Imaging Patterns of Intratumoral Calcification in the Abdominopelvic Cavity
- Affiliations
-
- 1Department of Radiology, Konkuk University Medical Center, Seoul 05030, Korea. yjkim@kuh.ac.kr
- KMID: 2427944
- DOI: http://doi.org/10.3348/kjr.2017.18.2.323
Abstract
- Intratumoral calcification is one of the most noticeable of radiologic findings. It facilitates detection and provides information important for correctly diagnosing tumors. In the abdominopelvic cavity, a wide variety of tumors have calcifications with various imaging features, though the majority of such calcifications are dystrophic in nature. In this article, we classify the imaging patterns of intratumoral calcification according to number, location, and morphology. Then, we describe commonly-encountered abdominopelvic tumors containing typical calcification patterns, focusing on their differentiable characteristics using the imaging patterns of intratumoral calcification.
Keyword
MeSH Terms
-
Abdominal Neoplasms/complications/*diagnosis/diagnostic imaging
Adenocarcinoma, Mucinous/diagnosis/diagnostic imaging/pathology
Adult
Aged
Calcinosis/complications/*diagnosis/diagnostic imaging
Female
Humans
Image Interpretation, Computer-Assisted
Liver Neoplasms/diagnosis/diagnostic imaging/pathology
Male
Middle Aged
Neoplasm Metastasis
Pancreatic Neoplasms/diagnosis/diagnostic imaging/pathology
Figure
-
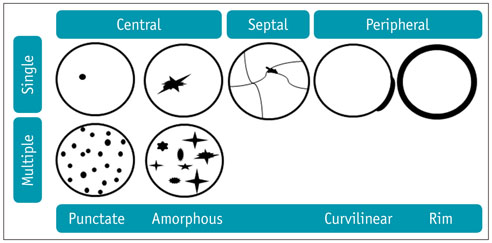
Fig. 1 Imaging patterns of intratumoral calcification according to number, location, and morphology. Calcification is seen–in tumors–in single or multiple form, and can be located in center or peripheral portion of tumor, or at internal septa (septal). Punctate (round), amorphous (irregularly shaped), curvilinear (curved line), or rim (eggshell, cyst-wall like appearance) calcification is in evidence.
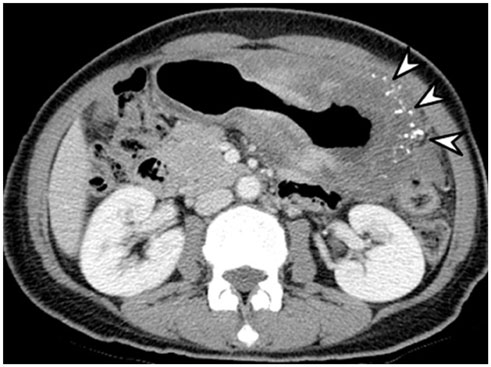
Fig. 2 Mucinous adenocarcinoma of stomach in 60-year-old female. Axial contrast-enhanced CT image shows diffuse, low-attenuated wall thickening containing multiple punctate calcifications (arrowheads) involving high-to-low body of stomach. These CT findings are characteristic imaging features of gastric mucinous adenocarcinoma.

Fig. 3 Mucinous adenocarcinoma of colon in 22-year-old female. Coronal contrast-enhanced CT image reveals segmental, low-attenuated wall thickening (arrow) at descending colon, causing upstream colonic obstruction (asterisk). Several punctate calcifications (arrowheads) are seen in low-attenuated, thickened colon wall. Patient underwent left hemicolectomy and was diagnosed with mucinous adenocarcinoma.
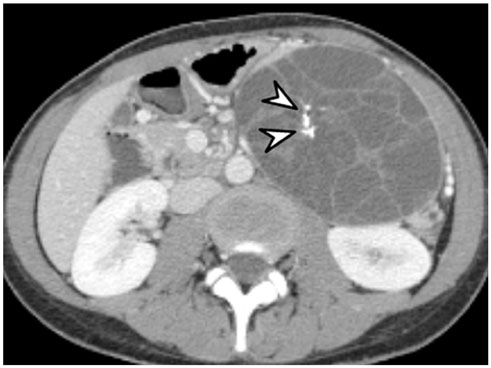
Fig. 4 Mucinous cystic neoplasm of pancreas in 31-year-old female. Axial contrast-enhanced CT image demonstrates large, well-defined, low-attenuated cystic mass with multiple internal septa in pancreatic tail (not shown). Typical septal calcifications (arrowheads) are noted within lesion. Distal pancreatectomy was performed, and mucinous cystic neoplasm was diagnosed.
