Novel Findings of Polypoidal Choroidal Vasculopathy via Optical Coherence Tomography Angiography
- Affiliations
-
- 1Department of Ophthalmology, Nune Eye Hospital, Seoul, Korea. owkwon0301@gmail.com
- KMID: 2434305
- DOI: http://doi.org/10.3341/kjo.2018.0048
Abstract
- PURPOSE
To introduce novel findings of polypoidal choroidal vasculopathy (PCV) via optical coherence tomography angiography (OCTA)
METHODS
This study is a retrospective chart review of 16 patients (16 eyes) with PCV. OCTA (Avanti RTVue XR) findings were evaluated and selected for analysis after agreement by two retina specialists .
RESULTS
Twenty one polyps in 16 eyes (16 patients) with PCV were included in this study. The mean patient age was 67 years (13 men and three women). The shape of polypoidal lesions on OCTA at initial were halo (five polyps), rosette (seven polyps), and vascular network (nine polyps). Eight months after anti-vascular endothelial growth factor treatment, in a total of four eyes, seven polyps could be followed up completely, the two halo type polypoidal lesions changed to rosette and vascular network type. The lesions of three rosette and two vascular network type lesions did not change in shape. In addition, the size of the polypoidal lesions (one among two halo types, two among three rosette types, and two among two vascular network types) decreased, but one halo type did not change and one rosette type increased in size on OCTA.
CONCLUSIONS
En-face OCTA enabled us to categorize novel types of PCV with polypoidal lesions.
Keyword
MeSH Terms
Figure
-
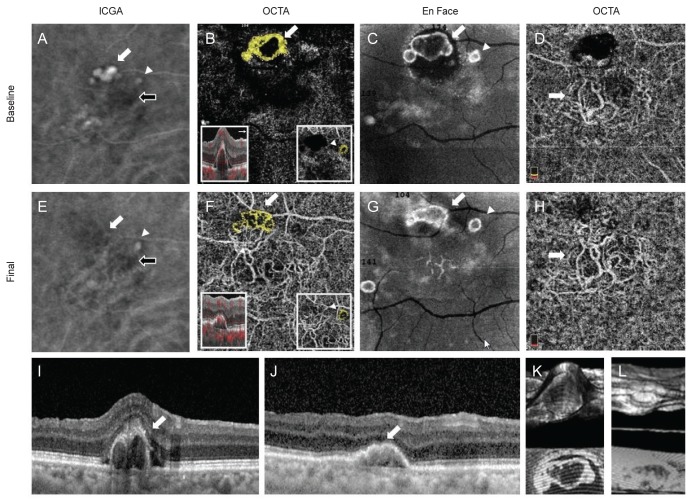
Fig. 1 Case 1 indocyanine green angiography (ICGA), optical coherence tomography angiography (OCTA), En Face, and spectral-domain optical coherence tomography (SD-OCT) findings. (A) Two hot spots (cluster and aneurysm, white arrow and arrowhead) of polypoidal lesions and branching vascular network (BVN, black arrow) were detected on ICGA. (B) Two round and high-flow outlined with dark halo polypoidal lesions (arrow and arrowhead, yellow colored area) were detected on OCTA. (C) These polpypoidal lesions were also detected on En-Face image (cluster and aneurysm, white arrow and arrowhead). (D) BVN (arrow) was identified on OCTA. (E) Cluster type of polypoidal lesion was disappeared after treatment, but aneurysm type was still remained on ICGA (cluster and aneurysm, white arrow and arrowhead; BVN, black arrow). (F) Large-sized halo type of polyp (arrow) was changed to vascular network type, and small-sized halo type polyp (arrowhead) was changed into rosette type on OCTA. (G) En-Face finding of polyps after treatment (cluster and aneurysm, white arrow and arrowhead). (H) Decreased the area of BVN (arrow) on OCTA. (I,J) SD-OCT finding of polyps (arrow) at initial and after treatment. (K,L) 3D finding of polyp at initial and after treatment.
