Ann Rehabil Med.
2018 Oct;42(5):773-776. 10.5535/arm.2018.42.5.773.
Spinal Accessory Nerve Injury Induced by Manipulation Therapy: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. coltrane@catholic.ac.kr
- KMID: 2429207
- DOI: http://doi.org/10.5535/arm.2018.42.5.773
Abstract
- Spinal accessory nerve (SAN) injury mostly occurs during surgical procedures. SAN injury caused by manipulation therapy has been rarely reported. We present a rare case of SAN injury associated with manipulation therapy showing scapular winging and droopy shoulder. A 42-year-old woman visited our outpatient clinic complaining of pain and limited active range of motion (ROM) in right shoulder and scapular winging after manipulation therapy. Needle electromyography and nerve conduction study suggested SAN injury. Physical therapy (PT) three times a week for 2 weeks were prescribed. After a total of 6 sessions of PT and modality, the patient reported that the pain was gradually relieved during shoulder flexion and abduction with improved active ROM of shoulder. Over the course of 2 months follow-up, the patient reported almost recovered shoulder ROM and strength as before. She did not complain of shoulder pain any more.
Keyword
MeSH Terms
Figure
-
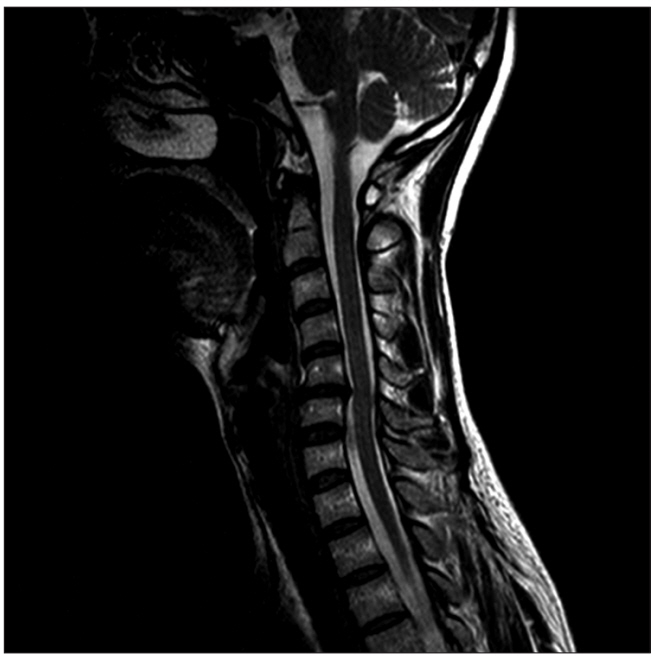
Fig. 1. Cervical magnetic resonance imaging revealing herniated nucleus pulposus in C4-5 and C5-6.
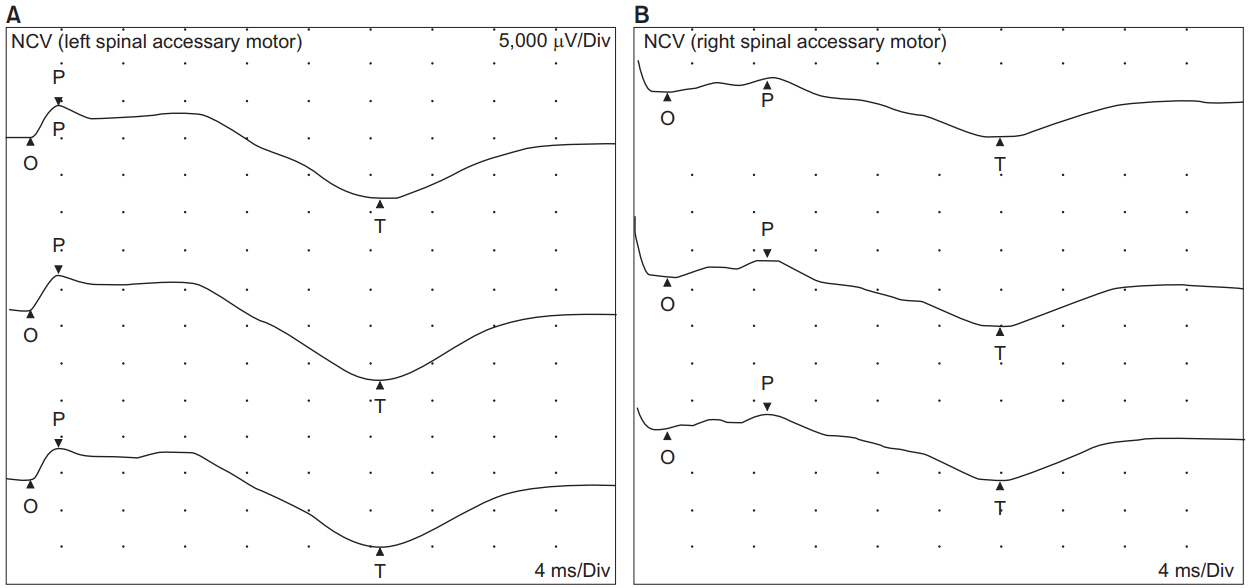
Fig. 2. (A) Normal ranges of onset latency and amplitude of compound muscle action potential (CMAP) in the left upper trapezius muscle. (B) Delayed onset latency and decreased amplitude of CMAP in the right upper trapezius muscle.
Reference
-
1. Aksoy IA, Schrader SL, Ali MS, Borovansky JA, Ross MA. Spinal accessory neuropathy associated with deep tissue massage: a case report. Arch Phys Med Rehabil. 2009; 90:1969–72.
Article2. Bodack MP, Tunkel RS, Marini SG, Nagler W. Spinal accessory nerve palsy as a cause of pain after whiplash injury: case report. J Pain Symptom Manag. 1998; 15:321–8.3. Wills AJ, Sawle GV. Accessory nerve palsies. Pract Neurol. 2010; 10:191–4.
Article4. Porter P, Fernandez GN. Stretch-induced spinal accessory nerve palsy: a case report. J Shoulder Elbow Surg. 2001; 10:92–4.
Article5. Lu L, Haman SP, Ebraheim NA. Vulnerability of the spinal accessory nerve in the posterior triangle of the neck: a cadaveric study. Orthopedics. 2002; 25:71–4.
Article6. Coulter JM, Warme WJ. Complete spinal accessory nerve palsy from carrying climbing gear. Wilderness Environ Med. 2015; 26:384–6.
Article7. Kelley MJ, Kane TE, Leggin BG. Spinal accessory nerve palsy: associated signs and symptoms. J Orthop Sports Phys Ther. 2008; 38:78–86.
Article8. Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003; 11:142–51.
Article9. Hsu PC, Chiu JW, Chou CL, Wang JC. Acute radial neuropathy at the spiral groove following massage: a case presentation. PM R. 2017; 9:1042–6.
Article10. Ernst E. Manipulation of the cervical spine: a systematic review of case reports of serious adverse events, 1995-2001. Med J Aust. 2002; 176:376–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Anatomical Study on the Variations of the First Cervical Dorsal Root
- A Case of Spinal Accessory Neurilemmoma
- The Number of the Spinal Rootlets of the Accessory Nerve and Their Most Caudal Level on Spinal Cord
- Delayed Spinal Accessory Neuropathy Diagnosed after Local Operative Surgical Procedures in The Posterior Cervical Triangle
- Intracisternal Cranial Root Accessory Nerve Schwannoma Associated with Recurrent Laryngeal Neuropathy