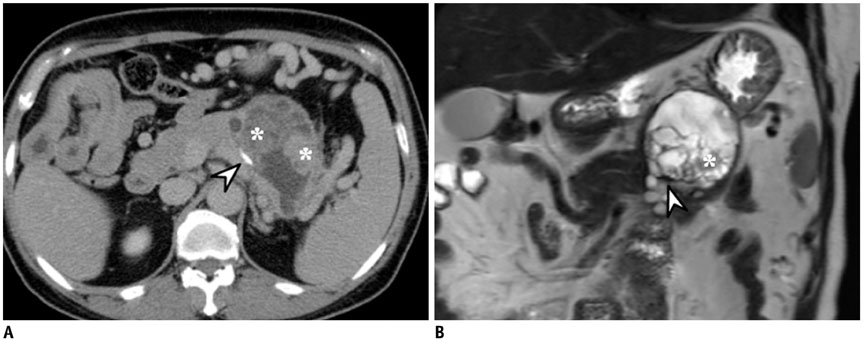
Fig. 5 Mucinous cystic neoplasm of pancreas in 51-year-old female. A. Bulging, contoured, low-attenuated cystic mass in pancreatic tail is seen on axial contrast-enhanced CT image. There are multifocal enhancing solid components (asterisks) in mass, and peripheral curvilinear calcification (arrowhead) is also in evidence. B. This coronal T2-weighted MR image demonstrates presence of cystic mass with internal solid portion (asterisk). Peripheral curvilinear calcification (arrowhead) of lesion is seen as region of hyposignal intensity. After distal pancreatectomy, mucinous cystic neoplasm with associated invasive carcinoma was diagnosed.
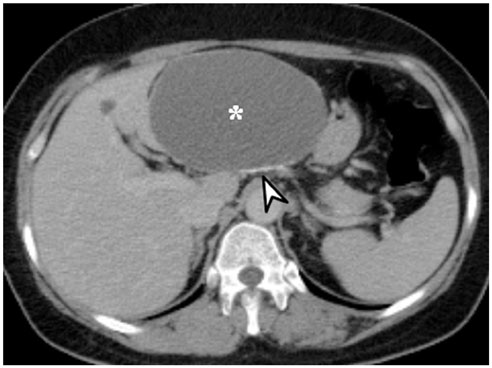
Fig. 6 Mucinous cystic neoplasm of liver in 56-year-old female. Large, well-defined, unilocular cystic mass (asterisk) is located in left lateral section of liver as shown on axial contrast-enhanced CT image. Peripheral curvilinear calcification (arrowhead) is noted, and there is no enhancing solid component. Hepatic segmentectomy was performed, and lesion was confirmed as being mucinous cystic neoplasm (biliary cystadenoma) with dystrophic calcification and containing internal hemorrhage.

Fig. 7 Mucinous cystic neoplasm of liver, in 75-year-old female. A. On axial pre-contrast CT image, lobulating, contoured cystic mass is located in segment 7 of liver. Fine septal calcifications (arrowheads) are seen. B. On ultrasound scan, fine septal calcifications (arrowheads), within cystic mass, are seen as echogenic lesions with posterior acoustic shadowing. After hepatic tumorectomy, mucinous cystic neoplasm (biliary cystadenoma) was diagnosed.
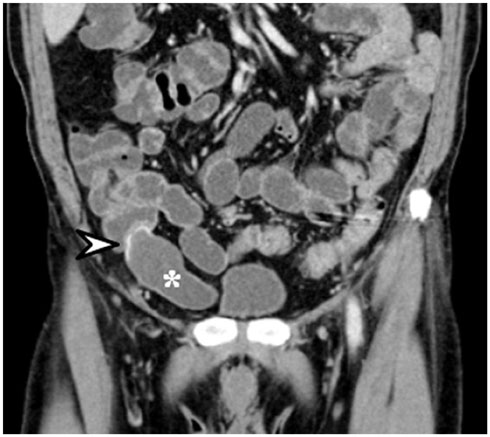
Fig. 8 Mucinous neoplasm of appendix in 61-year-old male. Coronal contrast-enhanced CT image demonstrates cystic dilatation of appendix (asterisk) without evidence of acute inflammation. Curvilinear calcification (arrowhead) is seen at proximal appendiceal wall. Appendectomy was performed, and low-grade appendiceal mucinous neoplasm was diagnosed.
