Conservative surgical treatment for ameloblastoma: a report of three cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Kyung Hee University Dental Hospital at Gangdong, Korea. omsjyj@khu.ac.kr
- 2Department of Pathology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- KMID: 2430586
- DOI: http://doi.org/10.5125/jkaoms.2018.44.5.242
Abstract
- Ameloblastoma treatment varies based on the clinical, histopathologic, and radiographic characteristics. Aggressive surgical treatments, such as marginal or segmental resection, have traditionally been implemented, but some conservative surgical methods are also being introduced, including decompression, enucleation, or curettage. The aim of the present study was to evaluate the possibility of applying these conservative surgical treatments to ameloblastoma and to analyze the prognosis of the procedures and their healing aspects. Among all patients who visited our clinic (Department of Oral and Maxillofacial Surgery, Kyung Hee University Dental Hospital at Gangdong) from 2009 to 2017, three who had undergone conservative surgery were recruited. One of these three patients underwent both excision of the lesion and an iliac bone graft during the same procedure. In the other two patients, due to the size of the lesion, decompression was performed to reduce the size of the lesion, and then conservative surgical treatments followed. As shown in the cases of this study, patients were only treated with conservative surgical methods, such as decompression or enucleation. During the follow-up period, there were no recurrences. In conclusion, the use of conservative surgical treatment in ameloblastoma can be a reliable, safe, and successful method.
MeSH Terms
Figure
-
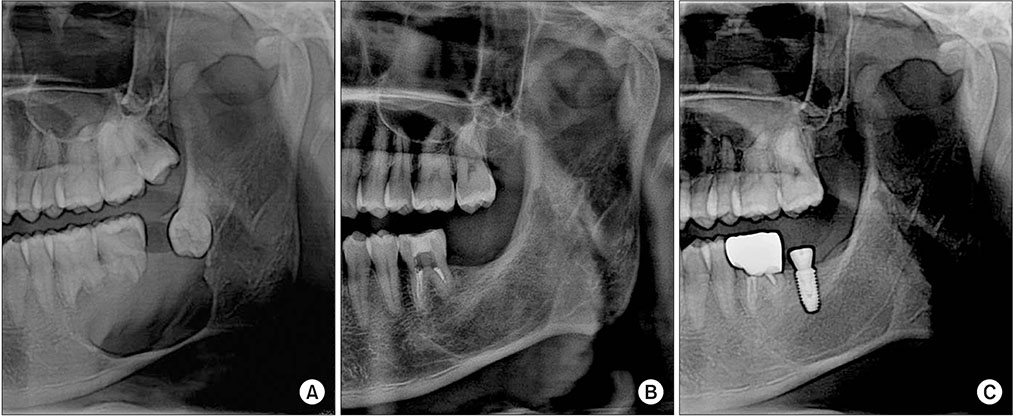
Fig. 1 A. X-ray shows a fairly large, well-defined rounded cystic destructive lesion involving the left mandibular body. Absorption of the roots of #36 and #37 is also apparent. B. Nine months after surgery, a panoramic view reveals favorable healing of the grafted iliac bone without any inflammation. C. One year five months after surgery, an implant fixture was placed near the #37 area. A 5.0 mm×10.0 mm implant was used, and the insertion path was satisfactory.
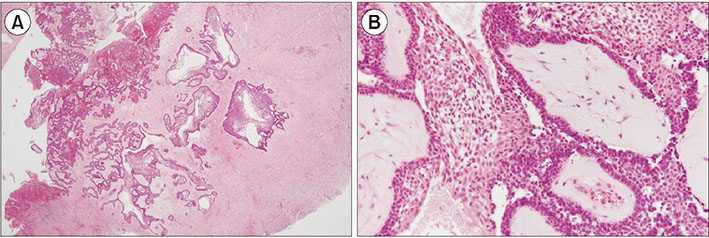
Fig. 2 Microscopic characteristics. A. Underlying the fibrous capsule, proliferation of neoplastic cells was noted; the cells were arranged in strands and in islands (H&E staining, ×20). B. Mural unicystic ameloblastoma shows invasive islands of the ameloblastic epithelium (H&E staining, ×100).
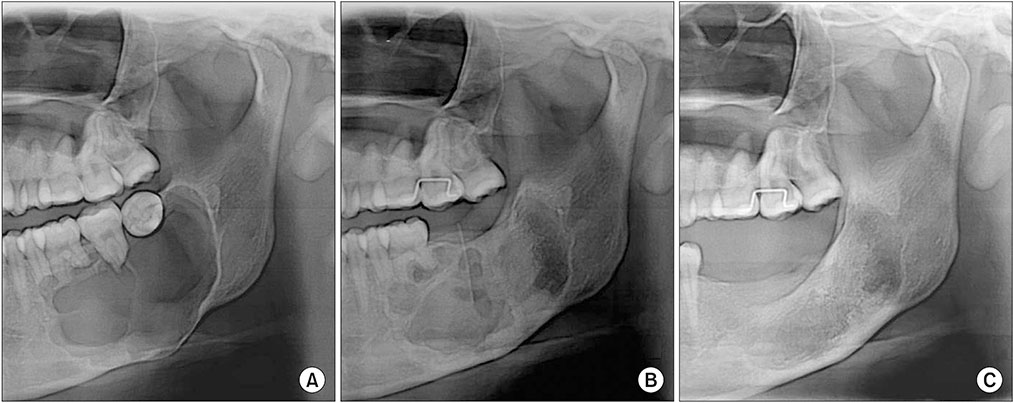
Fig. 3 A. The panoramic view shows a large, round-shaped radiolucent lesion near the posterior teeth. B. Nine months later after decompression, the size of the lesion had decreased. C. One year after surgery, bone formation at the operative site was satisfactory.

