Assessment of Left Ventricular Myocardial Diseases with Cardiac Computed Tomography
- Affiliations
-
- 1Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. ksm9723@yahoo.co.kr
- 2Department of Radiology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Radiology, Dongsan Medical Center, Keimyung University College of Medicine, Daegu, Korea.
- 5Department of Radiology, Korea University Anam Hospital, Seoul, Korea.
- KMID: 2438264
- DOI: http://doi.org/10.3348/kjr.2018.0280
Abstract
- Rapid advances in cardiac computed tomography (CT) have enabled the characterization of left ventricular (LV) myocardial diseases based on LV anatomical morphology, function, density, and enhancement pattern. Global LV function and regional wall motion can be evaluated using multi-phasic cine CT images. CT myocardial perfusion imaging facilitates the identification of hemodynamically significant coronary artery disease. CT delayed-enhancement imaging is used to detect myocardial scar in myocardial infarction and to measure the extracellular volume fraction in non-ischemic cardiomyopathy. Multi-energy cardiac CT allows the mapping of iodine distribution in the myocardium. This review summarizes the current techniques of cardiac CT for LV myocardial assessment, highlights the key findings in various myocardial diseases, and presents future applications to complement echocardiography and cardiovascular magnetic resonance.
MeSH Terms
Figure
-
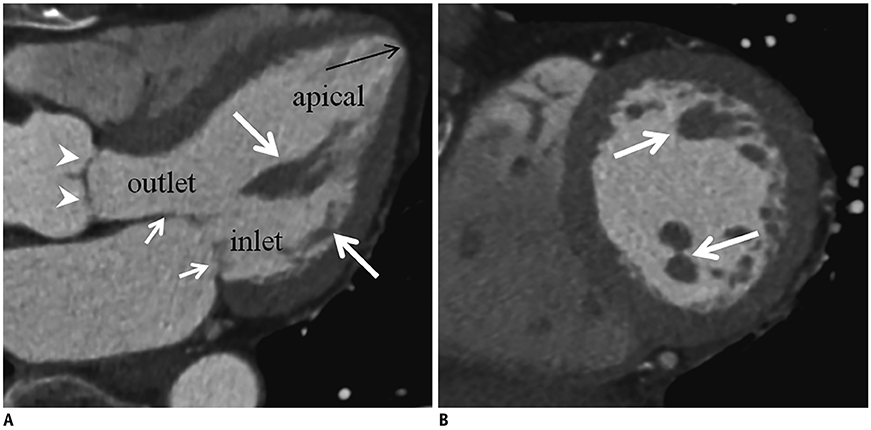
Fig. 1 Anatomy of left ventricle. Three-chamber (A) and short-axis (B) MPR CCT images show mitral valve (short arrows), aortic valve (arrowheads), papillary muscles (thick arrows), and apical thinning (long arrow). Left ventricle is divided into three portions: inlet, apical, and outlet. Short-axis MPR image (B) is obtained at midventricular level. CCT = cardiac computed tomography, MPR = multiplanar reformat

Fig. 2 Changes in LV wall thickness during mid- and end-diastole. Wall thickness and chamber dimension of left ventricle need precise measurements, usually in end-diastole. Most CCT is performed in mid-diastole to evaluate coronary artery. Interpretation of LV wall thickness may be misleading in mid-diastole (A) compared with that in end-diastole (B). LV = left ventricular

Fig. 3 Infarct imaging using first pass and delayed-enhancement CCT in patient with acute MI in left circumflex territory. Short-axis MPR images of first pass (A) and delayed enhancement (B) show fixed subendocardial perfusion defect (arrows) and delayed transmural hyperenhancement (arrowheads) in mid-lateral LV wall. Curved MPR coronary CT angiography image (C) shows acute thrombotic occlusion (arrows) of proximal left circumflex artery. Subendocardial perfusion defect indicates microvascular occlusion and poor prognosis. MI = myocardial infarction

Fig. 4 Global and regional LV function assessment with CCT in 51-year-old man with previous MI. Precontrast CCT image (A) shows curvilinear fat deposition in subendocardium of LV myocardium (arrowheads). Short-axis MPR CCT images obtained during end-systole (B) and end-diastole (C) show akinesia, curvilinear fat deposition in subendocardium (arrowheads), and thinned myocardium (5 mm in thickness) in mid-anterior and anteroseptal LV wall (arrows). LV ejection fraction, end-diastolic, and end-systolic volumes were 57%, 137 mL, and 59 mL, respectively.