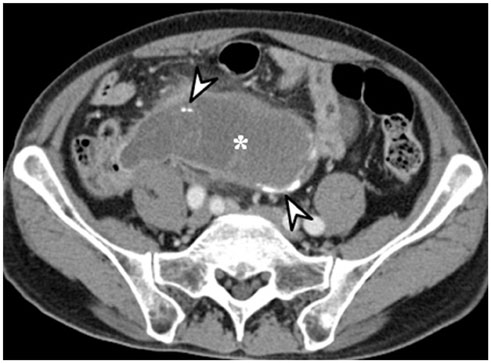
Fig. 9 Mucinous adenocarcinoma of appendix in 72-year-old male. Axial contrast-enhanced CT image reveals cystic dilatation of appendix (asterisk) with peripheral, curvilinear calcifications (arrowheads). Internal, mild enhancing solid portions and perilesional fatty infiltrations are demonstrated. After appendectomy, mucinous adenocarcinoma was diagnosed.
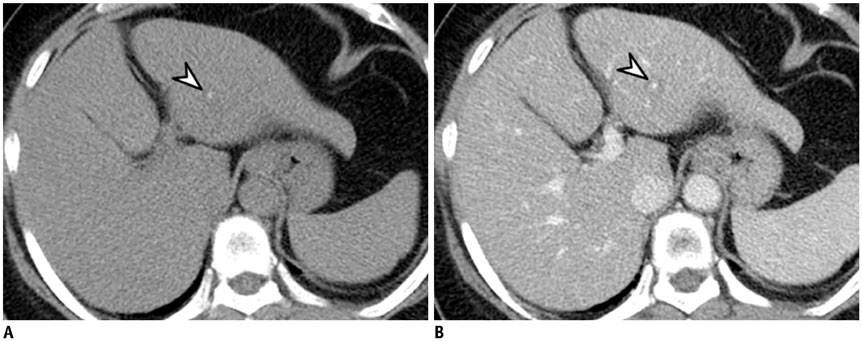
Fig. 10 Hepatic metastasis from breast cancer in 60-year-old female. A, B. Small low-attenuated lesion with tiny calcification (arrowheads) is noted in left lateral section of liver. Metastatic tumor from breast cancer was confirmed via percutaneous biopsy.

Fig. 11 Hepatic metastases from colon cancer in 60-year-old female. A. Multiple low-attenuated metastases (arrows) are located in both liver lobes on axial contrast-enhanced CT image. B. On follow-up CT image taken after patient underwent chemotherapy, multiple previous metastases are decreased in size, and amorphous intratumoral calcification (arrowhead) is newly developed.

Fig. 12 Hepatic hemangiomas in 67-year-old female. A, B. There are two small hemangiomas (arrows) in left lobe of liver. On axial pre-contrast CT scan (A), small punctate calcification (arrowhead), known as phlebolith, is seen at small hemangioma (arrows) in left lateral section. Although dynamic contrast-enhanced CT that showed typical progressive centripetal enhancement is not seen, hemangiomas (arrows) show peripheral nodular enhancement and punctate calcification on axial portal venous phase image (B).
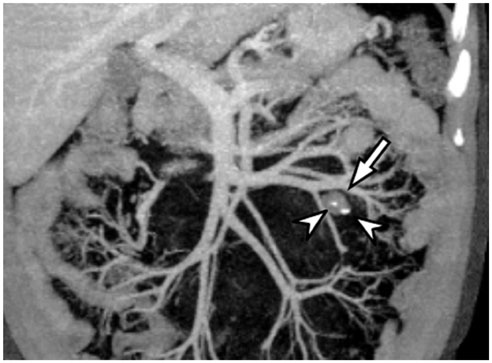
Fig. 13 Mesenteric hemangioma in 47-year-old male. On coronal, maximum-intensity projection CT image, small, round, soft tissue lesion is found in left-sided small bowel mesentery (arrow). Two small punctate calcifications (arrowheads) are seen within lesion. After mass excision, this lesion was confirmed as being mesenteric hemangioma.
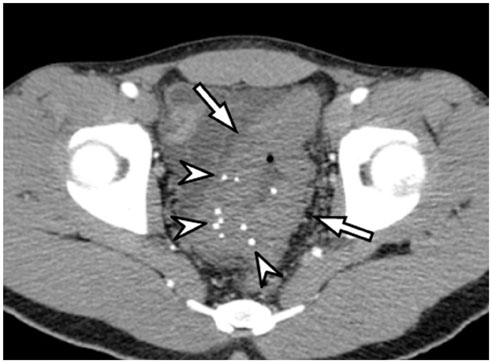
Fig. 14 Sigmoid colon hemangioma in 22-year-old male. Axial contrast-enhanced CT image demonstrates segmental concentric bowel wall thickening (arrows) with multiple punctate calcifications (arrowheads, phleboliths) involving sigmoid colon. This multiple punctate calcification pattern is characteristic imaging feature of gastrointestinal hemangioma.
