Anatomical variations and developmental anomalies of the thyroid gland in Ethiopian population: a cadaveric study
- Affiliations
-
- 1Department of Anatomy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia. mituababi@gmail.com
- KMID: 2430191
- DOI: http://doi.org/10.5115/acb.2018.51.4.243
Abstract
- Because of its embryonic origin, the thyroid gland is predisposed to multiple anatomical variations and developmental anomalies. These include the pyramidal lobe, the origin of levator glandular thyroidae, the absence of the isthmus, ectopic thyroid, accessory thyroid tissues, etc. These anatomical variations are clinically significant to surgeons, anatomists, and researchers. The present study was designed to report anatomical variations and developmental anomalies of the thyroid gland in Ethiopian population. The study was conducted on 40 cadavers used for routine dissection classes. The thyroid gland was exposed and observed for any variations and developmental anomalies. The length, width, and thickness of the lobes were measured using a vernier caliper. Differences in the incidence of pyramidal lobe and absence of the isthmus between sexes were tested using a Pearson chi-square test. The mean length, width, and thickness of the right lobe were 4.24 cm, 1.8 cm, and 1.6 cm, respectively, whereas it was 4.08 cm, 1.8 cm, and 1.6 cm, respectively for that of the left lobe. The pyramidal lobe was noted in 52.5% of the cadavers. The levator glandulae thyroidae were prevalent in 40% of the cadavers. The isthmus mainly overlies the 2nd to 4th tracheal rings and was absent in 7.5% of the cadavers. Accessory thyroid tissue and double pyramidal lobes were noted in 2.5% of the cadavers. Most of the variations of the thyroid gland were seen frequently in female but it was not statically significant. Different clinically important and rare variations of the thyroid gland were found.
Figure
-
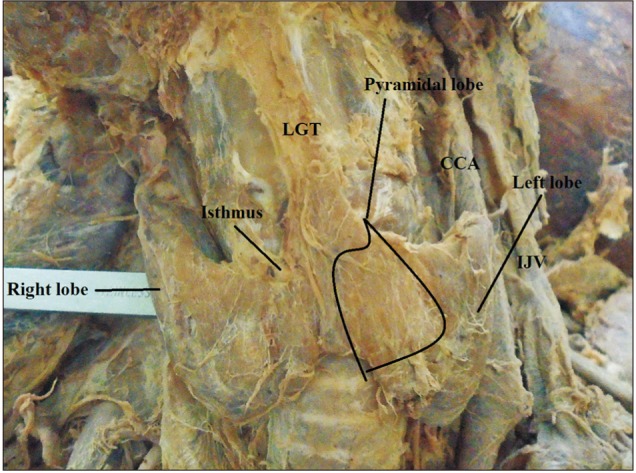
Fig. 1 Pyramidal lobe originating from the central part of the isthmus and its apex attached to hyoid bone by levator glandulae thyroidae (LGT) in male cadaver. CCA, common carotid artery; IJV, internal jugular vein.
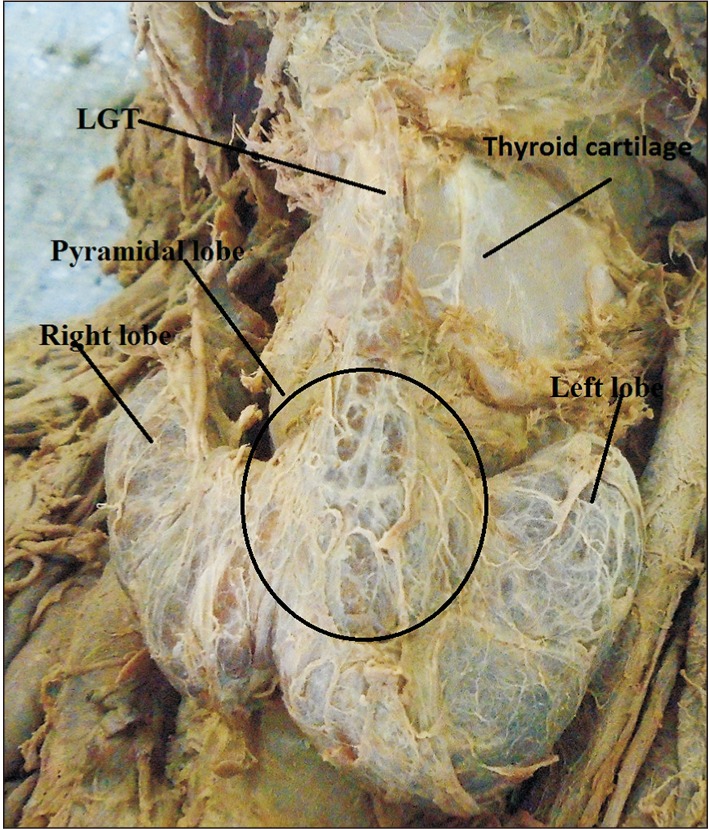
Fig. 2 Pyramidal lobe originating from the junction of the isthmus to the left lobe with levator glandulae thyroidae (LGT) attached to the hyoid bone.