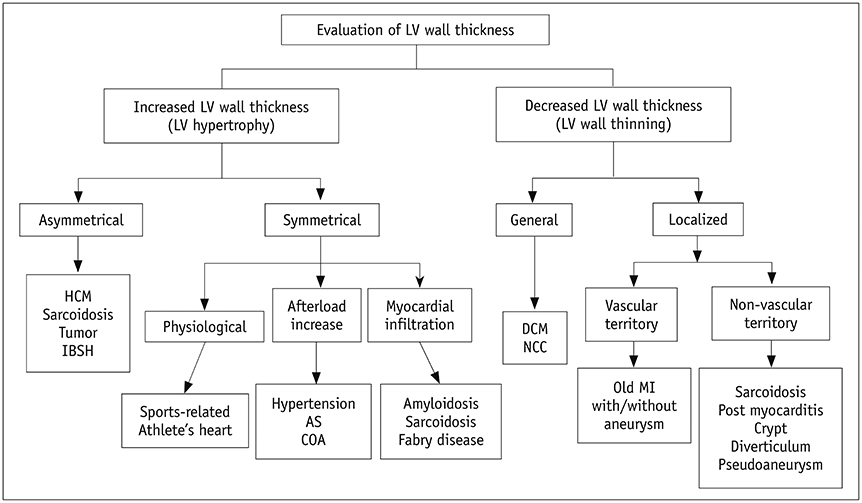
Fig. 5 Diagnostic approach based on LV wall thickness using CCT. AS = aortic stenosis, COA = coarctation of aorta, DCM = dilated cardiomyopathy, HCM = hypertrophic cardiomyopathy, IBSH = isolated basal septal hypertrophy, NCC = non-compaction cardiomyopathy
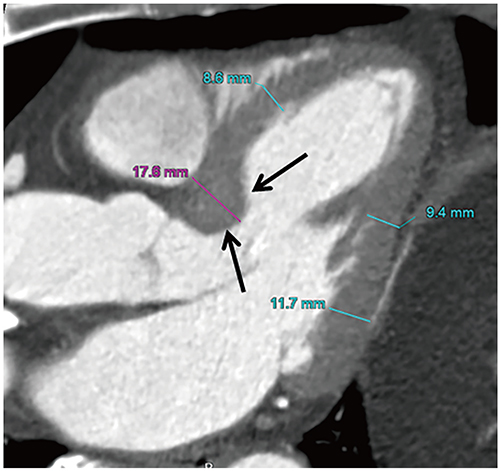
Fig. 6 IBSH of 67-year-old man with diabetes mellitus without hypertension. Three-chamber MPR CCT image shows focal hypertrophy of basal inter-ventricular septum (arrows) without hypertrophy elsewhere within myocardium in mid-diastole on LV outflow tract.
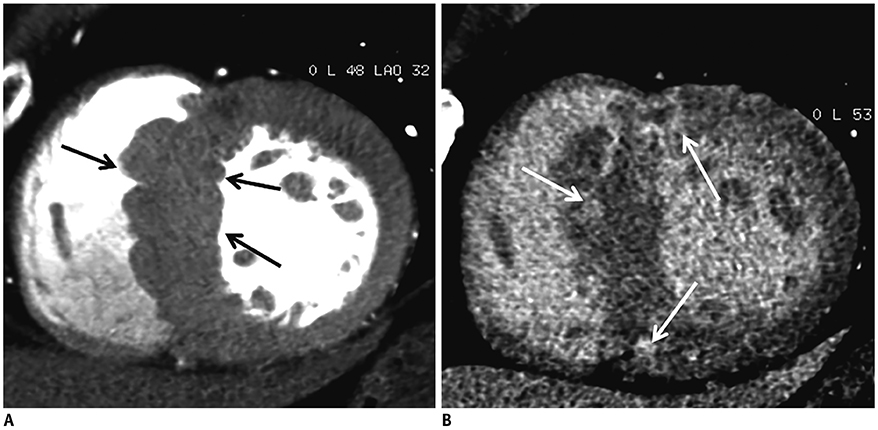
Fig. 7 HCM in 57-year-old man with chest pain. Short-axis MPR CCT images obtained during early (A) and delayed (B) contrast-enhancement phases show asymmetrical hypertrophy of mid anterior, anteroseptal, and anterolateral LV wall (A, arrows) in mid-diastole with multifocal mid-wall delayed enhancement (B, arrows).
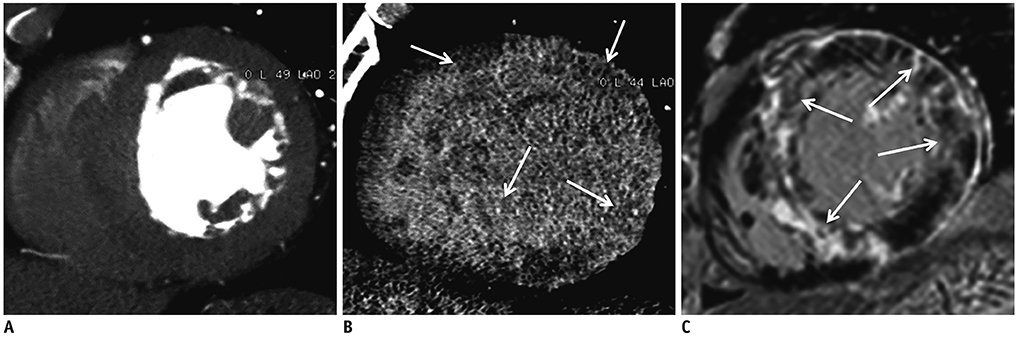
Fig. 8 Cardiac sarcoidosis in 61-year-old woman with irregular cardiac rhythm and dyspnea. Short-axis MPR CCT images obtained during early (A) and delayed (B) contrast-enhancement phases show concentrically hypertrophied mid-LV wall in mid-diastole with diffuse transmural and mesocardial delayed enhancement (arrows). Delayed-enhancement CMR image (C) shows diffuse mesocardial enhancement in septum and multifocal patchy mesocardial enhancement in mid anterior, lateral, and inferior LV wall (arrows). Delayed-enhancement CMR is superior to delayed-enhancement CCT for differentiating patterns of delayed myocardial enhancement. CMR = cardiovascular magnetic resonance

Fig. 9 LV metastasis from lung cancer in 93-year-old man. Contrast-enhanced chest CT image (A) shows 13-mm lobulated nodule with heterogeneous enhancement in anterior segment of left lower lobe (arrow). Mid-diastolic short-axis MPR CCT image (B) shows large infiltrating mass with homogeneous hypoenhancement as focal hypertrophied mid inferoseptal and inferior LV wall (arrows).