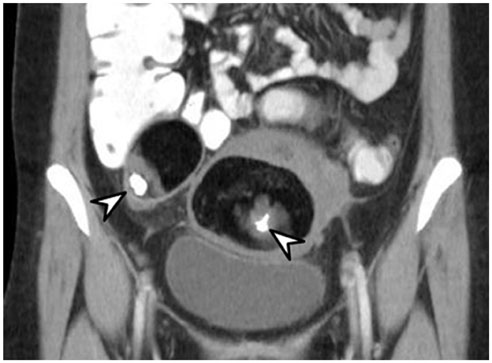
Fig. 15 Mature cystic teratomas in 40-year-old female. On coronal contrast-enhanced CT image, bilateral ovarian fatty masses containing punctate calcification (arrowheads) are visible. These are pathognomonic radiologic findings of mature cystic teratoma.

Fig. 16 Mature cystic teratomas in 55-year-old female. Bilateral mature cystic teratomas are found on axial pre-contrast CT image. In left mature cystic teratoma, presence of peripheral, thick, rim calcification (arrow) and central punctate calcification (arrowhead) are simultaneously noted. Right mature cystic teratoma contains single punctate calcification (arrowhead).
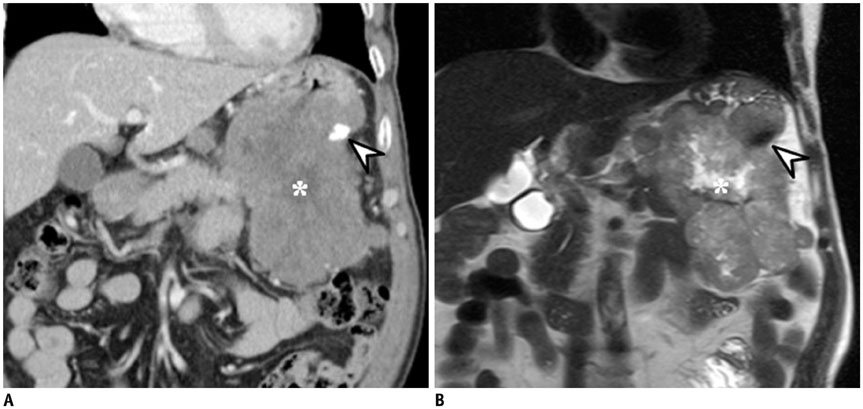
Fig. 17 Gastrointestinal stromal tumor in 61-year-old male. A. Exophytic lobulating contoured enhancing mass is seen in stomach high-body greater curvature on coronal contrast-enhanced CT image. Mass contains small, dense punctate calcification (arrowhead) and internal, low-density necrotic portion (asterisk). B. On coronal T2-weighted MR image, small dense punctate calcification (arrowhead) is seen as region of hyposignal intensity. Internal necrotic portion (asterisk) within mass appears as region of high signal intensity. Gastrointestinal stromal tumor was confirmed.
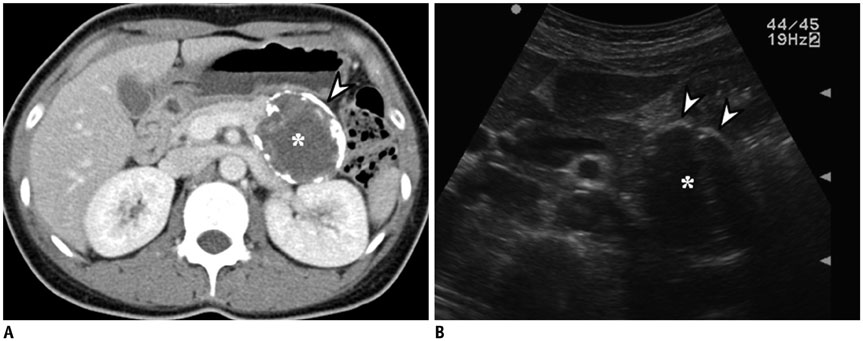
Fig. 18 Solid pseudopapillary neoplasm of pancreas in 28 year-old female. A. On axial contrast-enhanced CT image, low density mass (asterisk) with thick peripheral, rim calcification (arrowhead) is located in pancreatic tail. Main pancreatic duct is not dilated. B. On ultrasound scan, bulging contoured mass (asterisk) is suspected in pancreatic tail. Peripheral, rim calcification (arrowheads) of mass appears as hyperechogenicity with posterior acoustic presentation. Solid pseudopapillary neoplasm was diagnosed after distal pancreatectomy.
