Prediction of Treatment Response in Patients with Chronic Obstructive Pulmonary Disease by Determination of Airway Dimensions with Baseline Computed Tomography
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. sangmin.lee.md@gmail.com
- 2Department of Pulmonary and Critical Care Medicine, and Clinical Research Center for Chronic Obstructive Airway Diseases, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 2438261
- DOI: http://doi.org/10.3348/kjr.2018.0204
Abstract
OBJECTIVE
To determine the predictive factors for treatment responsiveness in patients with chronic obstructive pulmonary disease (COPD) at 1-year follow-up by performing quantitative analyses of baseline CT scans.
MATERIALS AND METHODS
COPD patients (n = 226; 212 men, 14 women) were recruited from the Korean Obstructive Lung Disease cohort. Patients received a combination of inhaled long-acting beta-agonists and corticosteroids twice daily for 3 months and subsequently received medications according to the practicing clinician's decision. The emphysema index, air-trapping indices, and airway parameter (Pi10), calculated using both full-width-half-maximum and integral-based half-band (IBHB) methods, were obtained with baseline CT scans. Clinically meaningful treatment response was defined as an absolute increase of ≥ 0.225 L in the forced expiratory volume in 1 second (FEV1) at the one-year follow-up. Multivariate logistic regression analysis was performed to investigate the predictors of an increase in FEV1, and receiver operating characteristic (ROC) analysis was performed to evaluate the performance of the suggested models.
RESULTS
Treatment response was noted in 47 patients (20.8%). The mean FEV1 increase in responders was 0.36 ± 0.10 L. On univariate analysis, the air-trapping index (ATI) obtained by the subtraction method, ATI of the emphysematous area, and IBHB-measured Pi10 parameter differed significantly between treatment responders and non-responders (p = 0.048, 0.042, and 0.002, respectively). Multivariate analysis revealed that the IBHB-measured Pi10 was the only independent variable predictive of an FEV1 increase (p = 0.003). The adjusted odds ratio was 1.787 (95% confidence interval: 1.220-2.619). The area under the ROC curve was 0.641.
CONCLUSION
Measurement of standardized airway dimensions on baseline CT by using a recently validated quantification method can predict treatment responsiveness in COPD patients.
Keyword
MeSH Terms
Figure
-

Fig. 1 Flowchart of study population.COPD = chronic obstructive pulmonary disease, KOLD = Korean Obstructive Lung Disease, PFT = pulmonary function test

Fig. 2 Measurement of standardized small-airway dimensions.Commercial software (Aview, Coreline Soft) automatically segments airways and detects airway level, lumens, and inner and outer boundaries of airway walls. After selecting most properly measured airways, software shows Pi10 with two different measurement algorithms (full-width-half-maximum and IBHB algorithms). IBHB = integral-based half-band, Pi10 = square root of airway wall area of theoretical airway with internal perimeter of 10 mm

Fig. 3 Calculation of Pi10.Square root of wall area of each measured airway (WA) was plotted against Pi of that airway. From regression line, standardized measure of airway wall thickness was predicted with Pi of 10 mm. Pi = internal perimeter