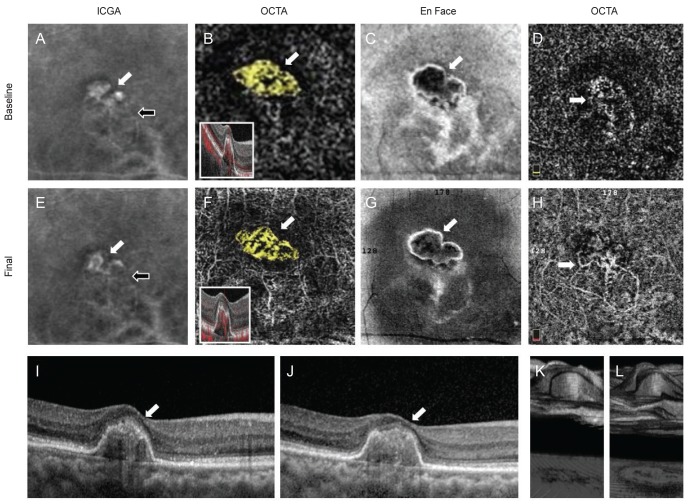
Fig. 2 Case 2 indocyanine green angiography (ICGA), optical coherence tomography angiography (OCTA), En Face, and spectral-domain optical coherence tomography (SD-OCT) findings. (A) Cluster type of polypoidal lesion (white arrow) and branching vascular network (BVN, black arrow) were detected on ICGA. (B) High-flow vascular network polypoidal lesions (white arrow and yellow colored area) was detected on OCTA. (C) This polpypoidal lesion (white arrow) was also detected on En-Face image. (D) BVN (arrow) was identified on OCTA. (E) Decreased size of cluster type polypoidal lesion (white arrow) and BVN (black arrow) after treatment on ICGA. (F) Vascular network type of polyp (white arrow) was maintained as the original type on OCTA. (G) En-Face finding of polyp (white arrow) after treatment. (H) Decreased the area of BVN (arrow) on OCTA. (I,J) SD-OCT finding of polyps (arrow) at initial and after treatment. (K,L) 3D finding of polyp at initial and after treatment.
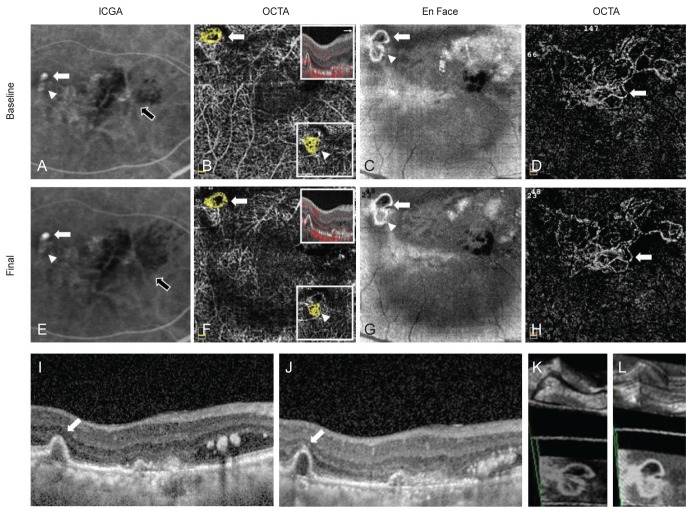
Fig. 3 Case 3 indocyanine green angiography (ICGA), optical coherence tomography angiography (OCTA), En Face, and spectral-domain optical coherence tomography (SD-OCT) findings. (A) Two hot spots (aneurysms, white arrow and arrowhead) of polypoidal lesions and branching vascular network (BVN, black arrow) were detected on ICGA. (B) High-flow outlined with irregular dark halo, the rosette type, polypoidal lesions (arrow) and high-flow vascular network type polypoidal lesion (arrowhead, in the small box) were detected on OCTA (yellow colored area). (C) These polpypoidal lesions (white arrow and arrow head) were also detected on En-Face image. (D) BVN (arrow) was identified on OCTA. (E) The brighter and large-sized aneurysm type of polypoidal lesion (white arrow) was increased the size, but the relatively faint aneurysm type (arrowhead) was almost disappeared after treatment on ICGA (BVN, black arrow). (F) The rosette type (arrow) and the vascular network type (arrowhead, in the small box) were unchanged as the original types after treatment on OCTA. (G) En-Face finding of polyps (white arrow and arrow head) after treatment. (H) Increased the area of BVN (arrow) on OCTA after treatment. (I,J) SD-OCT finding of polyps (arrow) at initial and after treatment. (K,L) 3D finding of polyps at initial and after treatment.
