“Spray-as-you-go†medical technique for awake intubation using a combination of an epidural catheter and the OptiScope in a patient with Ludwig's angina: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea. anaper@naver.com
- 2Department of Anesthesiology and Pain Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2436045
- DOI: http://doi.org/10.17085/apm.2018.13.3.336
Abstract
- A 73-year-old woman presented to the emergency department with submandibular pain and swelling. The patient was diagnosed to have Ludwig's angina, and she was planned to undergo urgent incision and drainage under general anesthesia. However, her physical examination revealed severe diffuse swelling extending from the bilateral submandibular spaces to the submental space and further down to the neck. As our view was blocked by the patient's neck swelling, we did not perform a regional anesthesia of the airway or a transtracheal block. Several non-invasive alternatives were considered. The "spray-as-you-go" technique was chosen, and it was performed using the OptiScope®. However, the OptiScope did not have a working channel or syringe adaptor for the administration of the local anesthetic solution. To solve this problem, we combined the OptiScope with a 27-G tunneled epidural catheter (100 cm) for the administration of lidocaine and this combination made the awake intubation successful.
Keyword
MeSH Terms
Figure
-
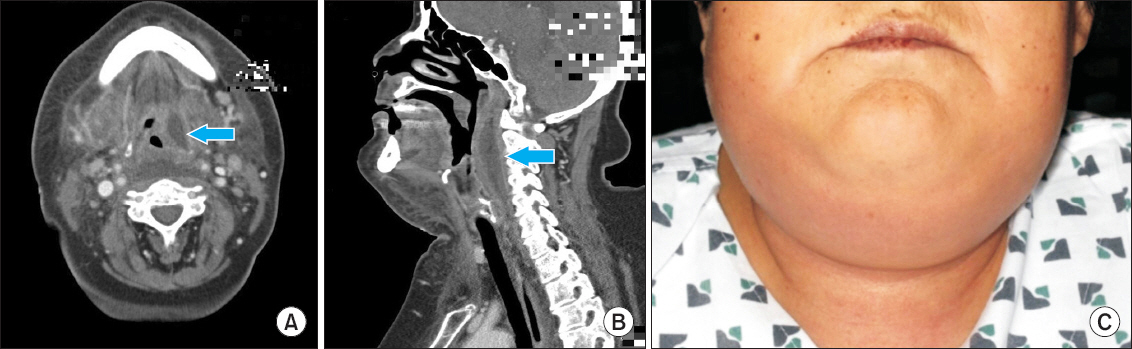
Fig. 1 Contrast-enhanced computed tomography scan of the neck showed a well-defined longitudinally oval, heterogeneously enhancing soft tissue lesion (6 × 4 × 3 cm) in the left carotid space (A) and retropharyngeal space (B) extending longitudinally between C1 and C4. The patient was diagnosed to have Ludwig’s angina (C).

Fig. 2 The OptiScope® (Clarus Medical, USA) was prepared for the “spray-as-you-go” awake intubation. A cutting epidural catheter (100 cm) (Portex®, Smiths Medical Ltd., Australia) was inserted into the endotracheal tube (A). The picture was taken to demonstrate the structures of the catheter and endotracheal tube. A tip of the epidural catheter was cut and the end of the catheter was not left poking out of the endotracheal tube (B).

Fig. 3 2% Lidocaine was administered below the glottis through the tip of the epidural catheter to anesthetize the mucosa of the epiglottis and vocal cords to prevent the gag reflex, cough, pain, nausea, and vomiting into her mouth and throat.
Reference
-
1. Iqbal R, Kapila A. Difficult airway: definitions, incidence and consequences. Difficult airway management. Popat MT, editor. Oxford: Oxford University Press;2009. p. 1–10. DOI: 10.1093/med/9780199554515.003.0001.2. Gil KSL, Diemunsch PA. Flexible scope intubation techniques. Hagberg and Benumof's airway management. 4th ed. Hagberg CA, Artime CA, Aziz MF, editors. Philadelphia: Elsevier;2018. p. 428–70.3. Maktabi MA, Hoffman H, Funk G, From RP. Laryngeal trauma during awake fiberoptic intubation. Anesth Analg. 2002; 95:1112–4. DOI: 10.1097/00000539-200210000-00061. PMID: 12351306.4. Finucane BT, Tsui BCH, Santora AH. Principles of airway management. 4th ed. New York: Springer;2011. p. 548–50. DOI: 10.1007/978-0-387-09558-5.5. Sethi N, Tarneja VK, Madhusudanan TP, Shouche S. Local anaesthesia for fiberoptic intubation: a comparison of three techniques. Med J Armed Forces India. 2005; 61:22–5. DOI: 10.1016/S0377-1237(05)80112-1.6. Mushambi MC, Pandey R. Management of the difficult airway in the obstetric patient. Oxford textbook of obstetric anaesthesia. Clark V, de Velde MV, Fernando R, editors. Oxford: Oxford University Press;2016; 393–418.7. Candamourty R, Venkatachalam S, Babu MR, Kumar GS. Ludwig's angina - an emergency: a case report with literature review. J Nat Sci Biol Med. 2012; 3:206–8. DOI: 10.4103/0976-9668.101932. PMID: 23225990. PMCID: PMC3510922.8. Saifeldeen K, Evans R. Ludwig's angina. Emerg Med J. 2004; 21:242–3. DOI: 10.1136/emj.2003.012336. PMID: 14988363. PMCID: PMC1726306.9. Kulkarni AH, Pai SD, Bhattarai B, Rao ST, Ambareesha M. Ludwig's angina and airway considerations: a case report. Cases J. 2008; 1:19. DOI: 10.1186/1757-1626-1-19. PMID: 18577200. PMCID: PMC2440366.10. Pedigo RA, Amsterdam JT. Oral medicine. Rosen's emergency medicine: concepts and clinical practice. 9th ed. Walls RM, Hockberger RS, Gausche-Hill M, editors. Philadelphia: Elsevier;2017. p. 771–89.11. Hagberg C, Artime C. Airway Management in the Adult. Miller's anesthesia. 8th ed. Miller RD, Cohen NH, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL, editors. Philadelphia: Elsevier/Saunders, cop;2015. p. 1647–83.12. Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult airway society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015; 115:827–48. DOI: 10.1093/bja/aev371. PMID: 26556848. PMCID: PMC4650961.13. Abramowicz AE, Bustillo M. Anesthesia for cervical spinal cord injury. Anesthesia for trauma: new evidence and new challenges. Scher CS, editor. New York: Springer;2014; 167–92. DOI: 10.1007/978-1-4939-0909-4_9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Air-Q(R)sp-assisted awake fiberoptic bronchoscopic intubation in a patient with Ludwig's angina
- Retrograde Intubation Technique Used Epidural Catheter; 3 Cases
- A Case of Ludwig Angina
- Difficult Airway Management with Fiberoptic Bronchoscopy Combined with Video Laryngoscope in a Patient with Ludwig Angina
- Retrograde Tracheal Intubation through Cricothyroid Membrane
