Management of High Ankle Sprain
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea. leejy88@chosun.ac.kr
- KMID: 2428653
- DOI: http://doi.org/10.14193/jkfas.2018.22.4.145
Abstract
- High ankle sprain (distal tibiofibular syndesmosis injury) occurs from rotational injuries, specifically external rotation, and may be associated with ankle fractures. The prevalence of these injuries may be higher than previously reported because they may be missed in an initial examination. Syndesmosis injury can lead to significant complications in injured ankle joints, so a precise physical examination and radiological evaluation is necessary. The most important treatment goal is to have the tibia and fibula located in the correct position with respect to each other and to heal in that position. The methods to fix these injuries is controversial.
Keyword
Figure
-

Figure 1 Illustration of the ligamentous anatomy of the syndesmosis: anterior-inferior tibiofibular ligament (AITFL), interosseous membrane (IOM), interosseous ligament (IOL), posterior-inferior tibiofibular ligament (PITFL), and transverse tibiofibular ligament (TTL).
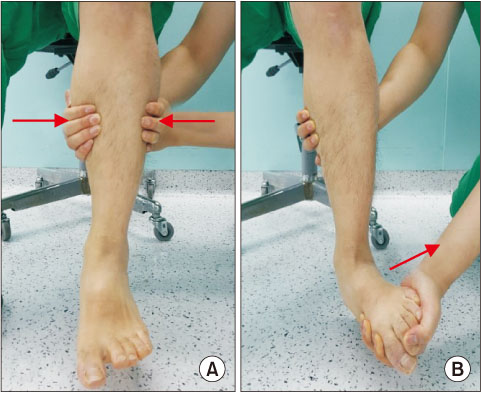
Figure 2 (A) Sqeeze test is performed by compressive force is applied between fibula and tibia above midpoint of calf. Test is considered If produces distal pain. (B) External rotation test is positive if pain is reproduced with external rotation of the foot and ankle relative to the tibia.
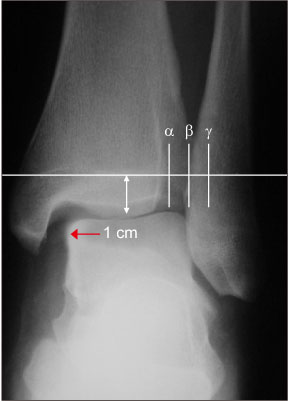
Figure 3 Anterior posterior radiograph of the ankle joint demonstrating important landmarks checked above 1 cm of distal tibial articular line. α to β distance is a tibio-fibular clear space, β to γ distance is a tibiofibular overlap, and red arrow indicates medial clear space. α: lateral border of posterior tibial malleolus, β: medial border of fibula, γ: lateral border of anterior tibial tubercle.
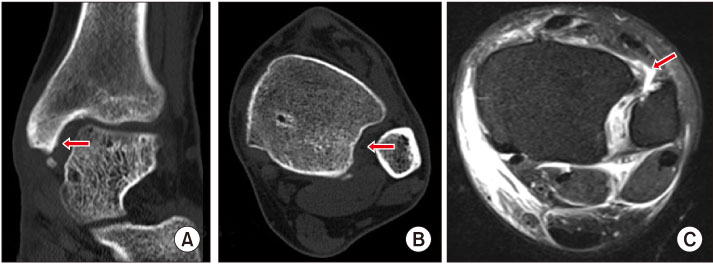
Figure 4 (A) Coronal section of the ankle joint computed tomography (CT) showed medial clear space widening with avulsion fragment of medial malleolus (arrow). (B) Axial section of the ankle joint CT showed widening of syndesmosis (arrow). (C) Axial T2-weighted magnetic resonance image of the ankle joint magnetic resonance imaging showed ruptured anterior-inferior tibiofibular ligament (arrow).

Figure 5 Intraoperative fluoroscopic image. (A) Image showed widening of syndesmosis. (B) Syndesmosis reduction performed by using large reduction clamp. (C) And then the syndesmosis fixation with single 4.5 mm screws was performed.
Reference
-
1. van den Bekerom MP, Lamme B, Hogervorst M, Bolhuis HW. Which ankle fractures require syndesmotic stabilization? J Foot Ankle Surg. 2007; 46:456–463.
Article2. Clanton TO, Paul P. Syndesmosis injuries in athletes. Foot Ankle Clin. 2002; 7:529–549.
Article3. Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br. 2008; 90:405–410.
Article4. Marti RK, Raaymakers EL, Nolte PA. Malunited ankle fractures. The late results of reconstruction. J Bone Joint Surg Br. 1990; 72:709–713.