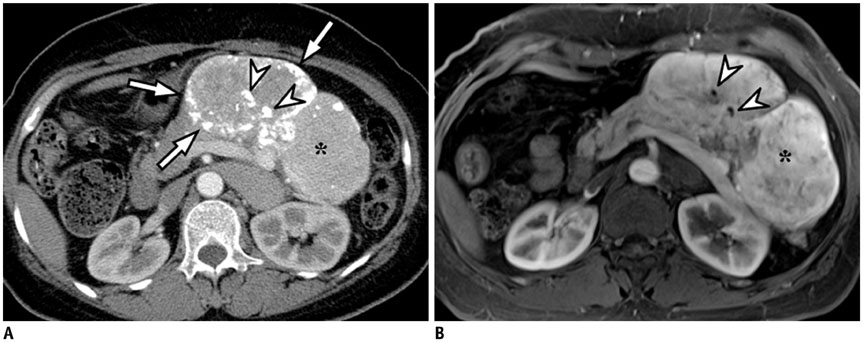
Fig. 19 Pancreatic neuroendocrine tumor in 54-year-old female. A. On axial contrast-enhanced CT image, large lobulating contoured hypervascular mass (asterisk) is located in pancreatic tail. Lesion contains multiple amorphous calcifications (arrows and arrowheads) at central and peripheral portions of mass. B. On contrast-enhanced T1-weighted image, dense calcifications (arrowheads) appear as dark signal intensity at center of mass (asterisk). However, other peripheral amorphous calcifications (arrows on A) are not clearly visualized. This mass was confirmed as neuroendocrine tumor (grade 2) after distal pancreatectomy.

Fig. 20 Multiple schwannomas in 39-year-old female. Coronal contrast-enhanced CT image demonstrates multiple round masses (asterisks) in retroperitoneum, which are confirmed as schwannomas. Punctate and curvilinear calcifications (arrowheads) are seen in some tumors.

Fig. 21 Castleman disease in 30-year-old male. A. On coronal contrast-enhanced CT image, well-defined hypervascular retroperitoneal mass (asterisk) is found. Multiple amorphous calcifications (arrowheads) are noted within mass. B. On ultrasound scan, well-defined hypoechoic mass (asterisk) is revealed. Multiple intratumoral calcifications (arrowheads) are seen as echogenic portions with or without posterior acoustic shadowing. After mass excision, lesion was confirmed as Castleman disease.
Cited by 1 articles
-
Imaging Evaluation Following 90Y Radioembolization of Liver Tumors: What Radiologists Should Know
Ijin Joo, Hyo-Cheol Kim, Gyoung Min Kim, Jin Chul Paeng
Korean J Radiol. 2018;19(2):209-222. doi: 10.3348/kjr.2018.19.2.209.
Reference
-
1. Curry CA, Eng J, Horton KM, Urban B, Siegelman S, Kuszyk BS, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol. 2000; 175:99–103.2. Ko EY, Ha HK, Kim AY, Yoon KH, Yoo CS, Kim HC, et al. CT differentiation of mucinous and nonmucinous colorectal carcinoma. AJR Am J Roentgenol. 2007; 188:785–791.3. Paley MR, Ros PR. Hepatic calcification. Radiol Clin North Am. 1998; 36:391–398.4. Izawa N, Sawada T, Abiko R, Kumon D, Hirakawa M, Kobayashi M, et al. Gastrointestinal stromal tumor presenting with prominent calcification. World J Gastroenterol. 2012; 18:5645–5648.5. Baek JH, Lee JM, Kim SH, Kim SJ, Kim SH, Lee JY, et al. Small (<or=3 cm) solid pseudopapillary tumors of the pancreas at multiphasic multidetector CT. Radiology. 2010; 257:97–106.6. Giachelli CM. Ectopic calcification: gathering hard facts about soft tissue mineralization. Am J Pathol. 1999; 154:671–675.7. Agarwal A, Yeh BM, Breiman RS, Qayyum A, Coakley FV. Peritoneal calcification: causes and distinguishing features on CT. AJR Am J Roentgenol. 2004; 182:441–445.8. Leyendecker JR, Tchelepi H. Lesion composition. In : Dalrymple NC, Leyendecker JR, Oliphant M, editors. Problem solving in abdominal imaging. 1st ed. Philadephia: Elsevier;2009. p. e1–e20.9. Wu Z, Mittal S, Kish K, Yu Y, Hu J, Haacke EM. Identification of calcification with MRI using susceptibility-weighted imaging: a case study. J Magn Reson Imaging. 2009; 29:177–182.10. Roy B, Verma S, Awasthi R, Rathore RK, Venkatesan R, Yoganathan SA, et al. Correlation of phase values with CT Hounsfield and R2* values in calcified neurocysticercosis. J Magn Reson Imaging. 2011; 34:1060–1064.11. Rahmouni A, Bargoin R, Herment A, Bargoin N, Vasile N. Color Doppler twinkling artifact in hyperechoic regions. Radiology. 