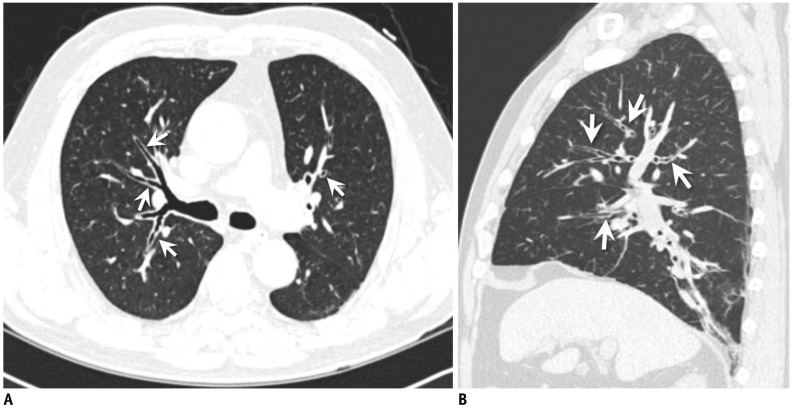
Fig. 4 Representative case of response to treatment in 58-year-old male patient.(A) Axial and (B) sagittal reconstructed images on baseline CT show diffuse bronchial wall thickening in both lungs (arrows). Pi10 by IBHB method was 4.82 mm and baseline FEV1 was 2.82 L. After receiving treatment, FEV1 at 1-year follow-up was 3.44 L, indicating increase of 0.62 L.FEV1 = forced expiratory volume in 1 second

Fig. 5 ROC curve of advanced baseline quantitation of standardized airway dimensions versus treatment response.Graph shows results of ROC analysis for differentiating between patients with and without treatment response by determining Pi10 obtained by IBHB. Area under curve for Pi10-IBHB was 0.641 (95% confidence interval: 0.558–0.724). Optimal cutoff value of Pi10-IBHB was 4.05 mm. Pi10-IBHB = Pi10 obtained by IBHB, ROC = receiver operating characteristic
Reference
-
1. Global Strategy for Diagnosis, Management, and Prevention of COPD-2016. Global Initiative for Chronic Obstructive Lung Disease. Accessed October 26, 2017. Available at: http://goldcopd.org/.2. McDonough JE, Yuan R, Suzuki M, Seyednejad N, Elliott WM, Sanchez PG, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease. N Engl J Med. 2011; 365:1567–1575. PMID: 22029978.
Article3. Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD, Lomas DA, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010; 11:122. PMID: 20831787.
Article4. Daudey L, Peters JB, Molema J, Dekhuijzen PN, Prins JB, Heijdra YF, et al. Health status in COPD cannot be measured by the St George's Respiratory Questionnaire alone: an evaluation of the underlying concepts of this questionnaire. Respir Res. 2010; 11:98. PMID: 20649991.
Article5. Bergin C, Müller N, Nichols DM, Lillington G, Hogg JC, Mullen B, et al. The diagnosis of emphysema. A computed tomographic-pathologic correlation. Am Rev Respir Dis. 1986; 133:541–546. PMID: 3963623.6. Nakano Y, Sakai H, Muro S, Hirai T, Oku Y, Nishimura K, et al. Comparison of low attenuation areas on computed tomographic scans between inner and outer segments of the lung in patients with chronic obstructive pulmonary disease: incidence and contribution to lung function. Thorax. 1999; 54:384–389. PMID: 10212100.
Article7. Lee YK, Oh YM, Lee JH, Kim EK, Lee JH, Kim N, et al. Quantitative assessment of emphysema, air trapping, and airway thickening on computed tomography. Lung. 2008; 186:157–165. PMID: 18351420.
Article8. Han MK, Kazerooni EA, Lynch DA, Liu LX, Murray S, Curtis JL, et al. COPDGene Investigators. Chronic obstructive pulmonary disease exacerbations in the COPDGene study: associated radiologic phenotypes. Radiology. 2011; 261:274–228. PMID: 21788524.
Article9. Grydeland TB, Dirksen A, Coxson HO, Pillai SG, Sharma S, Eide GE, et al. Quantitative computed tomography: emphysema and airway wall thickness by sex, age and smoking. Eur Respir J. 2009; 34:858–865. PMID: 19324952.
Article10. Kim SS, Jin GY, Li YZ, Lee JE, Shin HS. CT quantification of lungs and airways in normal Korean subjects. Korean J Radiol. 2017; 18:739–748. PMID: 28670169.
Article11. Park TS, Lee JS, Seo JB, Hong Y, Yoo JW, Kang BJ, et al. KOLD Study Group. Study design and outcomes of Korean Obstructive Lung Disease (KOLD) cohort study. Tuberc Respir Dis (Seoul). 2014; 76:169–174. PMID: 24851130.