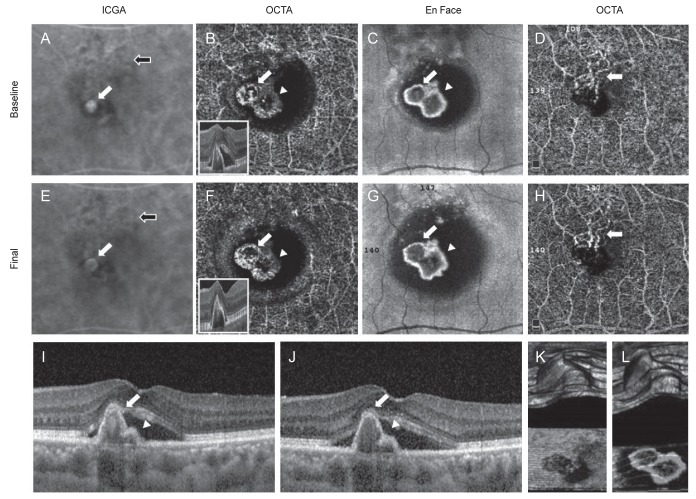
Fig. 4 Case 4 indocyanine green angiography (ICGA), optical coherence tomography angiography (OCTA), En Face, and spectral-domain optical coherence tomography (SD-OCT) findings. (A) One hot spots (aneurysm, white arrow) of polypoidal lesion and branching vascular network (BVN, black arrow) were detected on ICGA. (B) Two round and high-flow outlined with irregular dark halo polypoidal lesions (arrow and arrowhead) were detected on OCTA. (C) These polpypoidal lesions (white arrow and arrowhead) were also detected on En-Face image. (D) BVN (arrow) was identified on OCTA. (E) The fluorescence of aneurysm type of polypoidal lesion (white arrow) was decreased size after treatment (BVN, black arrow). (F) Two rosette type polyps (arrow and arrowhead) were remained as the original types after treatment on OCTA. (G) En-Face finding of polyps (white arrow and arrowhead) after treatment. (H) Decreased the area of BVN (arrow) on OCTA after treatment. (I,J) SD-OCT finding of polyps (white arrow and arrowhead) at initial and after treatment. (K,L) 3D finding of polyps at initial and after treatment.
Reference
-
1. Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina. 1990; 10:1–8. PMID: 1693009.
Article2. Spaide RF, Yannuzzi LA, Slakter JS, et al. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina. 1995; 15:100–110. PMID: 7542796.
Article3. Yannuzzi LA, Ciardella A, Spaide RF, et al. The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 1997; 115:478–485. PMID: 9109756.
Article4. Tateiwa H, Kuroiwa S, Gaun S, et al. Polypoidal choroidal vasculopathy with large vascular network. Graefes Arch Clin Exp Ophthalmol. 2002; 240:354–361. PMID: 12073058.
Article5. Uyama M, Matsubara T, Fukushima I, et al. Idiopathic polypoidal choroidal vasculopathy in Japanese patients. Arch Ophthalmol. 1999; 117:1035–1042. PMID: 10448746.
Article6. Uyama M, Wada M, Nagai Y, et al. Polypoidal choroidal vasculopathy: natural history. Am J Ophthalmol. 2002; 133:639–648. PMID: 11992861.7. Li X. Polypoidal choroidal vasculopathy. In : Ryan SJ, Sadda SR, Hinton DR, editors. Retina. 5th ed. St. Louis: Mosby;2013. p. 1285–1290.8. Koh AH. Expert PCV Panel. Chen LJ, et al. Polypoidal choroidal vasculopathy: evidence-based guidelines for clinical diagnosis and treatment. Retina. 2013; 33:686–716. PMID: 23455233.9. Ojima Y, Hangai M, Sakamoto A, et al. Improved visualization of polypoidal choroidal vasculopathy lesions using spectral-domain optical coherence tomography. Retina. 2009; 29:52–59. PMID: 18827738.
Article10. Miura M, Muramatsu D, Hong YJ, et al. Noninvasive vascular imaging of polypoidal choroidal vasculopathy by Doppler optical coherence tomography. Invest Ophthalmol Vis Sci. 2015; 56:3179–3186. PMID: 26024101.
Article11. Cheung CM, Yanagi Y, Mohla A, et al. Characterization and differentiation of polypoidal choroidal vasculopathy using swept source optical coherence tomography angiography. Retina. 2017; 37:1464–1474. PMID: 27828911.