Fig. 10 Severe aortic valve stenosis in 79-year-old man with chest discomfort and shortness of breath. Double oblique MPR image of aortic valve (A) shows thickened and calcified cusps (arrowheads) of tricuspid aortic valve with severely reduced opening (aortic valve area of 0.98 cm2) during early-systole. Short-axis MPR image (B) shows hypertrophied mid-LV wall, particularly asymmetric septal hypertrophy (arrows). Delayed-enhancement CCT image (C) shows extensive mesocardial delayed hyperenhancement in middle LV wall (arrows).

Fig. 11 Cardiac amyloidosis in 74-year-old male who presented with chest pain. Four-chamber MPR delayed enhancement image obtained during mid-diastole shows hypertrophy of LV myocardial wall and diffuse, concentric subendocardial and transmural enhancement (arrowheads) in LV myocardial wall. Case courtesy of HJ Lee, Yonsei University Severance Hospital.

Fig. 12 DCM in 63-year-old man. Four-chamber MPR image (A) obtained during end-diastole shows all cardiac chamber dilatation. Short-axis MPR CCT images obtained during end-systole (B) and end-diastole (C) show LV dilation, thinned myocardium (5 mm in thickness), and global severe hypokinesia. LV ejection fraction, end-diastolic, and end-systolic volumes were 12%, 137 mL, and 59 mL, respectively.
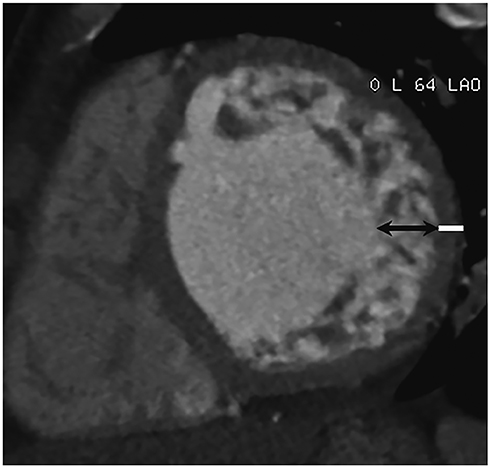
Fig. 13 NCC in 48-year-old woman with dyspnea and cough pain. End-diastolic short-axis MPR image shows increased thickness of noncompacted layer in anterior, lateral, and inferior segments of mid-LV wall with ratio of noncompacted (black arrow, 15 mm in thickness) to compacted myocardium (white line, 6 mm in thickness) > 2.3:1.
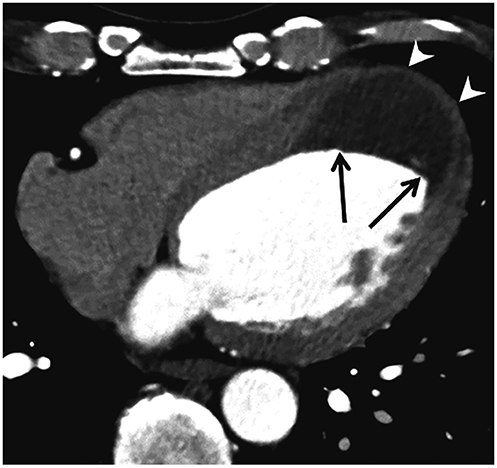
Fig. 14 LV aneurysm with intracavitary thrombus in 53-year-old man with chronic MI. Axial CCT image shows thin-walled apical aneurysm (arrowheads) and extensive intracavitary thrombus formation (arrows).
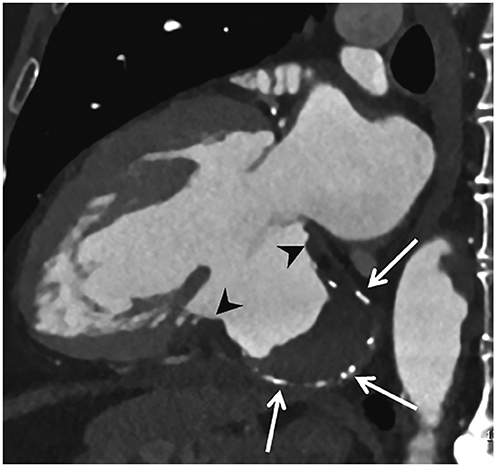
Fig. 15 LV pseudoaneurysm in 65-year-old man with stable angina. Two-chamber MPR CCT image shows LV inferior wall outpouching with relatively narrow neck (arrowheads), intracavitary thrombus (arrows), and multiple calcifications along its wall.