Article5. Rammelt S, Zwipp H, Grass R. Injuries to the distal tibiofibular syndesmosis: an evidence-based approach to acute and chronic lesions. Foot Ankle Clin. 2008; 13:611–633. vii–viii.
Article6. Ogilvie-Harris DJ, Reed SC. Disruption of the ankle syndesmosis: diagnosis and treatment by arthroscopic surgery. Arthroscopy. 1994; 10:561–568.
Article7. Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005; 19:604–609.
Article8. Peña FA, Coetzee JC. Ankle syndesmosis injuries. Foot Ankle Clin. 2006; 11:35–50. viii
Article9. Markolf KL, Jackson SR, McAllister DR. Syndesmosis fixation using dual 3.5 mm and 4.5 mm screws with tricortical and quadricortical purchase: a biomechanical study. Foot Ankle Int. 2013; 34:734–739.
Article10. Harris IA, Jones HP. The fate of the syndesmosis in type C ankle fractures: a cadaveric study. Injury. 1997; 28:275–277.
Article11. Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007; 15:330–339.
Article12. Sikka RS, Fetzer GB, Sugarman E, Wright RW, Fritts H, Boyd JL, et al. Correlating MRI findings with disability in syndesmotic sprains of NFL players. Foot Ankle Int. 2012; 33:371–378.
Article13. Sman AD, Hiller CE, Rae K, Linklater J, Black DA, Nicholson LL, et al. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br J Sports Med. 2015; 49:323–329.
Article14. Wuest TK. Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg. 1997; 5:172–181.
Article15. Pneumaticos SG, Noble PC, Chatziioannou SN, Trevino SG. The effects of rotation on radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle Int. 2002; 23:107–111.
Article16. Takao M, Ochi M, Oae K, Naito K, Uchio Y. Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J Bone Joint Surg Br. 2003; 85:324–329.17. Ebraheim NA, Elgafy H, Padanilam T. Syndesmotic disruption in low fibular fractures associated with deltoid ligament injury. Clin Orthop Relat Res. 2003; (409):260–267.
Article18. Heim D, Heim U, Regazzoni P. [Malleolar fractures with ankle joint instability--experience with the positioning screw]. Unfallchirurgie. 1993; 19:307–312. German.19. Jones CB, Gilde A, Sietsema DL. Treatment of syndesmotic injuries of the ankle: a critical analysis review. JBJS Rev. 2015; 3:DOI: 10.2106/JBJS.RVW.N.00083.20. Thompson MC, Gesink DS. Biomechanical comparison of syndesmosis fixation with 3.5- and 4.5-millimeter stainless steel screws. Foot Ankle Int. 2000; 21:736–741.
Article21. Needleman RL, Skrade DA, Stiehl JB. Effect of the syndesmotic screw on ankle motion. Foot Ankle. 1989; 10:17–24.
Article22. Andersen MR, Frihagen F, Hellund JC, Madsen JE, Figved W. Randomized trial comparing suture button with single syndesmotic screw for syndesmosis injury. J Bone Joint Surg Am. 2018; 100:2–12.
Article23. Degroot H, Al-Omari AA, El Ghazaly SA. Outcomes of suture button repair of the distal tibiofibular syndesmosis. Foot Ankle Int. 2011; 32:250–256.
Article24. Thornes B, Walsh A, Hislop M, Murray P, O'Brien M. Sutureendobutton fixation of ankle tibio-fibular diastasis: a cadaver study. Foot Ankle Int. 2003; 24:142–146.
Article25. McBryde A, Chiasson B, Wilhelm A, Donovan F, Ray T, Bacilla P. Syndesmotic screw placement: a biomechanical analysis. Foot Ankle Int. 1997; 18:262–266.
Article26. Kukreti S, Faraj A, Miles JN. Does position of syndesmotic screw affect functional and radiological outcome in ankle fractures? Injury. 2005; 36:1121–1124.
Article27. Tornetta P 3rd, Spoo JE, Reynolds FA, Lee C. Overtightening of the ankle syndesmosis: is it really possible? J Bone Joint Surg Am. 2001; 83:489–492.
Article28. Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle Int. 1997; 18:693–698.
Article29. Song DJ, Lanzi JT, Groth AT, Drake M, Orchowski JR, Shaha SH, et al. The effect of syndesmosis screw removal on the reduction of the distal tibiofibular joint: a prospective radiographic study. Foot Ankle Int. 2014; 35:543–548.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Severe Open Ankle Sprain (SOAS): A Case Report
- Evidence-based Treatment of Acute Lateral Ankle Sprain
- Conservative Management of Ankle Sprains
- The Effect of 2 Hz and 100 Hz Electrical Stimulation of Acupoint on Ankle Sprain in Rats
- Acute Anterior Talofibular Ligament Open Type Avulsion Fracture: A Case Report