1996; 199:269–271.12. Kim HC, Yang DM, Jin W, Ryu JK, Shin HC. Color Doppler twinkling artifacts in various conditions during abdominal and pelvic sonography. J Ultrasound Med. 2010; 29:621–632.13. Sarmiento de la Iglesia MM, Lecumberri Cortés G, Lecumberri Cortés I, Oleaga Zufiria L, Isusi Fontan M, Grande Icaran D. [Intracranial calcifications on MRI]. Radiologia. 2006; 48:19–26.14. Hu B, El Hajj N, Sittler S, Lammert N, Barnes R, Meloni-Ehrig A. Gastric cancer: classification, histology and application of molecular pathology. J Gastrointest Oncol. 2012; 3:251–261.15. Park MS, Yu JS, Kim MJ, Yoon SW, Kim SH, Noh TW, et al. Mucinous versus nonmucinous gastric carcinoma: differentiation with helical CT. Radiology. 2002; 223:540–546.16. Ghahremani GG, Meyers MA, Port RB. Calcified primary tumors of the gastrointestinal tract. Gastrointest Radiol. 1978; 2:331–339.17. Stoupis C, Taylor HM, Paley MR, Buetow PC, Marre S, Baer HU, et al. The Rocky liver: radiologic-pathologic correlation of calcified hepatic masses. Radiographics. 1998; 18:675–685. quiz 726.18. Bosman FT, Cameron JL, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press;2010. p. 217–224. p. 236–238. p. 254–261.19. Kim HJ, Yu ES, Byun JH, Hong SM, Kim KW, Lee JS, et al. CT differentiation of mucin-producing cystic neoplasms of the liver from solitary bile duct cysts. AJR Am J Roentgenol. 2014; 202:83–91.20. Farrell JJ. Prevalence, diagnosis and management of pancreatic cystic neoplasms: current status and future directions. Gut Liver. 2015; 9:571–589.21. Buetow PC, Rao P, Thompson LD. From the Archives of the AFIP. Mucinous cystic neoplasms of the pancreas: radiologic-pathologic correlation. Radiographics. 1998; 18:433–449.22. Sahani DV, Kadavigere R, Saokar A, Fernandez-del Castillo C, Brugge WR, Hahn PF. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. Radiographics. 2005; 25:1471–1484.23. Lee NK, Kim S, Kim HS, Jeon TY, Kim GH, Kim DU, et al. Spectrum of mucin-producing neoplastic conditions of the abdomen and pelvis: cross-sectional imaging evaluation. World J Gastroenterol. 2011; 17:4757–4771.24. Qian LJ, Zhu J, Zhuang ZG, Xia Q, Liu Q, Xu JR. Spectrum of multilocular cystic hepatic lesions: CT and MR imaging findings with pathologic correlation. Radiographics. 2013; 33:1419–1433.25. Buetow PC, Buck JL, Pantongrag-Brown L, Ros PR, Devaney K, Goodman ZD, et al. Biliary cystadenoma and cystadenocarcinoma: clinical-imaging-pathologic correlations with emphasis on the importance of ovarian stroma. Radiology. 1995; 196:805–810.26. Pickhardt PJ, Levy AD, Rohrmann CA Jr, Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics. 2003; 23:645–662.27. Carr N, Sobin L. Tumors of the appendix. In : Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press;2010. p. 122–125.28. Tirumani SH, Fraser-Hill M, Auer R, Shabana W, Walsh C, Lee F, et al. Mucinous neoplasms of the appendix: a current comprehensive clinicopathologic and imaging review. Cancer Imaging. 2013; 13:14–25.29. Madwed D, Mindelzun R, Jeffrey RB Jr. Mucocele of the appendix: imaging findings. AJR Am J Roentgenol. 1992; 159:69–72.30. Persaud T, Swan N, Torreggiani WC. Giant mucinous cystadenoma of the appendix. Radiographics. 2007; 27:553–557.31. Hale HL, Husband JE, Gossios K, Norman AR, Cunningham D. CT of calcified liver metastases in colorectal carcinoma. Clin Radiol. 