Article12. Kim JY, Kwon OW, Oh HS, et al. Optical coherence tomography angiography in patients with polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2016; 254:1505–1510. PMID: 26617178.
Article13. Srour M, Querques G, Semoun O, et al. Optical coherence tomography angiography characteristics of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2016; 100:1489–1493. PMID: 26837506.
Article14. Tomiyasu T, Nozaki M, Yoshida M, Ogura Y. Characteristics of polypoidal choroidal vasculopathy evaluated by optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016; 57:OCT324–OCT330. PMID: 27409489.
Article15. Wang M, Zhou Y, Gao SS, et al. Evaluating polypoidal choroidal vasculopathy with optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016; 57:OCT526–OCT532. PMID: 27472276.
Article16. Takayama K, Ito Y, Kaneko H, et al. Comparison of indocyanine green angiography and optical coherence tomographic angiography in polypoidal choroidal vasculopathy. Eye (Lond). 2017; 31:45–52. PMID: 27813526.
Article17. Tanaka K, Mori R, Kawamura A, et al. Comparison of OCT angiography and indocyanine green angiographic findings with subtypes of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2017; 101:51–55. PMID: 27913447.
Article18. Lee JW, Kim IT. Epidemiologic and clinical characteristics of polypoidal choroidal vasculopathy in Korean patients. J Korean Ophthalmol Soc. 2007; 48:63–74.19. Wen F, Chen C, Wu D, Li H. Polypoidal choroidal vasculopathy in elderly Chinese patients. Graefes Arch Clin Exp Ophthalmol. 2004; 242:625–629. PMID: 15257461.
Article20. Schneider U, Gelisken F, Kreissig I. Indocyanine green angiography and idiopathic polypoidal choroidal vasculopathy. Br J Ophthalmol. 1998; 82:98–99. PMID: 9536893.
Article21. Inoue M, Balaratnasingam C, Freund KB. Optical coherence tomography angiography of polypoidal choroidal vasculopathy and polypoidal choroidal neovascularization. Retina. 2015; 35:2265–2274. PMID: 26405770.
Article22. Inoue M, Arakawa A, Yamane S, Kadonosono K. Short-term efficacy of intravitreal aflibercept in treatment-naive patients with polypoidal choroidal vasculopathy. Retina. 2014; 34:2178–2184. PMID: 25046397.
Article23. Ijiri S, Sugiyama K. Short-term efficacy of intravitreal aflibercept for patients with treatment-naïve polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2015; 253:351–357. PMID: 25023147.
Article24. Gomi F, Sawa M, Sakaguchi H, et al. Efficacy of intravitreal bevacizumab for polypoidal choroidal vasculopathy. Br J Ophthalmol. 2008; 92:70–73. PMID: 17567661.
Article25. Kokame GT, Yeung L, Lai JC. Continuous anti-VEGF treatment with ranibizumab for polypoidal choroidal vasculopathy: 6-month results. Br J Ophthalmol. 2010; 94:297–301. PMID: 19726427.
Article26. Spaide RF, Donsoff I, Lam DL, et al. Treatment of polypoidal choroidal vasculopathy with photodynamic therapy. Retina. 2002; 22:529–535. PMID: 12441716.
Article27. Silva RM, Figueira J, Cachulo ML, et al. Polypoidal choroidal vasculopathy and photodynamic therapy with verteporfin. Graefes Arch Clin Exp Ophthalmol. 2005; 243:973–979. PMID: 15864616.
Article28. Wong CW, Yanagi Y, Lee WK, et al. Age-related macular degeneration and polypoidal choroidal vasculopathy in Asians. Prog Retin Eye Res. 2016; 53:107–139. PMID: 27094371.
Article29. Koh A, Lee WK, Chen LJ, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina. 2012; 32:1453–1464. PMID: 22426346.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Availability of Optical Coherence Tomography in Diagnosis and Classification of Choroidal Neovascularization
- Diagnosing Polypoidal Choroidal Vasculopathy Using Color Fundus Photography, Optical Coherence Tomography, and Optical Coherence Tomography Angiography
- Comparison of Indocyanine Green Angiography and Optical Coherence Tomography Angiography for Polypoidal Choroidal Vasculopathy
- Epidemiologic and Clinical Characteristics of Polypoidal Choroidal Vasculopathy in Korean Patients
- Optical Coherence Tomography of Idiopathic Polypoidal Choroidal Vasculopathy