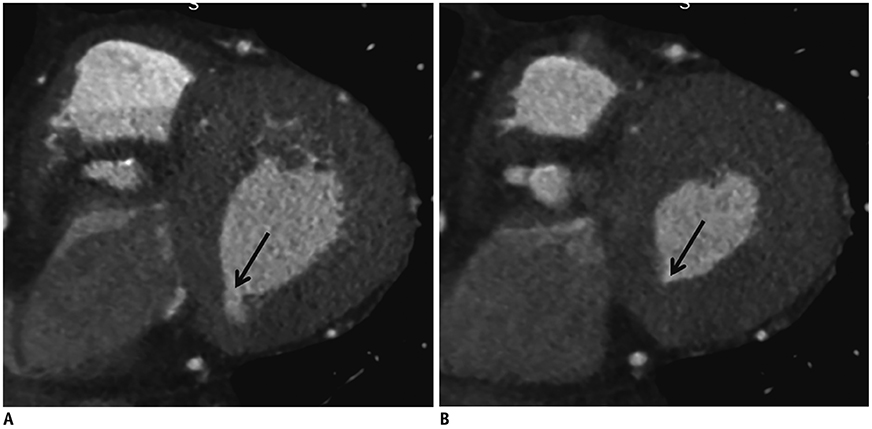
Fig. 16 LV crypt in 68-year-old man with HCM. End-diastolic (A) and end-systolic short-axis (B) MPR CCT images show sharp-edged disruption of normal compacted myocardium penetrating basal inferior LV wall (A, arrow) with near complete obliteration during end-systole (B, arrow).
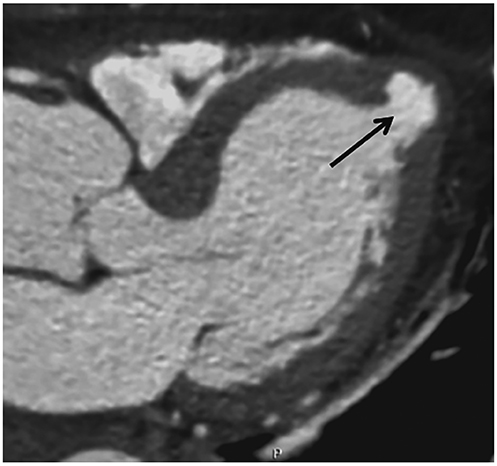
Fig. 17 V diverticulum. Three-chamber MPR CCT image shows finger or hook-like pouch of entire LV myocardial wall (arrow) arising from LV apex in mid-diastole.

Fig. 18 Myocarditis in 69-year-old man with dyspnea for 10 days. Initial chest CT (A) shows hypoenhancement in apical to mid interventricular septum (arrows) with preserved myocardial thickness. Short-axis MPR CCT image (B) obtained 3 weeks later shows thinned myocardium at anterior, septal, and inferior segments of middle LV wall (arrows). Delayed-enhancement cardiac magnetic resonance image (C) obtained 5 weeks later shows transmural hyperenhancement at mid-anterior and septal LV wall and subendocardial hyperenhancement at middle inferior LV wall (arrows).

Fig. 19 Nonspecific myocardial fat in 51-year-old woman without cardiac symptoms. Axial precontrast CCT image shows fat (arrow) in LV apical septum.
Reference
-
1. Clayton B, Roobottom C, Morgan-Hughes G. Assessment of the myocardium with cardiac computed tomography. Eur Heart J Cardiovasc Imaging. 2014; 15:603–609.
Article2. Prasad K, Atherton J, Smith GC, McKenna WJ, Frenneaux MP, Nihoyannopoulos P. Echocardiographic pitfalls in the diagnosis of hypertrophic cardiomyopathy. Heart. 1999; 82:suppl 3. III8–III15.
Article3. Patel AR, Kramer CM. Role of cardiac magnetic resonance in the diagnosis and prognosis of nonischemic cardiomyopathy. JACC Cardiovasc Imaging. 2017; 10:1180–1193.4. Captur G, Manisty C, Moon JC. Cardiac MRI evaluation of myocardial disease. Heart. 2016; 102:1429–1435.
Article5. Machida H, Tanaka I, Fukui R, Shen Y, Ishikawa T, Tate E, et al. Current and novel imaging techniques in coronary CT. Radiographics. 2015; 35:991–1010.
Article6. Treibel TA, Bandula S, Fontana M, White SK, Gilbertson JA, Herrey AS, et al. Extracellular volume quantification by dynamic equilibrium cardiac computed tomography incardiac amyloidosis. J Cardiovasc Comput Tomogr. 2015; 9:585–592.7. Ho SY. Anatomy and myoarchitecture of the left ventricular wall in normal and in disease. Eur J Echocardiogr. 2009; 10:iii3–iii7.
Article8. Sengupta PP, Korinek J, Belohlavek M, Narula J, Vannan MA, Jahangir A, et al. Left ventricular structure and function: basic science for cardiac imaging. J Am Coll Cardiol. 2006; 48:1988–2001.9. O'Brien JP, Srichai MB, Hecht EM, Kim DC, Jacobs JE. Anatomy of the heart at multidetector CT: what the radiologist needs to know. Radiographics. 2007; 27:1569–1582.10. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the cardiac imaging committee of the council on clinical cardiology of the American Heart Association. Circulation. 2002; 105:539–554.
Article11. Kim YJ, Yong HS, Kim SM, Kim JA, Yang DH, Hong YJ, et al. Korean guidelines for the appropriate use of cardiac CT. Korean J Radiol. 2015; 16:251–285.
Article12. ASCI Practice Guideline Working Group. Beck KS, Kim JA, Choe YH, Hian SK, Hoe J, et al. 2017 multimodality appropriate use criteria for noninvasive cardiac imaging: expert consensus of the Asian Society of Cardiovascular Imaging. Korean J Radiol. 2017; 18:871–880.
Article13. Sato A, Aonuma K. Role of cardiac multidetector computed tomography beyond coronary angiography. Circ J. 2015; 79:712–720.