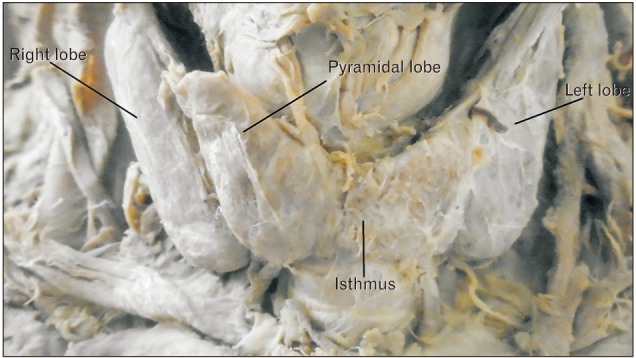
Fig. 3 Pyramidal lobe at the junction of the isthmus to the right lobe with free apex.

Fig. 4 An accessory thyroid tissue overlying the isthmus along with right and left lobes. CCA, common carotid artery; IJV, internal jugular vein.

Fig. 5 The isthmus is absent; the pyramidal lobe originates from the left lobe and attached to the hyoid bone in a female cadaver. LGT, levator glandulae thyroidae.
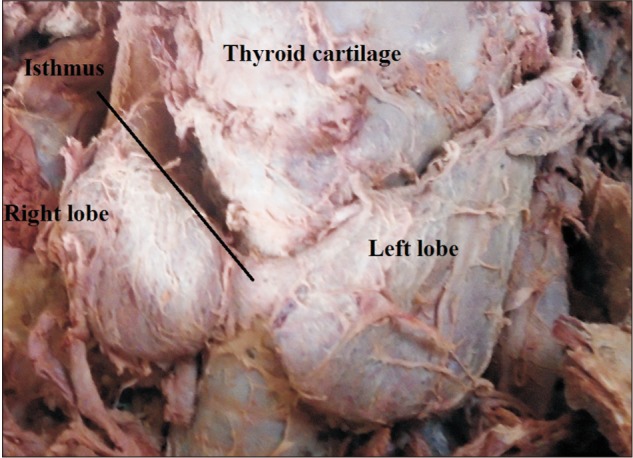
Fig. 6 The right and left lobes of the thyroid gland with a narrow isthmus related to the 3rd tracheal ring.
Reference
-
1. Thiagarajan B. Anatomy of thyroid gland surgeon's perspective. Otolaryngol Online J. 2015; 5:1–9.2. Muktyaz H, Birendra Y, Dhiraj S, Arun SK. Anatomical variations of thyroid gland and its clinical significance in North Indian population. Global J Biol Agric Health Sci. 2013; 2:12–16.3. Gaikwad S, Joshi R. An anatomical study of morphological variations of the thyroid gland. Int J Anat Res. 2016; 4:2665–2669.4. Sinha MB, Siddiqui AU, Sharma DK. Levator glandulae thyroideae: a fibromusculoglandular band: a case report. Indian J Clin Anat Physiol. 2014; 1:57–59.5. Asha S, Dixit D, Shirol VS, Bhimalli S. Study of absence of isthmus of thyroid gland with its developmental and surgical implications in adult human cadavers: a case series. Med Innov. 2013; 2:50–52.6. Reddy CK, Panchakshari M. A study of anatomical and morphological variations of the thyroid gland. Sch J Appl Med Sci. 2016; 4:3510–3513.7. Rajkonwar AJ, Kusre G. Morphological variations of the thyroid gland among the people of upper Assam region of northeast India: a cadaveric study. J Clin Diagn Res. 2016; 10:AC01–AAC3.8. Şeker S, TaŞ İ. Determination of thyroid volume and its relation with isthmus thickness. Eur J Gen Med. 2010; 7:125–129.9. Nikumbh RD, Nikumbh DB, Doshi MA. Multiple morphological variations in the thyroid gland: report of two cases. Int J Anat Res. 2015; 3:1476–1480.10. Onwuaso IC, Samuel MN, Nwagbo ED. Age-related morphological changes in the foetal thyroid gland of white Fulani (Zebu) cattle. Indian J Anim Res. 2014; 48:438–443.11. Joshi SD, Joshi SS, Daimi SR, Athavale SA. The thyroid gland and its variations: a cadaveric study. Folia Morphol (Warsz). 2010; 69:47–50. PMID: 20235050.12. Moore K, Persaud TV, Torchia M. The developing human: clinical oriented embryology. 10th ed. Philadelphia, PA: Saunders;2015.13. Chaudhary P, Singh Z, Khullar M, Arora K. Levator glandulae thyroideae, a fibromusculoglandular band with absence of pyramidal lobe and its innervation: a case report. J Clin Diagn Res. 2013; 7:1421–1424. PMID: 23998080.14. Lokanadham S, Satheesh Naik K, Subhadra Devi V. Thyroid gland isthmus agenesis in autopsied fetus: case study. Prime Res Med. 2012; 2:69–71.15. Milojevic B, Tosevski J, Milisavljevic M, Babic D, Malikovic A. Pyramidal lobe of the human thyroid gland: an anatomical study with clinical implications. Rom J Morphol Embryol. 2013; 54:285–289. PMID: 23771071.16. Geraci G, Pisello F, Li Volsi F, Modica G, Sciumè C. The importance of pyramidal lobe in thyroid surgery. G Chir. 2008; 29:479–482. PMID: 19068184.17. Hakeem AH, Hakeem IH, Wani FJ. Double pyramidal lobe of thyroid gland: a rare presentation. Thyroid Res Pract. 2016; 13:25–26.18. Zivic R, Radovanovic D, Vekic B, Markovic I, Dzodic R, Zivaljevic V. Surgical anatomy of the pyramidal lobe and its significance in thyroid surgery. S Afr J Surg. 2011; 49:110. PMID: 21933507.19. Sinos G, Sakorafas GH. Pyramidal lobe of the thyroid: anatomical considerations of importance in thyroid cancer surgery. Oncol Res Treat. 