1998; 53:735–741.32. Easson AM, Barron PT, Cripps C, Hill G, Guindi M, Michaud C. Calcification in colorectal hepatic metastases correlates with longer survival. J Surg Oncol. 1996; 63:221–225.33. Caseiro-Alves F, Brito J, Araujo AE, Belo-Soares P, Rodrigues H, Cipriano A, et al. Liver haemangioma: common and uncommon findings and how to improve the differential diagnosis. Eur Radiol. 2007; 17:1544–1554.34. Vilgrain V, Boulos L, Vullierme MP, Denys A, Terris B, Menu Y. Imaging of atypical hemangiomas of the liver with pathologic correlation. Radiographics. 2000; 20:379–397.35. Klotz T, Montoriol PF, Da Ines D, Petitcolin V, Joubert-Zakeyh J, Garcier JM. Hepatic haemangioma: common and uncommon imaging features. Diagn Interv Imaging. 2013; 94:849–859.36. Mitsudo K, Watanabe Y, Saga T, Dohke M, Sato N, Minami K, et al. Nonenhanced hepatic cavernous hemangioma with multiple calcifications: CT and pathologic correlation. Abdom Imaging. 1995; 20:459–461.37. Djouhri H, Arrivé L, Bouras T, Martin B, Monnier-Cholley L, Tubiana JM. Diffuse cavernous hemangioma of the rectosigmoid colon: imaging findings. J Comput Assist Tomogr. 1998; 22:851–855.38. Yoo S. GI-associated hemangiomas and vascular malformations. Clin Colon Rectal Surg. 2011; 24:193–200.39. Levy AD, Abbott RM, Rohrmann CA Jr, Frazier AA, Kende A. Gastrointestinal hemangiomas: imaging findings with pathologic correlation in pediatric and adult patients. AJR Am J Roentgenol. 2001; 177:1073–1081.40. Hsu RM, Horton KM, Fishman EK. Diffuse cavernous hemangiomatosis of the colon: findings on three-dimensional CT colonography. AJR Am J Roentgenol. 2002; 179:1042–1044.41. Outwater EK, Siegelman ES, Hunt JL. Ovarian teratomas: tumor types and imaging characteristics. Radiographics. 2001; 21:475–490.42. Park SB, Kim JK, Kim KR, Cho KS. Imaging findings of complications and unusual manifestations of ovarian teratomas. Radiographics. 2008; 28:969–983.43. Jung SE, Lee JM, Rha SE, Byun JY, Jung JI, Hahn ST. CT and MR imaging of ovarian tumors with emphasis on differential diagnosis. Radiographics. 2002; 22:1305–1325.44. Guinet C, Ghossain MA, Buy JN, Malbec L, Hugol D, Truc JB, et al. Mature cystic teratomas of the ovary: CT and MR findings. Eur J Radiol. 1995; 20:137–143.45. Buy JN, Ghossain MA, Moss AA, Bazot M, Doucet M, Hugol D, et al. Cystic teratoma of the ovary: CT detection. Radiology. 1989; 171:697–701.46. Friedman AC, Pyatt RS, Hartman DS, Downey EF Jr, Olson WB. CT of benign cystic teratomas. AJR Am J Roentgenol. 1982; 138:659–665.47. Saba L, Guerriero S, Sulcis R, Virgilio B, Melis G, Mallarini G. Mature and immature ovarian teratomas: CT, US and MR imaging characteristics. Eur J Radiol. 2009; 72:454–463.48. Moon W, Kim Y, Rhim H, Koh B, Cho O. Coexistent cystic teratoma of the omentum and ovary: report of two cases. Abdom Imaging. 1997; 22:516–518.49. Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics. 2003; 23:283–304. 456quiz 532.50. Miettinen M, Lasota J. Gastrointestinal stromal tumors: pathology and prognosis at different sites. Semin Diagn Pathol. 2006; 23:70–83.51. Ghanem N, Altehoefer C, Furtwängler A, Winterer J, Schäfer O, Springer O, et al. Computed tomography in gastrointestinal stromal tumors. Eur Radiol. 2003; 13:1669–1678.52. Tateishi U, Hasegawa T, Satake M, Moriyama N. Gastrointestinal stromal tumor. Correlation of computed tomography findings with tumor grade and mortality. J Comput Assist Tomogr. 2003; 27:792–798.53. Kim HC, Lee JM, Choi SH, Kim KW, Kim SH, Lee JY, et al. Imaging of gastrointestinal stromal tumors. J Comput Assist Tomogr. 