Article14. Abbara S, Blanke P, Maroules CD, Cheezum M, Choi AD, Han BK, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: a report of the society of cardiovascular computed tomography guidelines committee: endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016; 10:435–449.15. Bischoff B, Bamberg F, Marcus R, Schwarz F, Becker HC, Becker A, et al. Optimal timing for first-pass stress CT myocardial perfusion imaging. Int J Cardiovasc Imaging. 2013; 29:435–442.
Article16. Rossi A, Merkus D, Klotz E, Mollet N, de Feyter PJ, Krestin GP. Stress myocardial perfusion: imaging with multidetector CT. Radiology. 2014; 270:25–46.
Article17. Yang DH, Kim YH, Roh JH, Kang JW, Han D, Jung J, et al. Stress myocardial perfusion CT in patients suspected of having coronary artery disease: visual and quantitative analysis-validation by using fractional flow reserve. Radiology. 2015; 276:715–723.
Article18. Rossi A, Dharampal A, Wragg A, Davies LC, van Geuns RJ, Anagnostopoulos C, et al. Diagnostic performance of hyperaemic myocardial blood flow index obtained by dynamic computed tomography: does it predict functionally significant coronary lesions? Eur Heart J Cardiovasc Imaging. 2014; 15:85–94.
Article19. Ko SM, Kim YW, Han SW, Seo JB. Early and delayed myocardial enhancement in myocardial infarction using two-phase contrast-enhanced multidetector-row CT. Korean J Radiol. 2007; 8:94–102.
Article20. Lardo AC, Cordeiro MA, Silva C, Amado LC, George RT, Saliaris AP, et al. Contrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scar. Circulation. 2006; 113:394–404.21. Deseive S, Bauer RW, Lehmann R, Kettner M, Kaiser C, Korkusuz H, et al. Dual-energy computed tomography for the detection of late enhancement in reperfused chronic infarction: a comparison to magnetic resonance imaging and histopathology in a porcine model. Invest Radiol. 2011; 46:450–456.22. Mahnken AH, Koos R, Katoh M, Wildberger JE, Spuentrup E, Buecker A, et al. Assessment of myocardial viability in reperfused acute myocardial infarction using 16-slice computed tomography in comparison to magnetic resonance imaging. J Am Coll Cardiol. 2005; 45:2042–2047.
Article23. Gerber BL, Belge B, Legros GJ, Lim P, Poncelet A, Pasquet A, et al. Characterization of acute and chronic myocardial infarcts by multidetector computed tomography: comparison with contrast-enhanced magnetic resonance. Circulation. 2006; 113:823–833.24. Bandula S, White SK, Flett AS, Lawrence D, Pugliese F, Ashworth MT, et al. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: validation against histologic findings. Radiology. 2013; 269:396–403.
Article25. Lee HJ, Im DJ, Youn JC, Chang S, Suh YJ, Hong YJ, et al. Myocardial extracellular volume fraction with dual-energy equilibrium contrast-enhanced cardiac CT in nonischemic cardiomyopathy: a prospective comparison with cardiac MR imaging. Radiology. 2016; 280:49–57.
Article26. McCollough CH, Leng S, Yu L, Fletcher JG. Dual- and multi-energy CT: principles, technical approaches, and clinical applications. Radiology. 2015; 276:637–653.
Article27. Kalisz K, Halliburton S, Abbara S, Leipsic JA, Albrecht MH, Schoepf UJ, et al. Update on cardiovascular applications of multienergy CT. Radiographics. 2017; 37:1955–1974.
Article28. Ko SM, Song MG, Chee HK, Hwang HK, Feuchtner GM, Min JK. Diagnostic performance of dual-energy CT stress myocardial perfusion imaging: direct comparison with cardiovascular MRI. AJR Am J Roentgenol. 2014; 203:W605–W613.
Article29. Asferg C, Usinger L, Kristensen TS, Abdulla J. Accuracy of multi-slice computed tomography for measurement of left for measurement of left ventricular ejection compared with cardiac magnetic resonance imaging and two-dimensional transthoracic echocardiography: a systematic review and meta-analysis. Eur J Radiol. 2012; 81:e757–e762.30. Kang EJ, Lee KN, Choi WJ, Kim YD, Shin KM, Lim JK, et al. Left ventricular functional parameters and geometric patterns in Korean adults on coronary CT angiography with a 320-detector-row CT scanner. Korean J Radiol. 2017; 18:664–673.
Article31. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015; 16:233–271.
Article32. Barbieri A, Bursi F, Mantovani F, Valenti C, Quaglia M, Berti E, et al. Left ventricular hypertrophy reclassification and death: application of the recommendation of the American Society of Echocardiography/European Association of Echocardiography. Eur Heart J Cardiovasc Imaging. 2012; 13:109–117.
Article33. Alkema M, Spitzer E, Soliman OI, Loewe C. Multimodality imaging for left ventricular hypertrophy severity grading: a methodological review. J Cardiovasc Ultrasound. 2016; 24:257–267.
Article34. Kelshiker MA, Mayet J, Unsworth B, Okonko DO. Basal septal hypertrophy. Curr Cardiol Rev. 2013; 9:325–330.
Article35. Ranasinghe I, Ayoub C, Cheruvu C, Freedman SB, Yiannikas J. Isolated hypertrophy of the basal ventricular septum: characteristics of patients with and without outflow tract obstruction. Int J Cardiol. 2014; 173:487–493.