Article12. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005; 26:319–338. PMID: 16055882.13. Tweeddale PM, Merchant S, Leslie M, Alexander F, McHardy GJ. Short term variability in FEV1: relation to pretest activity, level of FEV1, and smoking habits. Thorax. 1984; 39:928–932. PMID: 6515598.
Article14. Herpel LB, Kanner RE, Lee SM, Fessler HE, Sciurba FC, Connett JE, et al. National Emphysema Treatment Trial Research Group. Variability of spirometry in chronic obstructive pulmonary disease: results from two clinical trials. Am J Respir Crit Care Med. 2006; 173:1106–1113. PMID: 16497996.15. Cho YH, Seo JB, Kim N, Lee HJ, Hwang HJ, Kim EY, et al. Comparison of a new integral-based half-band method for CT measurement of peripheral airways in COPD with a conventional full-width half-maximum method using both phantom and clinical CT images. J Comput Assist Tomogr. 2015; 39:428–436. PMID: 25700223.
Article16. Galbán CJ, Han MK, Boes JL, Chughtai KA, Meyer CR, Johnson TD, et al. Computed tomography-based biomarker provides unique signature for diagnosis of COPD phenotypes and disease progression. Nat Med. 2012; 18:1711–1715. PMID: 23042237.
Article17. Kim EY, Seo JB, Lee HJ, Kim N, Lee E, Lee SM, et al. Detailed analysis of the density change on chest CT of COPD using non-rigid registration of inspiration/expiration CT scans. Eur Radiol. 2015; 25:541–549. PMID: 25218764.
Article18. Lee SM, Seo JB, Lee SM, Kim N, Oh SY, Oh YM. Optimal threshold of subtraction method for quantification of air-trapping on coregistered CT in COPD patients. Eur Radiol. 2016; 26:2184–2192. PMID: 26515547.
Article19. Kitaguchi Y, Fujimoto K, Kubo K, Honda T. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006; 100:1742–1752. PMID: 16549342.
Article20. Nakano Y, Muro S, Sakai H, Hirai T, Chin K, Tsukino M, et al. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function. Am J Respir Crit Care Med. 2000; 162(3 Pt 1):1102–1108. PMID: 10988137.21. Nakano Y, Müller NL, King GG, Niimi A, Kalloger SE, Mishima M, et al. Quantitative assessment of airway remodeling using high-resolution CT. Chest. 2002; 122(6 Suppl):271S–275S.
Article22. Kim N, Seo JB, Song KS, Chae EJ, Kang SH. Semi-automatic measurement of the airway dimension by computed tomography using the full-with-half-maximum method: a study of the measurement accuracy according to the orientation of an artificial airway. Korean J Radiol. 2008; 9:236–242. PMID: 18525226.
Article23. Fujimoto K, Kitaguchi Y, Kubo K, Honda T. Clinical analysis of chronic obstructive pulmonary disease phenotypes classified using high-resolution computed tomography. Respirology. 2006; 11:731–740. PMID: 17052301.
Article24. Pistolesi M, Camiciottoli G, Paoletti M, Marmai C, Lavorini F, Meoni E, et al. Identification of a predominant COPD phenotype in clinical practice. Respir Med. 2008; 102:367–376. PMID: 18248806.
Article25. Pennock BE, Rogers RM, McCaffree DR. Changes in measured spirometric indices. What is significant? Chest. 1981; 80:97–99. PMID: 7249720.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical use of chest CT in chronic obstructive pulmonary diseases
- Recent advances in airway imaging using micro-computed tomography and computed tomography for chronic obstructive pulmonary disease
- Phenotype of Chronic Obstructive Pulmonary Disease Based on Computed Tomography–Defined Underlying Pathology
- Pathogenesis and pathophysiology of COPD
- Chronic Obstructive Pulmonary Disease: Respiratory Review of 2013