2004; 28:596–604.54. Law JK, Ahmed A, Singh VK, Akshintala VS, Olson MT, Raman SP, et al. A systematic review of solid-pseudopapillary neoplasms: are these rare lesions? Pancreas. 2014; 43:331–337.55. Choi JY, Kim MJ, Kim JH, Kim SH, Lim JS, Oh YT, et al. Solid pseudopapillary tumor of the pancreas: typical and atypical manifestations. AJR Am J Roentgenol. 2006; 187:W178–W186.56. Buetow PC, Buck JL, Pantongrag-Brown L, Beck KG, Ros PR, Adair CF. Solid and papillary epithelial neoplasm of the pancreas: imaging-pathologic correlation on 56 cases. Radiology. 1996; 199:707–711.57. Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, Caplin ME, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut. 2012; 61:6–32.58. Sahani DV, Bonaffini PA, Fernández-Del Castillo C, Blake MA. Gastroenteropancreatic neuroendocrine tumors: role of imaging in diagnosis and management. Radiology. 2013; 266:38–61.59. Heller MT, Shah AB. Imaging of neuroendocrine tumors. Radiol Clin North Am. 2011; 49:529–548. vii60. Lewis RB, Lattin GE Jr, Paal E. Pancreatic endocrine tumors: radiologic-clinicopathologic correlation. Radiographics. 2010; 30:1445–1464.61. Buetow PC, Parrino TV, Buck JL, Pantongrag-Brown L, Ros PR, Dachman AH, et al. Islet cell tumors of the pancreas: pathologic-imaging correlation among size, necrosis and cysts, calcification, malignant behavior, and functional status. AJR Am J Roentgenol. 1995; 165:1175–1179.62. Poultsides GA, Huang LC, Chen Y, Visser BC, Pai RK, Jeffrey RB, et al. Pancreatic neuroendocrine tumors: radiographic calcifications correlate with grade and metastasis. Ann Surg Oncol. 2012; 19:2295–2303.63. Kim DW, Kim HJ, Kim KW, Byun JH, Song KB, Kim JH, et al. Neuroendocrine neoplasms of the pancreas at dynamic enhanced CT: comparison between grade 3 neuroendocrine carcinoma and grade 1/2 neuroendocrine tumour. Eur Radiol. 2015; 25:1375–1383.64. Low G, Panu A, Millo N, Leen E. Multimodality imaging of neoplastic and nonneoplastic solid lesions of the pancreas. Radiographics. 2011; 31:993–1015.65. Rha SE, Byun JY, Jung SE, Chun HJ, Lee HG, Lee JM. Neurogenic tumors in the abdomen: tumor types and imaging characteristics. Radiographics. 2003; 23:29–43.66. Kim TJ, Han JK, Kim YH, Kim TK, Choi BI. Castleman disease of the abdomen: imaging spectrum and clinicopathologic correlations. J Comput Assist Tomogr. 2001; 25:207–214.67. Ko SF, Hsieh MJ, Ng SH, Lin JW, Wan YL, Lee TY, et al. Imaging spectrum of Castleman's disease. AJR Am J Roentgenol. 2004; 182:769–775.68. Bonekamp D, Horton KM, Hruban RH, Fishman EK. Castleman disease: the great mimic. Radiographics. 2011; 31:1793–1807.69. Meador TL, McLarney JK. CT features of Castleman disease of the abdomen and pelvis. AJR Am J Roentgenol. 2000; 175:115–118.70. Hill AJ, Tirumani SH, Rosenthal MH, Shinagare AB, Carrasco RD, Munshi NC, et al. Multimodality imaging and clinical features in Castleman disease: single institute experience in 30 patients. Br J Radiol. 2015; 88:20140670.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Analysis of Intratumoral Gas Formation after Hepatic Tumor Embolization
- Imaging Findings of Pediatric Oligodendroglioma
- Multifocal Peritoneal Splenosis in Tc-99m-Labeled Heat-Denatured Red Blood Cell Scintigraphy
- Radiological observation of determination of sex by costal cartilage calcification
- Chondrosarcoma with Intratumoral Hemorrhage: Case Report