Article36. Gaudron PD, Liu D, Scholz F, Hu K, Florescu C, Herrmann S, et al. The septal bulge--an early echocardiographic sign in hypertensive heart disease. J Am Soc Hypertens. 2016; 10:70–80.
Article37. Cardim N, Galderisi M, Edvardsen T, Plein S, Popescu BA, D'Andrea A, et al. Role of multimodality cardiac imaging in the management of patients with hypertrophic cardiomyopathy: an expert consensus of the European Association of Cardiovascular Imaging Endorsed by the Saudi Heart Association. Eur Heart J Cardiovasc Imaging. 2015; 16:280.
Article38. Biagini E, Coccolo F, Ferlito M, Perugini E, Rocchi G, Bacchi-Reggiani L, et al. Dilated-hypokinetic evolution of hypertrophic cardiomyopathy: prevalence, incidence, risk factors, and prognostic implications in pediatric and adult patients. J Am Coll Cardiol. 2005; 46:1543–1550.39. Harris KM, Spirito P, Maron MS, Zenovich AG, Formisano F, Lesser JR, et al. Prevalence, clinical profile, and significance of left ventricular remodeling in the end-stage phase of hypertrophic cardiomyopathy. Circulation. 2006; 114:216–225.
Article40. Olivotto I, Gistri R, Petrone P, Pedemonte E, Vargiu D, Cecchi F. Maximum left ventricular thickness and risk of sudden death in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003; 41:315–321.
Article41. Kim SS, Ko SM, Choi SI, Choi BH, Stillman AE. Sudden cardiac death from structural heart diseases in adults: imaging findings with cardiovascular computed tomography and magnetic resonance. Int J Cardiovasc Imaging. 2016; 32:Suppl 1. 21–43.
Article42. Chun EJ, Choi SI, Jin KN, Kwag HJ, Kim YJ, Choi BW, et al. Hypertrophic cardiomyopathy: assessment with MR imaging and multidetector CT. Radiographics. 2010; 30:1309–1328.
Article43. Hashimura H, Kimura F, Ishibashi-Ueda H, Morita Y, Higashi M, Nakano S, et al. Radiologic-pathologic correlation of primary and secondary cardiomyopathies: MR imaging and histopathologic findings in hearts from autopsy and transplantation. Radiographics. 2017; 37:719–736.
Article44. Blankstein R, Waller AH. Evaluation of known or suspected cardiac sarcoidosis. Circ Cardiovasc Imaging. 2016; 9:e000867.
Article45. Isobe M, Tezuka D. Isolated cardiac sarcoidosis: clinical characteristics, diagnosis and treatment. Int J Cardiol. 2015; 182:132–140.
Article46. Kusano KF, Satomi K. Diagnosis and treatment of cardiac sarcoidosis. Heart. 2016; 102:184–190.
Article47. Lee HJ, Im DJ, Youn JC, Chang S, Suh YJ, Hong YJ, et al. Assessment of myocardial delayed enhancement with cardiac computed tomography in cardiomyopathies: a prospective comparison with delayed enhancement cardiac magnetic resonance imaging. Int J Cardiovasc Imaging. 2017; 33:577–584.
Article48. Chiles C, Woodard PK, Gutierrez FR, Link KM. Metastatic involvement of the heart and pericardium: CT and MR imaging. Radiographics. 2001; 21:439–449.
Article49. Galderisi M, Cardim N, D'Andrea A, Bruder O, Cosyns B, Davin L, et al. The multi-modality cardiac imaging approach to the athlete's heart: an expert consensus of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015; 16:353.
Article50. Spirito P, Pelliccia A, Proschan MA, Granata M, Spataro A, Bellone P, et al. Morphology of the “athlete's heart” assessed by echocardiography in 947 elites athletes representing 27 sports. Am J Cardiol. 1994; 74:802–806.51. Gräni C, Buechel RR, Kaufmann PA, Kwong RY. Multimodality imaging in individuals with anomalous coronary arteries. JACC Cardiovasc Imaging. 2017; 10:471–481.52. Marwick TH, Gillebert TC, Aurigemma G, Chirinos J, Derumeaux G, Galderisi M, et al. Recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). Eur Heart J Cardiovasc Imaging. 2015; 16:577–605.
Article53. Maceira AM, Mohiaddin RH. Cardiovascular magnetic resonance in systemic hypertension. J Cardiovasc Magn Reson. 2012; 14:28.
Article54. Rodrigues JC, Amadu AM, Dastidar AG, Hassan N, Lyen SM, Lawton CB, et al. Prevalence and predictors of asymmetric hypertensive heart disease: insights from cardiac and aortic function with cardiovascular magnetic resonance. Eur Heart J Cardiovasc Imaging. 2016; 17:1405–1413.
Article55. Maganti K, Rigolin VH, Sarano ME, Bonow RO. Valvular heart disease: diagnosis and management. Mayo Clin Proc. 2010; 85:483–500.
Article56. Badiani S, van Zalen J, Treibel TA, Bhattacharyya S, Moon JC, Lloyd G. Aortic stenosis, a left ventricular disease: insights from advanced imaging. Curr Cardiol Rep. 2016; 18:80.
Article57. Tuseth N, Cramariuc D, Rieck AE, Wachtell K, Gerdts E. Asymmetric septal hypertrophy - a marker of hypertension in aortic stenosis (a SEAS substudy). Blood Press. 2010; 19:140–144.
