Early Lateral Compartment Physeal Closure of the Elbow in Osteochondritis Dissecans of the Adolescent Baseball Players
- Affiliations
-
- 1Department of Orthopaedic Surgery, Good Samsun Hospital, Busan, Korea. 214077@goodhospital.or.kr
- KMID: 2428001
- DOI: http://doi.org/10.5763/kjsm.2018.36.4.180
Abstract
- PURPOSE
The purpose of this study is to identify bilateral differences of physeal closure of the lateral compartment of the elbow in osteochondritis dissecans (OCD) and related factors with premature physeal closure.
METHODS
Initial radiographs of the bilateral elbows in 40 baseball players with OCD (group I) were reviewed for the status of physeal closure of the lateral compartment; capitellum, radial head, lateral epicondyle. Forty baseball players with medial epicondylar apophysitis (group II) were enrolled as a control. Relative status of physeal closure of dominant elbow was defined as early, same, and delayed. Bilateral differences of the status of physeal closure were analyzed between groups, and according to the radiographic stages, extent of the lesions and demographic factors in group I.
RESULTS
Significant early physeal closures of dominant elbows were identified in group I in capitellum (group I, 55%; group II, 3%), radial head (group I, 53%; group II, 3%), and lateral epicondyle (group I 37%; group II, 5%). In group I, advanced stage and extended lesion showed early lateral compartment physeal closure especially in capitellum and radial head, and players with longer career length and limitation of motion showed early closure.
CONCLUSION
Over the half of the adolescent baseball players with OCD demonstrated early radiocapitellar physeal closures of dominant elbow in initial presentation. Because premature physeal closure contributes to the development of arthritis without appropriate radiocapitellar remodeling, early detection of OCD is essential for prevention of arthritis and successful conservative management.
Keyword
MeSH Terms
Figure
-
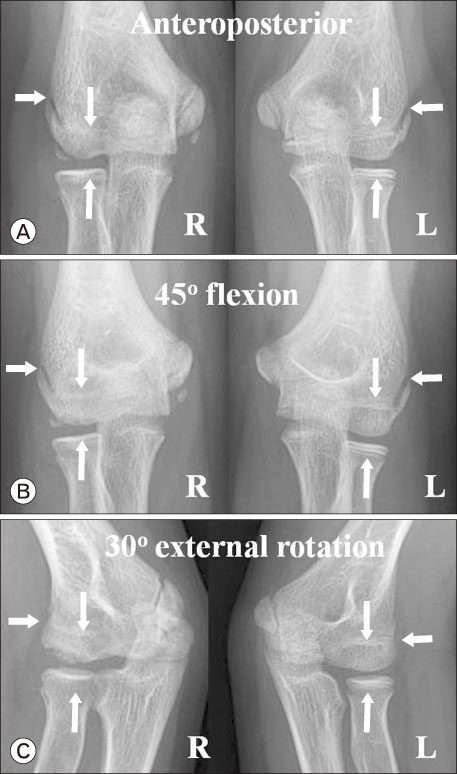
Fig. 1 Bilateral plain radiographs of 12-year-old pitcher with osteochondritis dissecans in right (R) elbow. (A) Anteroposterior, (B) 45° flexion anteroposterior, and (C) 30o external rotation oblique views show earlier physeal closure than left (L) elbow in capitellum, radial head, and lateral epicondyle. Arrows indicate each lateral compartment physes; lateral epicondyle, capitellum, radial head.
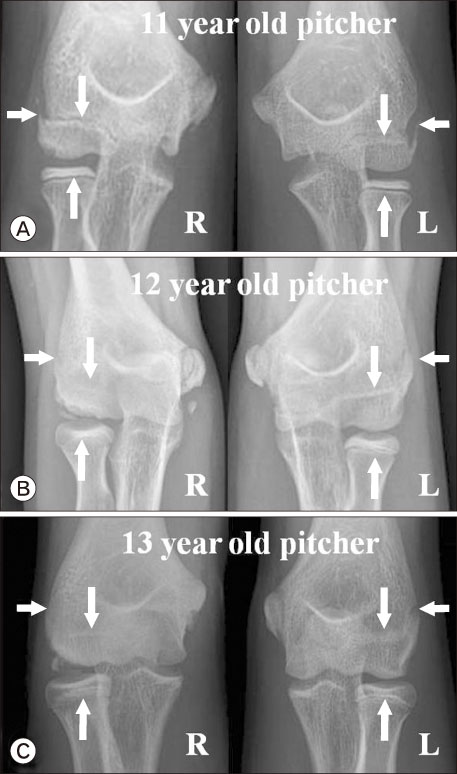
Fig. 2 Bilateral 45° flexion anteroposterior plain radiographs according to the stage of osteochondritis dissecans. (A) Eleven-year-old pitcher in radiolucent stage showed same status of lateral compartment physeal closure in both elbow. (B) Twelve-year-old pitcher in fragmentation stage showed earlier lateral compartment physeal closure than nondominant elbow. (C) Thirteen-year-old pitcher in free stage also showed earlier lateral compartment physeal closure. Arrows indicate each lateral compartment physes; lateral epicondyle, capitellum, radial head. R: right, L: left.