Fig. 4 Microscopic characteristics. A. The tumor is composed of a partly cystic portion and a solid portion (H&E staining, ×20). B. The tumor contains anastomosing cords and strands. At the center of these anastomoses, the cells are loosely arranged and have a cystic appearance. Each cell is spindle-shaped and has hyperchromatic nuclei (H&E staining, ×100).
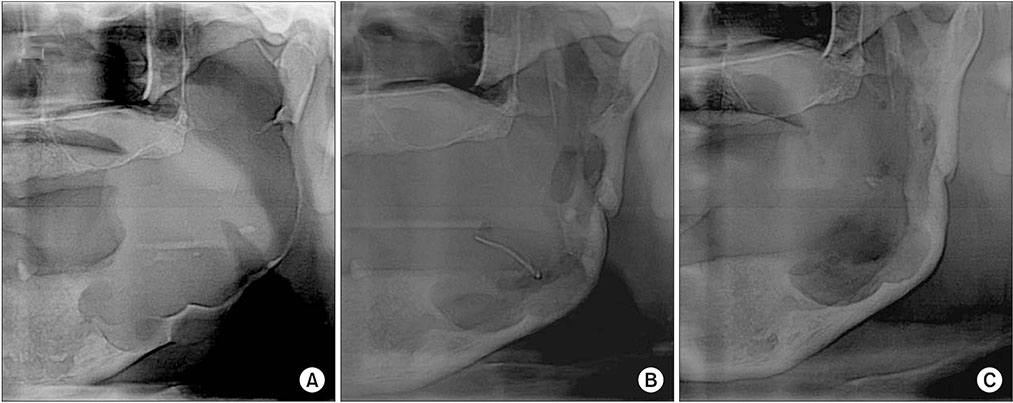
Fig. 5 A. The panoramic radiograph shows a fairly large, well-defined rounded destructive lesion involving the left mandibular body. B. One year after decompression, the panoramic x-ray reveals that the size of the lesion has decreased. C. Three months after surgery, bone formation has progressed well.
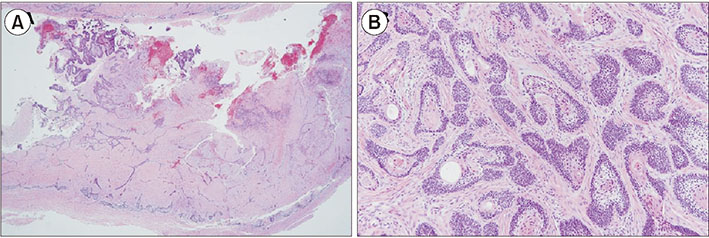
Fig. 6 Microscopic characteristics. A. The tumor is composed of a partly cystic portion and a solid portion (H&E staining, ×20). B. The tumor demonstrates a follicular pattern, which is composed of islands of odontogenic epithelium. The basal cells of these islands are column, hyperchromatic, and palisading. Their centers show squamous differentiation (H&E staining, ×100).
Reference
-
1. Nakamura N, Higuchi Y, Tashiro H, Ohishi M. Marsupialization of cystic ameloblastoma: a clinical and histopathologic study of the growth characteristics before and after marsupialization. J Oral Maxillofac Surg. 1995; 53:748–754. discussion 755-6.2. Ghandhi D, Ayoub AF, Pogrel MA, MacDonald G, Brocklebank LM, Moos KF. Ameloblastoma: a surgeon’s dilemma. J Oral Maxillofac Surg. 2006; 64:1010–1014.
Article3. Haq J, Siddiqui S, McGurk M. Argument for the conservative management of mandibular ameloblastomas. Br J Oral Maxillofac Surg. 2016; 54:1001–1005.
Article4. Kumar V. Conservative surgical approach to aggressive benign odontogenic neoplasm: a report of three cases. J Korean Assoc Oral Maxillofac Surg. 2015; 41:37–42.
Article5. Borrello R, Bettio E, Bacci C, Valente M, Sivolella S, Mazzoleni S, et al. A conservative approach to a peripheral ameloblastoma. Case Rep Dent. 2016; 2016:8254571.
Article6. Chae MP, Smoll NR, Hunter-Smith DJ, Rozen WM. Establishing the natural history and growth rate of ameloblastoma with implications for management: systematic review and meta-analysis. PLoS One. 2015; 10:e0117241.
Article7. Pogrel MA, Montes DM. Is there a role for enucleation in the management of ameloblastoma? Int J Oral Maxillofac Surg. 2009; 38:807–812.
Article8. Gardner DG. Some current concepts on the pathology of ameloblastomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 82:660–669.
Article9. Marx RE, Stern D. Oral and maxillofacial pathology: a rationale for diagnosis and treatment. Chicago: Quintessence;2003.10. Garcia NG, Oliveira DT, Rodrigues MT. Unicystic ameloblastoma with mural proliferation managed by conservative treatment. Case Rep Pathol. 2016; 2016:3089540.
Article11. Kiran KRK, George GB, Padiyath S, Rupak S. [Mural unicystic ameloblastoma crossing the midline: a rare case report]. Int J Odontostomat. 2012; 6:97–103.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Literature review & case report : the conservative treatment of unicystic ameloblastoma
- Case report : The conservative treatment of unilocular plexiform ameloblastoma
- Cryosurgical Treatment of Ameloblastoma: Case Report
- Conservative therapy of extensive unicystic ameloblastoma: a case report
- Conservative management (marsupialization) of unicystic ameloblastoma: literature review and a case report