Article58. Czeyda-Pommersheim F, Hwang M, Chen SS, Strollo D, Fuhrman C, Bhalla S. Amyloidosis: modern cross-sectional imaging. Radiographics. 2015; 35:1381–1392.
Article59. Bhogal S, Ladia V, Sitwala P, Cook E, Bajaj K, Ramu V, et al. Cardiac amyloidosis: an updated review with emphasis on diagnosis and future directions. Curr Probl Cardiol. 2018; 43:10–34.
Article60. Deux JF, Mihalache CI, Legou F, Damy T, Mayer J, Rappeneau S, et al. Noninvasive detection of cardiac amyloidosis using delayed enhanced MDCT: a pilot study. Eur Radiol. 2015; 25:2291–2297.
Article61. Shah DJ, Kim HW, James O, Parker M, Wu E, Bonow RO, et al. Prevalence of regional myocardial thinning and relationship with myocardial scarring in patients with coronary artery disease. JAMA. 2013; 309:909–918.
Article62. Komatsu Y, Cochet H, Jadidi A, Sacher F, Shah A, Derval N, et al. Regional myocardial wall thinning at multidetector computed tomography correlates to arrhythmogenic substrate in postinfarction ventricular tachycardia: assessment of structural and electrical substrate. Circ Arrhythm Electrophysiol. 2013; 6:342–350.63. Cisneros S, Duarte R, Fernandez-Perez GC, Castellon D, Calatayud J, Lecumberri I, et al. Left ventricular apical diseases. Insights Imaging. 2011; 2:471–482.
Article64. Dec GW, Fuster V. Idiopathic dilated cardiomyopathy. N Engl J Med. 1994; 331:1564–1575.
Article65. McCrohon JA, Moon JC, Prasad SK, McKenna WJ, Lorenz CH, Coats AJ, et al. Differentiation of heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-enhanced cardiovascular magnetic resonance. Circulation. 2003; 108:54–59.
Article66. Nanjo S, Yoshikawa K, Harada M, Inoue Y, Namiki A, Nakano H, et al. Correlation between left ventricular diastolic function and ejection fraction in dilated cardiomyopathy using magnetic resonance imaging with late gadolinium enhancement. Circ J. 2009; 73:1939–1944.
Article67. Weiford BC, Subbarao VD, Mulhern KM. Noncompaction of the ventricular myocardium. Circulation. 2004; 109:2965–2971.
Article68. Ritter M, Oechslin E, Sütsch G, Attenhofer C, Schneider J, Jenni R. Isolated noncompaction of the myocardium in adults. Mayo Clin Proc. 1997; 72:26–31.
Article69. Freedom RM, Yoo SJ, Perrin D, Taylor G, Petersen S, Anderson RH. The morphological spectrum of ventricular noncompaction. Cardiol Young. 2005; 15:345–364.
Article70. Sidhu MS, Uthamalingam S, Ahmed W, Engel LC, Vorasettakarnkij Y, Lee AM, et al. Defining left ventricular noncompaction using cardiac computed tomography. J Thorac Imaging. 2014; 29:60–66.
Article71. Melendez-Ramirez G, Castillo-Castellon F, Espinola-Zavaleta N, Meave A, Kimura-Hayama ET. Left ventricular noncompaction: a proposal of new diagnostic criteria by multidetector computed tomography. J Cardiovasc Comput Tomogr. 2012; 6:346–354.
Article72. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al. Executive summary: heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012; 125:188–197.73. Rajiah P, Desai MY, Kwon D, Flamm SD. MR imaging of myocardial infarction. Radiographics. 2013; 33:1383–1412.
Article74. Ichikawa Y, Kitagawa K, Chino S, Ishida M, Matsuoka K, Tanigawa T, et al. Adipose tissue detected by multislice computed tomography in patients after myocardial infarction. JACC Cardiovasc Imaging. 2009; 2:548–555.
Article75. La Grutta L, Toia P, Maffei E, Cademartiri F, Lagalla R, Midiri M. Infarct characterization using CT. Cardiovasc Diagn Ther. 2017; 7:171–188.
Article76. Vliegenthart R, Henzler T, Moscariello A, Ruzsics B, Bastarrika G, Oudkerk M, et al. CT of coronary heart disease: part 1, CT of myocardial infarction, ischemia, and viability. AJR Am J Roentgenol. 2012; 198:531–547.
Article77. Cwajg JM, Cwajg E, Nagueh SF, He ZX, Qureshi U, Olmos LI, et al. End-diastolic wall thickness as a predictor of recovery of function in myocardial hibernation: relation to rest-redistribution T1-201 tomography and dobutamine stress echocardiography. J Am Coll Cardiol. 2000; 35:1152–1161.78. Nieman K, Cury RC, Ferencik M, Nomura CH, Abbara S, Hoffmann U, et al. Differentiation of recent and chronic myocardial infarction by cardiac computed tomography. Am J Cardiol. 2006; 98:303–308.
Article79. Cury RC, Nieman K, Shapiro MD, Butler J, Nomura CH, Ferencik M, et al. Comprehensive assessment of myocardial perfusion defects, regional wall motion, and left ventricular function by using 64-section multidetector CT. Radiology. 2008; 248:466–475.
Article80. Rodriguez-Granillo GA. Delayed enhancement cardiac computed tomography for the assessment of myocardial infarction: from bench to bedside. Cardiovasc Diagn Ther. 2017; 7:159–170.