Fig. 3 Bilateral 30° external rotation oblique plain radiographs according to the grade of osteochondritis dissecans. (A) Twelve-year-old pitcher with localized lateral type showed same status of lateral compartment physeal closure in both elbow. (B) Twelve-year-old fielder with radiolucent central type stage also showed same status. (C) Twelve-year-old pitcher with large fragmented central type showed earlier lateral compartment physeal closure than nondominant elbow. (D) Twelve-year-old fielder with extended lateral type showed premature lateral compartment physeal closure and asymmetry of radial head morphology. Arrows indicate each lateral compartment physes; lateral epicondyle, capitellum, radial head. R: right, L: left.
Reference
-
1. Cain EL Jr, Dugas JR, Wolf RS, Andrews JR. Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med. 2003; 31:621–635.
Article2. Yadao MA, Field LD, Savoie FH 3rd. Osteochondritis dissecans of the elbow. Instr Course Lect. 2004; 53:599–606.3. Ruchelsman DE, Hall MP, Youm T. Osteochondritis dissecans of the capitellum: current concepts. J Am Acad Orthop Surg. 2010; 18:557–567.
Article4. Takahara M, Mura N, Sasaki J, Harada M, Ogino T. Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum. J Bone Joint Surg Am. 2007; 89:1205–1214.
Article5. Mihara K, Tsutsui H, Nishinaka N, Yamaguchi K. Nonoperative treatment for osteochondritis dissecans of the capitellum. Am J Sports Med. 2009; 37:298–304.
Article6. Mihata T, Quigley R, Robicheaux G, McGarry MH, Neo M, Lee TQ. Biomechanical characteristics of osteochondral defects of the humeral capitellum. Am J Sports Med. 2013; 41:1909–1914.
Article7. Wu M, Eisenberg K, Williams K, Bae DS. Radial head changes in osteochondritis dissecans of the humeral capitellum. Orthop J Sports Med. 2018; 6:2325967118769059.
Article8. Caine D, DiFiori J, Maffulli N. Physeal injuries in children's and youth sports: reasons for concern. Br J Sports Med. 2006; 40:749–760.
Article9. Sato T, Shinozaki T, Fukuda T, et al. Atypical growth plate closure: a possible chronic Salter and Harris type V injury. J Pediatr Orthop B. 2002; 11:155–158.
Article10. Minami M, Nakashita K, Ishii S, et al. Twenty-five cases of osteochondritis dissecans of the elbow. Rinsho Seikei Geka. 1979; 14:805–810.11. Kosaka M, Nakase J, Takahashi R, et al. Outcomes and failure factors in surgical treatment for osteochondritis dissecans of the capitellum. J Pediatr Orthop. 2013; 33:719–724.
Article12. Takahara M, Ogino T, Sasaki I, Kato H, Minami A, Kaneda K. Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop Relat Res. 1999; (363):108–115.
Article13. Takahara M, Ogino T, Takagi M, Tsuchida H, Orui H, Nambu T. Natural progression of osteochondritis dissecans of the humeral capitellum: initial observations. Radiology. 2000; 216:207–212.
Article14. Davies DA, Parsons FG. The age order of the appearance and union of the normal epiphyses as seen by X-rays. J Anat. 1927; 62(Pt 1):58–71.15. Yamaguchi K, Sweet FA, Bindra R, Morrey BF, Gelberman RH. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am. 1997; 79:1653–1662.16. Schenck RC Jr, Athanasiou KA, Constantinides G, Gomez E. A biomechanical analysis of articular cartilage of the human elbow and a potential relationship to osteochondritis dissecans. Clin Orthop Relat Res. 1994; (299):305–312.
Article17. Keret D, Mendez AA, Harcke HT, MacEwen GD. Type V physeal injury: a case report. J Pediatr Orthop. 1990; 10:545–548.
Article18. Matsui Y, Funakoshi T, Momma D, et al. Variation in stress distribution patterns across the radial head fovea in osteochondritis dissecans: predictive factors in radiographic findings. J Shoulder Elbow Surg. 2018; 27:923–930.
Article19. Weinstein SL, Dolan LA. Proximal femoral growth disturbance in developmental dysplasia of the hip: what do we know? J Child Orthop. 2018; 12:331–341.
Article20. Bowen JR, Schreiber FC, Foster BK, Wein BK. Premature femoral neck physeal closure in Perthes' disease. Clin Orthop Relat Res. 1982; (171):24–29.
Article21. Kida Y, Morihara T, Kotoura Y, et al. Prevalence and clinical characteristics of osteochondritis dissecans of the humeral capitellum among adolescent baseball players. Am J Sports Med. 2014; 42:1963–1971.
Article22. Matsuura T, Suzue N, Iwame T, Nishio S, Sairyo K. Prevalence of osteochondritis dissecans of the capitellum in young baseball players: results based on ultrasonographic findings. Orthop J Sports Med. 2014; 2:2325967114545298.23. Oh Y, Lee R, Kim HS. Evaluation of skeletal maturity score for Korean children and the standard for comparison of bone age and chronological age in normal children. J Pediatr Endocrinol Metab. 2012; 25:279–284.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Glenoid Lesions on Magnetic Resonance Imaging in Adolescent Baseball Players
- Osteochondritis Dissecans of the Capitellum Humeri: Surgical Treatment and Resuls
- Osteochondritis Dissecans in Medial Trochlea of the Humerus in a Pitcher: A Case Report
- Osteochondritis Dissecans of the Capitellum Humeri: Analysis of C. T. Findings
- Osteochondritis Dissecans of the Knee
