Bilateral Gluteal Necrosis and Deep Infection after Transarterial Embolization for Pelvic Ring Injury in Patient with Hemodynamic Instability: A Case Report
- Affiliations
-
- 1Department of Trauma Surgery, Pusan National University Hospital, Busan, Korea.
- 2Department of Intervention Radiology, Pusan National University Hospital, Busan, Korea.
- 3Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea. realjang1979@gmail.com
- KMID: 2432500
- DOI: http://doi.org/10.12671/jkfs.2019.32.1.56
Abstract
- Transarterial embolization is accepted as effective and safe for the acute management in hemodynamically unstable patients with pelvic ring injury. However, transarterial embolization has potential complications, such as gluteal muscle/skin necrosis, deep infection, surgical wound breakdown, and internal organ infarction, which are caused by blocked blood flow to surrounding tissues and organs, and many studies on the complications have been reported. Here, we report an experience of the management of gluteal necrosis and infection that occurred after transarterial embolization, with a review of the relevant literature.
Figure
-

Fig. 1 (A) A 22-year-old female patient fell from the 5th floor and was transferred to the emergency room of the trauma center. During the primary survey according to ATLS® (Advanced Trauma Life Support), Focused Assessment with Sonography for Trauma was negative and anteroposterior pelvic radiograph showed an unstable pelvic ring injury. (B) The abdomen radiograph taken after preperitoneal pelvic packing and application of a pelvic binder showed decreased pelvic volume and reduction of iliac fracture.
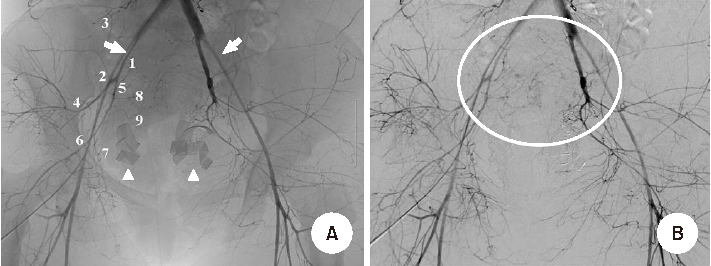
Fig. 2 (A) Transarterial pelvic aortography demonstrated diffuse attenuation of bilateral common, external (arrows), and internal iliac arteries. Radiographic gauzes for preperitoneal pelvic packing were also noted (arrowheads). Diffuse attenuation of internal iliac artery (1), the posterior division branch of the internal iliac artery (2) including iliolumbar artery (3), superior gluteal artery (4), and the anterior division branch of the internal iliac artery (5) including inferior gluteal artery (6), obturator artery (7), internal pudendal artery (8), medial sacral artery (9) were observed. (B) Digital subtraction angiography of pelvic aortography showed equivocal contrast blushes from both internal iliac arteries and their anterior divisional branches (circle). Nonselective embolization of bilateral internal iliac artery was performed.
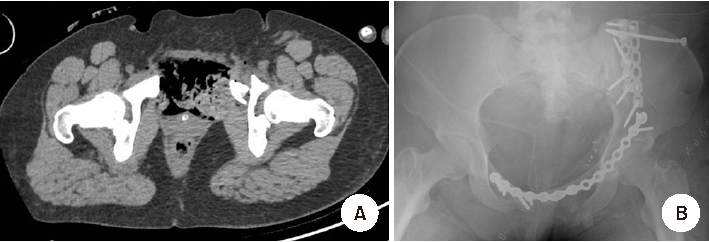
Fig. 3 (A) The pelvic ring injury was a closed fracture and Morel-Lavallee lesion was not observed in preoperative computed tomography scan. (B) Open reduction and internal fixation through the modified Stoppa approach with lateral window was performed on the fourth day after the injury.
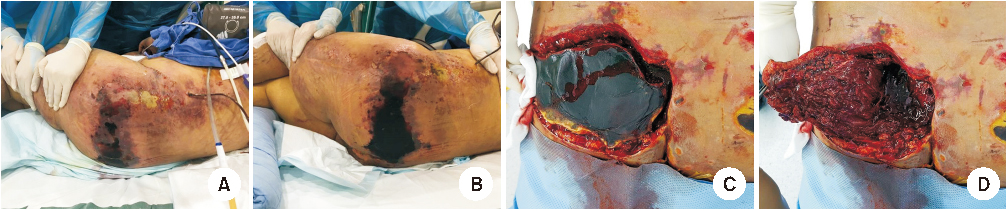
Fig. 4 (A) On the 5th day after the injury, skin color change of both buttocks was first detected in the intensive care unit. (B) Skin necrosis progressed. (C) On the 10th day after the injury, surgery for gluteal necrosis was performed. (D) The affected skin was excised and extensive necrosis and infection of gluteus maximus muscle were observed. Surgical debridement, copious irrigation and vacuum-assisted closure were performed.