Article81. Sato A, Nozato T, Hikita H, Akiyama D, Nishina H, Hoshi T, et al. Prognostic value of myocardial contrast delayed enhancement with 64-slice multidetector computed tomography after acute myocardial infarction. J Am Coll Cardiol. 2012; 59:730–738.
Article82. Sharma A, Kumar S. Overview of left ventricular outpouchings on cardiac magnetic resonance imaging. Cardiovasc Diagn Ther. 2015; 5:464–470.83. Makkuni P, Kotler MN, Figueredo VM. Diverticular and aneurysmal structures of the left ventricle in adults: report of a case within the context of a literature review. Tex Heart Inst J. 2010; 37:699–705.84. Frances C, Romero A, Grady D. Left ventricular pseudoaneurysm. J Am Coll Cardiol. 1998; 32:557–561.
Article85. Sharma RK, Gore R, Rosen BD, Arbab-Zadeh A. Diagnosis of left ventricular pseudoaneurysm by cardiac CT angiography. J Cardiovasc Comput Tomogr. 2014; 8:246–247.
Article86. Bradfield JW, Beck G, Vecht RJ. Left ventricular apical thin point. Br Heart J. 1977; 39:806–809.
Article87. Johnson KM, Johnson HE, Dowe DA. Left ventricular apical thinning as normal anatomy. J Comput Assist Tomogr. 2009; 33:334–337.
Article88. Deva DP, Williams LK, Care M, Siminovitch KA, Moshonov H, Wintersperger BJ, et al. Deep basal inferoseptal crypts occur more commonly in patients with hypertrophic cardiomyopathy due to disease-causing myofilament mutations. Radiology. 2013; 269:68–76.
Article89. Child N, Muhr T, Sammut E, Dabir D, Ucar EA, Bueser T, et al. Prevalence of myocardial crypts in a large retrospective cohort study by cardiovascular magneticresonance. J Cardiovasc Magn Reson. 2014; 16:66.
Article90. Germans T, Wilde AA, Dijkmans PA, Chai W, Kamp O, Pinto YM, et al. Structural abnormalities of the inferoseptal left ventricular wall detected by cardiac magnetic resonance imaging in carriers of hypertrophic cardiomyopathy mutations. J Am Coll Cardiol. 2006; 48:2518–2523.
Article91. Maron MS, Rowin EJ, Lin D, Appelbaum E, Chan RH, Gibson CM, et al. Prevalence and clinical profile of myocardial crypts in hypertrophic cardiomyopathy. Circ Cardiovasc Imaging. 2012; 5:441–447.
Article92. Ohlow MA. Congenital left ventricular aneurysms and diverticula: definition, pathophysiology, clinical relevance and treatment. Cardiology. 2006; 106:63–72.
Article93. Romagnoli A, Ricci A, Morosetti D, Fusco A, Citraro D, Simonetti G. Congenital left ventricular diverticulum: multimodality imaging evaluation and literature review. J Saudi Heart Assoc. 2015; 27:61–67.
Article94. Brunetti L, DeSantis ER. Treatment of viral myocarditis caused by coxsackievirus B. Am J Health Syst Pharm. 2008; 65:132–137.
Article95. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000; 343:1388–1398.
Article96. Okura Y, Dec GW, Hare JM, Kodama M, Berry GJ, Tazelaar HD, et al. A clinical and histopathologic comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis. J Am Coll Cardiol. 2003; 41:322–329.
Article97. Drory Y, Turetz Y, Hiss Y, Lev B, Fisman EZ, Pines A, et al. Sudden unexpected death in persons less than 40 years of age. Am J Cardiol. 1991; 68:1388–1392.98. Axsom K, Lin F, Weinsaft JW, Min JK. Evaluation of myocarditis with delayed-enhancement computed tomography. J Cardiovasc Comput Tomogr. 2009; 3:409–411.
Article99. Tröbs M, Brand M, Achenbach S, Marwan M. Ultra-low dose comprehensive cardiac CT imaging in a patient with acute myocarditis. J Cardiovasc Comput Tomogr. 2014; 8:475–476.
Article100. Kimura F, Matsuo Y, Nakajima T, Nishikawa T, Kawamura S, Sannohe S, et al. Myocardial fat at cardiac imaging: how can we differentiate pathologic from physiologic fatty infiltration? Radiographics. 2010; 30:1587–1602.
Article101. Kim SS, Ko SM, Song MG. Linear fat deposition in the middle layer of the left ventricular myocardium: computed tomographic findings. Korean J Radiol. 2010; 11:571–573.
Article102. Kim SS, Ko SM, Song MG. Fat streak in the middle layer of the left ventricular myocardium in a patient with dilated cardiomyopathy: findings of multidetector CT and MR imaging. Int J Cardiovasc Imaging. 2011; 27:745–748.
Article103. Zafar HM, Litt HI, Torigian DA. CT imaging features and frequency of left ventricular myocardial fat in patients with CT findings of chronic left ventricular myocardial infarction. Clin Radiol. 2008; 63:256–262.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Cardiac Computed Tomography in the Diagnosis of Left Ventricular Myocardial Diseases
- Cardiac Strain Analysis Using Cine Magnetic Resonance Imaging and Computed Tomography
- Pulling Bowstring of Gated Myocardial SPECT
- Pattern Analysis of Left Ventricular Remodeling Using Cardiac Computed Tomography in Children with Congenital Heart Disease: Preliminary Results
- Recent Trends in Nuclear Cardiology Practice