2015; 38:309–310. PMID: 26045028.20. Kotisso B, Ersumo T, Ali A, Wassie A. Thyroid disease in Tikur Anbessa Hospital: a five-year review. Ethiop Med J. 2004; 42:205–209. PMID: 16895039.21. Debebe K, Genetu G, Feleke Y, Kebede T. Pattern, clinical presentation and pregnancy outcome of thyroid diseases in pregnant women at national endocrine referral clinic of Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia from june 2010 to june 2015. J Thyroid Disord Ther. 2017; 6:209.22. Abuye C, Berhane Y, Akalu G, Getahun Z, Ersumo T. Prevalence of goiter in children 6 to 12 years of age in Ethiopia. Food Nutr Bull. 2007; 28:391–398. PMID: 18274165.23. Won SY. Anatomical considerations of the superior thyroid artery: its origins, variations, and position relative to the hyoid bone and thyroid cartilage. Anat Cell Biol. 2016; 49:138–142. PMID: 27382516.24. Prakash , Rajini T, Ramachandran A, Savalgi GB, Venkata SP, Mokhasi V. Variations in the anatomy of the thyroid gland: clinical implications of a cadaver study. Anat Sci Int. 2012; 87:45–49. PMID: 21956789.25. Ranade AV, Rai R, Pai MM, Nayak SR, Prakash , Krisnamurthy A, Narayana S. Anatomical variations of the thyroid gland: possible surgical implications. Singapore Med J. 2008; 49:831–834. PMID: 18946620.26. Standring S. Gray's anatomy: the anatomical basis of clinical practice. London: Elsevier Churchill Livingstone;2005.27. Dixit D, Shilpa MB, Harsh MP, Ravishankar MV. Agenesis of isthmus of thyroid gland in adult human cadavers: a case series. Cases J. 2009; 2:6640. PMID: 20181171.28. Rashid SQ. Thyroid gland standard for Bangladeshi population and prevalence of unknown pathologies in the normal population. J Med Ultrasound. 2016; 24:101–106.29. Braun EM, Windisch G, Wolf G, Hausleitner L, Anderhuber F. The pyramidal lobe: clinical anatomy and its importance in thyroid surgery. Surg Radiol Anat. 2007; 29:21–27. PMID: 17146601.30. Moore KL, Dalley AF. Clinically oriented anatomy. 5th ed. Toronto: Lippincott Williams & Wilkins;2006.31. Gurleyik E, Gurleyik G, Dogan S, Cobek U, Cetin F, Onsal U. Pyramidal lobe of the thyroid gland: surgical anatomy in patients undergoing total thyroidectomy. Anat Res Int. 2015; 2015:384148. PMID: 26236507.32. Kaklamanos I, Zarokosta M, Flessas I, Zoulamoglou M, Katsoulas T, Birbas K, Troupis T, Mariolis-Sapsakos T. Surgical anatomy of double pyramidal lobe on total thyroidectomy: a rare case report. J Surg Case Rep. 2017; 2017:rjx035. PMID: 28458845.33. Ignjatović M. Double pyramidal thyroid lobe. J Postgrad Med. 2009; 55:41–42. PMID: 19242079.34. Kulkarni V, Sreepadma S, Deshpande SK. Morphological variations ot the thyroid gland. Med Innov. 2012; 1:35–38.35. Sawant DA, Moore TF. An unusual course of segmental renal artery displays a rare case of hilar nutcracker phenomenon. Case Rep Med. 2015; 2015:249015. PMID: 26448765.36. Snell RS. Clinical anatomy by regions. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2008.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomical considerations of the superior thyroid artery: its origins, variations, and position relative to the hyoid bone and thyroid cartilage
- Coexistence of multiple anomalies in the hepatobiliary system
- A Case of Contemporaneous Occurrence of Thyroglossal Duct Cyst and Lingual Thyroid without the Orthotopic Thyroid Gland
- Monitoring the Bifurcated Recurrent Laryngeal Nerve
- Morphologic Variations of the Thyroid Gland in Korean Adults