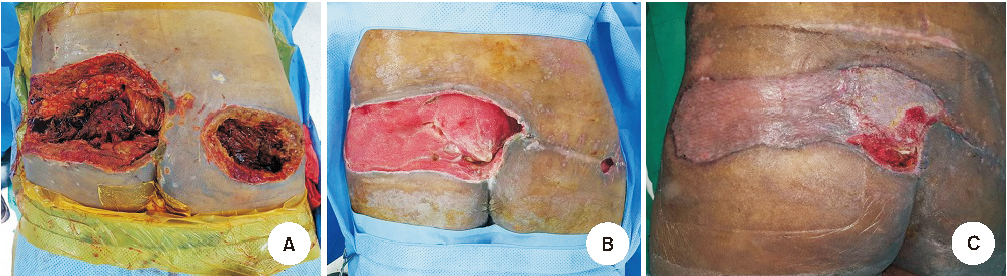
Fig. 5 (A) Repetitive surgical debridement was performed concurrently with intravenous antibiotics. (B) The infection was controlled about two months after the surgeries and sufficient formation of granulation tissues was achieved for skin graft. (C) A suture was performed for the right buttock and a skin graft for the left. There is no evidence of infection at the surgical wound, and some defects in the skin graft site are still under treatment.
Reference
-
1. El-Haj M, Bloom A, Mosheiff R, Liebergall M, Weil YA. Outcome of angiographic embolisation for unstable pelvic ring injuries: factors predicting success. Injury. 2013; 44:1750–1755.
Article2. Lustenberger T, Wutzler S, Störmann P, Laurer H, Marzi I. The role of angio-embolization in the acute treatment concept of severe pelvic ring injuries. Injury. 2015; 46:Suppl 4. S33–S38.
Article3. Perez JV, Hughes TM, Bowers K. Angiographic embolisation in pelvic fracture. Injury. 1998; 29:187–191.
Article4. Takahira N, Shindo M, Tanaka K, Nishimaki H, Ohwada T, Itoman M. Gluteal muscle necrosis following transcatheter angiographic embolisation for retroperitoneal haemorrhage associated with pelvic fracture. Injury. 2001; 32:27–32.
Article5. Matityahu A, Marmor M, Elson JK, et al. Acute complications of patients with pelvic fractures after pelvic angiographic embolization. Clin Orthop Relat Res. 2013; 471:2906–2911.
Article6. Tanizaki S, Maeda S, Matano H, Sera M, Nagai H, Ishida H. Time to pelvic embolization for hemodynamically unstable pelvic fractures may affect the survival for delays up to 60 min. Injury. 2014; 45:738–741.
Article7. Velmahos GC, Chahwan S, Falabella A, Hanks SE, Demetriades D. Angiographic embolization for intraperitoneal and retroperitoneal injuries. World J Surg. 2000; 24:539–545.
Article8. Li Q, Dong J, Yang Y, et al. Retroperitoneal packing or angioembolization for haemorrhage control of pelvic fractures--Quasi-randomized clinical trial of 56 haemodynamically unstable patients with Injury Severity Score ≥33. Injury. 2016; 47:395–401.
Article9. Yoon HK, Kim MD, Han SH, Kim BK, Ahn TK. Effectiveness of arterial embolization in hemodynamically unstable pelvic fracture. J Korean Hip Soc. 2008; 20:117–123.
Article10. Hak DJ, Smith WR, Suzuki T. Management of hemorrhage in life-threatening pelvic fracture. J Am Acad Orthop Surg. 2009; 17:447–457.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior Gluteal Artery Injury during Percutaneous Iliosacral Screw Fixation: A Case Report
- Early Results of Percutaneous Ilioscral Screw Fixation in Unstable Posterior Pelvic Ring Injury
- Latent Superior Gluteal Artery Injury by Entrapment between the Fragments in Transverse Acetabular Fracture - A Case Report -
- Testicular Dislocation Associated with Pelvic Ring Injury
- A Case of Uterine Fibroids Necrosis after Transarterial Embolization for Treatment of Uterine Fibroids
