction using biologic and suture fixation. Arthroscopy. 2007; 23(7):785. PMID: 17637416.
Article4. Scheibel M, Ifesanya A, Pauly S, Haas NP. Arthroscopically assisted coracoclavicular ligament reconstruction for chronic acromioclavicular joint instability. Arch Orthop Trauma Surg. 2008; 128(11):1327–1333. PMID: 18087706.
Article5. Shin SJ, Jeon YS, Kim RG. Arthroscopic-assisted coracoclavicular ligament reconstruction for acute acromioclavicular dislocation using 2 clavicular and 1 coracoid cortical fixation buttons with suture tapes. Arthroscopy. 2017; 33(8):1458–1466. PMID: 28427871.
Article6. Blake MH, Lu MT, Shulman BS, Glaser DL, Huffman GR. Arthroscopic cortical button stabilization of isolated acute Neer type II fractures of the distal clavicle. Orthopedics. 2017; 40(6):e1050–e1054. PMID: 28968475.
Article7. Cook JB, Shaha JS, Rowles DJ, Bottoni CR, Shaha SH, Tokish JM. Early failures with single clavicular transosseous coracoclavicular ligament reconstruction. J Shoulder Elbow Surg. 2012; 21(12):1746–1752. PMID: 22521387.
Article8. Shin SJ, Kim NK. Complications after arthroscopic coracoclavicular reconstruction using a single adjustable-looplength suspensory fixation device in acute acromioclavicular joint dislocation. Arthroscopy. 2015; 31(5):816–824. PMID: 25543250.
Article9. Choi NH, Lim SM, Lee SY, Lim TK. Loss of reduction and complications of coracoclavicular ligament reconstruction with autogenous tendon graft in acute acromioclavicular dislocations. J Shoulder Elbow Surg. 2017; 26(4):692–698. PMID: 27765500.
Article10. Martetschlager F, Horan MP, Warth RJ, Millett PJ. Complications after anatomic fixation and reconstruction of the coracoclavicular ligaments. Am J Sports Med. 2013; 41(12):2896–2903. PMID: 24007761.
Article11. Milewski MD, Tompkins M, Giugale JM, Carson EW, Miller MD, Diduch DR. Complications related to anatomic reconstruction of the coracoclavicular ligaments. Am J Sports Med. 2012; 40(7):1628–1634. PMID: 22553116.
Article12. Parnes N, Blevins M, Carey P, Carr B. Arthroscopic reconstruction of the coracoclavicular ligaments using a coracoid cerclage technique. Arthrosc Tech. 2016; 5(2):e241–e246. PMID: 27330946.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long-term clinical and radiographic outcomes of arthroscopic acromioclavicular stabilization for acute acromioclavicular joint dislocation
- Current Concepts in Arthroscopic Treatment of Anterior Shoulder Instability
- Arthroscopic Latarjet procedure: current concepts and surgical techniques
- Arthroscopic Stabilization for Displaced Lateral Clavicular Fractures: Can It Restore Anatomy?
- Treatment of Complete Acromioclavicular Separation by Coracoclavicular Wiring
